Acute Skin Failure
Dermatological Emergencies Dr Sami Fatehi MBBS, MSc, MD, PhD
Objectives
- By the end of this lecture you should be able to:
- Find out clues to the presence of a potential dermatologic emergency
- Define and identify the underlying pathophysiology consequences of the acute skin failure
- Manage patient with dermatologic emergencies
Introduction
About 15-20 % of visits to primary care physicians and emergency departments are due to dermatologic complaints
How to differentiate simple skin conditions from the more serious, life threatening conditions that require immediate intervention ?
Clues to the Presence of a Potential Dermatologic Emergency
- Fever and rash
- Fever and blisters or denuding skin
- Rash in immunocompromised
- Palpable purpura
- Full body redness
Definition of Acute Skin Failure
Is a failure of skin functions mainly due de novo skin disease.
What are Skin functions?
- barrier
- temperature regulation
- immunological function
- …
- …
- …
Causes of Acute Skin Failure
Steven Jonson syndrome Acute generalized Pusular psoriasis Immunobolous disorders (Pemphigus vulgaris) Erythroderma Infections → staphylococcal scalded skin syndrome , febrile viral exanthemas
Erythroderma


Steven Johnson Syndrome (SJS)



Pemphigus Vulgaris (PV)

Generalized Pustular Psoriasis (GPP)

Staphylococcal Scalded Skin Syndrome (SSSS)

Consequences of Acute Skin Failure
1. Hemodynamic Alteration
- Persistent inflammation of the skin →
- marked peripheral vasodilatation and increased cutaneous blood flow(erythema and edema)
- increased blood volume and cardiac output→
- high-output cardiac failure.
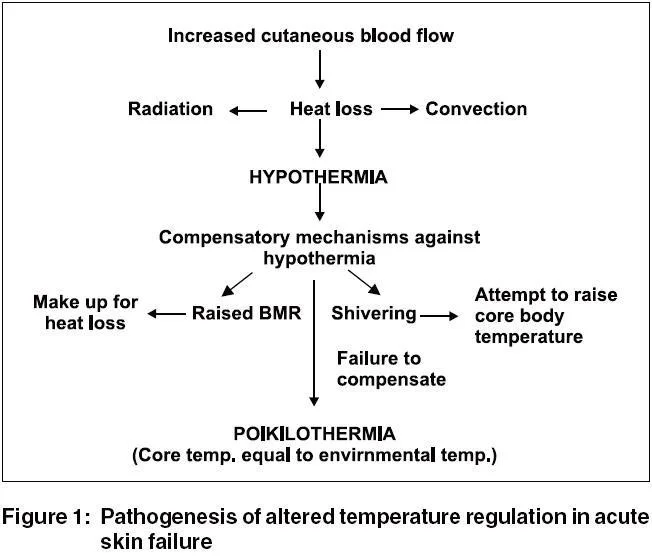
2. Thermoregulation Disturbance
Hypothermia is a very common and its sudden onset is a sign of septic shock.
Fever may be present in the absence of infection due to sweat ducts occlusion
Figure 1: Pathogenesis of altered temperature regulation in acute skin failure
3. Metabolic Disturbance
- High basal metabolic rate (BMR) increases energy consuming
- A hyperglycemic state and glycosuria due to associated pancreatitis
- Pancreatitis lead to decrease insulin secretion → enhances caloric loss by depleting tissue protein as an energy source.
- Patient shivers → is also highly energy consuming.
4. Fluid and Electrolyte Imbalance
In patients with acute skin failure, the daily transepidermal water loss is very high ⇒ May reaches 3-4 liters in patient who is 50% of body surface area involved.
Hyponatreamia, Hypophosphatemia and hyperkalaemia are common. ⇒ Leads to neurologic disturbances and diaphragmatic disturbances and respiratory failure
5. Altered Immune Function Associated with TEN:
- Lymphopenia
- Neutropenia
- Thrombocytopenia
- Impaired chemotaxis and phagocytosis of granulocytes
- Hypo-gammaglobulinemia
6. Infection
- The incidence of septic complications is increased in the presence of altered body defense mechanisms
- Damaged barrier function of the skin facilitates colonization and systemic entry of commensal, exogenous and endogenous (gut flora) microorganisms.
Care of Patients with Acute Skin Failure
- Treat patient with acute skin failure as severe burned patient.
- Use role of nine to estimate the affected body surface area to calculate the fluid replacement
- Assessment of the severity of the disease helps in planning the management.
The Pillars cycle in the Management of Such Patients Are:
- Nursing care
- Monitoring hemodynamic changes
- Fluid, electrolyte balance and nutrition
- Prevention of complication (e.g. sepsis)
- identification of risk factors
- Topical therapy.