Vitiligo
Dr Sami Aldaham
Introduction
-
Vitiligo is a common acquired disorder.
-
Characterized by well-marginated white spots resulting from loss of melanocytes.
-
Vitiligo is associated with some autoimmune disorders.
-
Is associated with social stigma.
-
Confusion with leprosy is partly responsible for this.
Aetiology & Pathogenesis
-
Susceptibility to the disease may be inherited.
-
1/4 to 1/3 of patients have family members affected with the disease.
-
A multifactorial pattern of inheritance is revealed in most studies.
-
There are three possible mechanisms that may cause destruction of melanocytes.
-
However, multiple mechanisms may be responsible for the causation of vitiligo in an individual.
The three possible mechanisms of vitiligo
-
The autoimmune hypothesis
- Originated from the observation that vitiligo is associated with some autoimmune diseases.
- Suggets that there is an autoimmune damage to melanocytes.
-
The autocytotoxic or self-destruct hypothesis
- Suggests that some toxic molecules produced during the biosynthesis of melanin are responsible for melanocyte damage in susceptible individuals.
-
The neural hypothesis
- Postulates that neurochemicals liberated from nerve endings are toxic to melanocytes.
Clinical Features
-
Vitiligo affects all races with an average frequency of 1% to 2% of the population.
-
Both sexes are affected equally.
-
The disease may develop at any age, the peak age of onset is between 10 and 30 years.
-
Stressful life events or physical trauma can often precipitate the onset of disease.
-
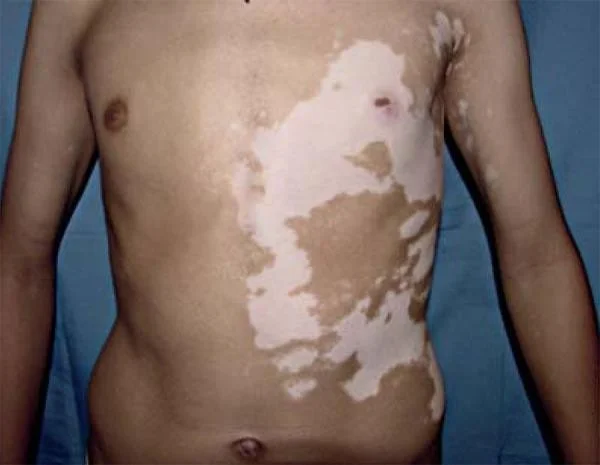
Typically, macule of vitiligo is well-circumscribed depigmented of varying sizes.
-
The hairs on the patch may turn grey.
-
There may be a single or numerous depigmented macules distributed all over the body.
-
With time, the macules may enlarge and coalesce to produce extensive pigment loss.
-
The lesions are asymptomatic.
Clinical types
- According to:
- The extent of involvement
- Pattern of distribution
Is clinically categorized into the following types:
- Focal vitiligo
- Is an isolated macule or a few macules in a localized non-dermatomal distribution.

- Segmental vitiligo
- Is characterized by macules in a unilateral dermatomal distribution.


- Generalized vitiligo - patches generally
- Is the most common type showing macules in a generalized widespread distribution.
- There is often symmetry of affection.
- Sites: Face (particularly around the orifices), neck, bony prominences of hands, legs, axillae and mucosal surfaces are particularly affected.



- Acro-facial vitiligo
- Affects distal end of fingers and facial orifices.



- Universal Vitiligo - 80% body surfaces
- Implies loss of pigment over the entire body surface area with only isolated islands of normal pigmentation remaining.
Associated diseases
- Patients with vitiligo have an increased risk of developing autoimmune diseases like:
- Alopecia areata
- Thyroid diseases
- Addison’s disease
- Pernicious anaemia
- Insulin-dependent diabetes mellitus.
Psychosocial impact of vitiligo
- Although vitiligo by itself is asymptomatic and does not cause any physical discomfort or disability.
- It may be associated with devastating psychological and social consequences.
- Feeling of stress and embarrassment on social contacts, lowered self-esteem may be detrimental to the patients, particularly when the lesions are on visible area of the body.
Treatment
- With treatment, re-pigmentation occurs around the hair follicles, which is achieved by stimulation and migration of follicular melanocytes.
- Spread of pigmentation from the margin of the patch can also occur.
- Whatever the mode of therapy, patient education and reassurance is very importance.
- Explanation of the benign nature of the disease and psychological support is needed in all patients.
1- Topical steroids
- Are effective in the management of disease limited to small area.
- Lesions on face and neck respond better than other parts or the body. Hydrocortisone is the topical agent of choice.
- More potent steroids can also be used intermittently.
2- PUVA therapy
- PUVA therapy (Psoralen + Ultraviolet A) is the mainstay of management of vitiligo.
- Topical PUVA involves painting the area with psoralen solution and exposing the area to UVA.
- Patients with limited involvement are best suited for this mode of therapy.
- Is used in patients with extensive vitiligo.
- Is avoided in children below the age of 12.
- It is contraindicated in pregnancy and lactation.
3-Surgical treatment
- When topical steroids or PUVA therapy fails to repigment, surgical treatment may be undertaken such as skin graft, melanocyte transplant
- Best suited for segmental and localized vitiligo.
3- Depigmentation
- In patients with extensive vitiligo.
- Depigmentation of the remaining islands of normal skin may be more cosmetically acceptable.
- To achieve this, hydroquinone in a concentration of 20% is applied twice a day on the pigmented skin.
- It may take months to establish depigmentation, which is usually permanent.