Urticaria (hives)
Dr Sami Aldaham
Goals and Objectives
- You have to be able to
- Describe the morphology of urticaria
- Distinguish between acute and chronic urticaria
Urticaria
- Urticaria (hives) is a vascular reaction of the skin characterized by wheals surrounded by a red halo or flare (area of erythema)
- Cardinal symptom is PRURITUS (itch)
- Urticaria = pruritus
- Urticaria is caused by swelling of the upper dermis
- Up to 20% of the population experience urticaria at some point in their lives
Angioedema
-
Angioedema can be caused by the same pathogenic mechanisms as urticaria
-
The pathology is in the deep dermis and subcutaneous tissue and swelling is the major manifestation
-
Angioedema commonly affects the face or a portion of an extremity
-
Involvement of the lips, cheeks, and periorbital areas is common, but angioedema also may affect the tongue, pharynx, larynx and bowels.
-
May be painful or burning, but not pruritic
-
May last several days
Examples of Urticaria


Example of Angioedema

Urticaria & Angioedema
- Urticaria and angioedema may occur in any location together or individually.
- Angioedema and/or urticaria may be the cutaneous presentation of anaphylaxis, so assessment of the respiratory and cardiovascular systems is vital.
Clinical Findings
- Lesions typically appear over the course of minutes, enlarge, and then disappear within hours
- Individual wheals rarely last >12hrs
- Surrounding erythema will blanch with pressure
Clinical Classification
- Acute urticaria = new onset urticaria < 6 weeks
- Chronic urticaria = recurrent urticaria (most days) > 6 weeks
Common Causes of Acute Urticaria
- Idiopathic
- Food reactions: Shellfish, nuts, fruit
- Infections: Upper respiratory, streptococcal infections, helminthes
- Drug reactions
- IV administration
- Blood products, contrast agents
Etiology of Chronic Urticaria
- Idiopathic: over 50% of chronic urticaria RR
- Physical urticarias: many patients with chronic urticaria have physical factors that contribute to their urticaria
- These factors include pressure, cold, heat, water (aquagenic), sunlight (solar), vibration, and exercise
- Cholinergic urticaria is triggered by heat and emotion
- The diagnosis of pure physical urticaria is made when the sole cause of a patient’s urticaria is a physical factor
- Chronic autoimmune: possibly a third or more of patients with chronic urticaria
- Other: infections, ingestions, medications
Dermatographism
- Most common form of physical urticaria
- Sharply localized
- edema or wheal
- within seconds to minutes after the skin has been rubbed
 #ospe
#ospe
Pathophysiology
- Immunologic mediated urticaria
- The mast cell is the major effector cell in urticaria
- Non – immunologic mediated urticaria
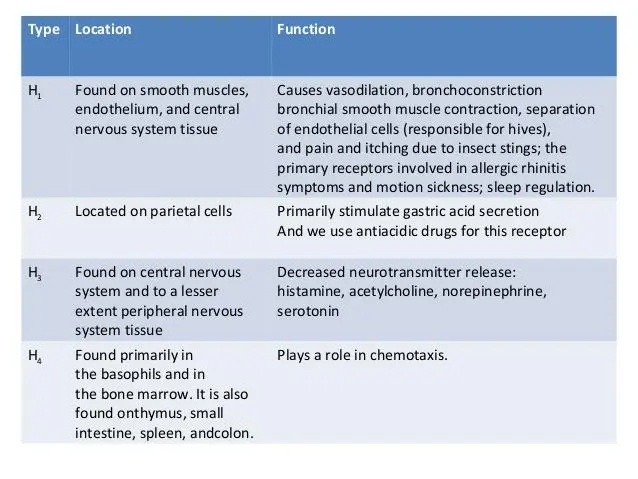
1- Immunologic Urticaria
- Antigen binds to IgE on the mast cell ⇒
- Mast cell degranulation ⇒
- histamine releasing ⇒
- Histamine binds to H1 and H2 receptors to cause arteriolar dilatation ⇒
- venous constriction ⇒
- increased capillary permeability.
2- Non-Immunologic Urticaria: Not dependent on the binding of IgE receptors
- Some drugs (aspirin) ⇒
- Unknown: pharmacologic mechanism ⇒
- Affect the arachidonic acid metabolism ⇒
- release of histamine from mast cells.
3- Physical stimuli
- Physical stimuli
- direct mast cell degranulation
- Induced histamine release
DIAGNOSIS
-
Urticaria is a clinical diagnosis
-
A detailed history and physical exam should be performed
-
Many times patients will not present with urticaria during their clinic visit
-
show patients photographs of urticaria and ask if their lesions appear similar
-
Ask patients to take photos of their lesions / bring them to their office visit
Allergy Testing
-
Allergy testing is not routinely performed in patients with chronic urticaria.
-
Skin prick testing may reveal sensitivities to a variety of allergens that may not be .relevant to the patient’s urticaria
Natural History and Prognosis
-
In most patients, chronic urticaria is an episodic and self-limited disorder
-
Average duration of disease is two to five years
-
Symptoms of chronic urticaria can be severe and impair the patient’s quality of life (QOL)
Treatment
Antihistamines
Oral H1 antihistamines are the first-line treatment for acute and chronic urticaria
-
First-generation H1 antihistamines are less well-tolerated due to sedation used also in atopic dermatitis
-
Second-generation H1 long acting antihistamines are well tolerated with fewer sedative and anticholinergic effects

The following are examples of H₁ antihistamines: 1st Generation
- Diphenhydramine (OTC)
- Hydroxyzine (Rx,generic)
- Chlorpheniramine (OTC)
2nd Generation
- Cetirizine (OTC)
- Loratadine (OTC)
- Fexofenadine (OTC)
Referral to Dermatologist and indication of skin biopsy
Biopsy should be performed in patients with one or more of the following features:
- Individual lesions that persist beyond 48 hours, are painful rather than pruritic, or have accompanying petechial characteristics
- Systemic symptoms
- Lack of response to antihistamines
- Lesions that leave pigmentation changes upon resolution
Take Home Points
- Urticaria (hives) is a vascular reaction of the skin characterized by wheals surrounded by a red halo or flare.
- Urticaria is classified as acute or chronic. Acute urticaria is defined as periodic outbreaks of urticarial lesions that resolve within six weeks.
- Over 50% of chronic urticaria is idiopathic.
- Oral H1 antihistamines are first-line treatment for acute and chronic urticaria.
- 1st generation H1 antihistamines can cause sedation.
- The presence of systemic symptoms should signal the possibility that an urticarial rash is not ordinary urticaria.
Urticaria
Characteristics and Causes
- Time to onset: immediate, accelerated (hours), or delayed (days).
- Type I hypersensitivity reactions: antibiotics (cephalosporins, and sulfonamides), local anesthetics, radiocontrast media, blood products, and gamma globulin.
- Non-immune urticaria: radiocontrast media and long-acting ACE-inhibitors (due to changes in vascular response to bradykinin).
- Mast cell degranulation by non-IgE mechanisms: opiate analgesics, anesthetic muscle relaxants, and Vancomycin (Red Man Syndrome, which can be worsened by concommitant opiate use).
