Pediatrics
Definition and Etiology
Epiglottitis is the inflammation of the epiglottis and adjacent supraglottic structures, primarily due to infection. Without treatment, it can progress to life-threatening airway obstruction.
Etiologies:
- Infectious:
- Haemophilus influenzae type b (Hib): Despite a rapid decline in the post-conjugate vaccine era, Hib remains an important etiology, primarily in unvaccinated or incompletely immunized children.
- Streptococcus pyogenes (Group A Strep)
- Streptococcus pneumoniae
- Staphylococcus aureus
- Non-infectious: Caustic ingestion, thermal injury, and local trauma.
Infectious Pathogens
| Category | Pathogens |
|---|---|
| Bacterial | Haemophilus influenzae (Hib, types A, F, and nontypeable strains), Haemophilus parainfluenzae, Streptococcus pneumoniae, Staphylococcus pneumoniae, Staphylococcus aureus (methicillin susceptible and methicillin resistant), Beta-hemolytic streptococci (Groups A, B, C, F, G), Pasteurella multocida, Moraxella catarrhalis, Klebsiella pneumoniae, Neisseria meningitidis and other Neisseria species, Escherichia coli, Enterobacter cloacae, Pseudomonas aeruginosa* |
| Viral | Herpes simplex virus (types 1 and 2), Varicella zoster virus (VZV), Parainfluenza virus type 3, Influenza (types A and B), Epstein-Barr virus (EBV), SARS-CoV-2, HIV |
| Fungal | Candida albicans* |
*Candidal and pseudomonal epiglottitis usually occur in immunocompromised patients. †Epiglottitis may result from bacterial superinfection.
 “
“
Clinical Presentation
- Hallmarks: Abrupt onset and rapid progression (within hours).
- Appearance: Toxic appearance and distress (agitation, restlessness, irritability).
- Fever: Sudden onset of high fever (between 38.8 and 40.0°C).
- Classic Signs: Stridor, Drooling, Dysphagia, Distress, Change in voice (muffled, “hot potato” voice).
- Postures:
- Tripod Posture: Sitting forward with the trunk leaning forward, neck hyperextended, and chin thrust forward.
- Sniffing Posture: Attempting to maximize the diameter of the obstructed airway.
- Reluctance: Children may be reluctant to lie down.
- Absence of: Hoarseness or barking cough (which are more characteristic of croup).
- Older Patients: Adolescents and adults may present with severe sore throat, dysphagia, and drooling; a relatively normal oropharyngeal exam; and minimal respiratory distress.



Tripod positioning and sniffing position. Note the anxious and toxic appearance.
Diagnosis
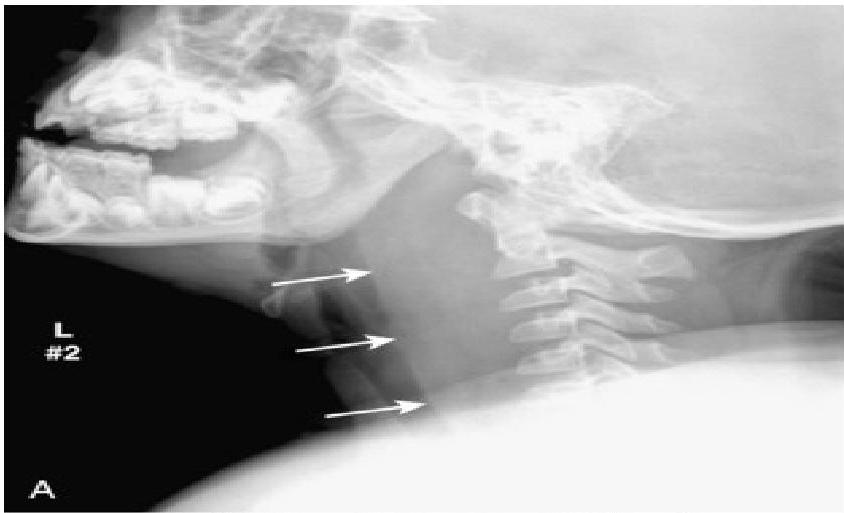
- Soft-tissue Lateral Neck Radiographs:
- Portable if possible.
- Positive in 80% of cases.
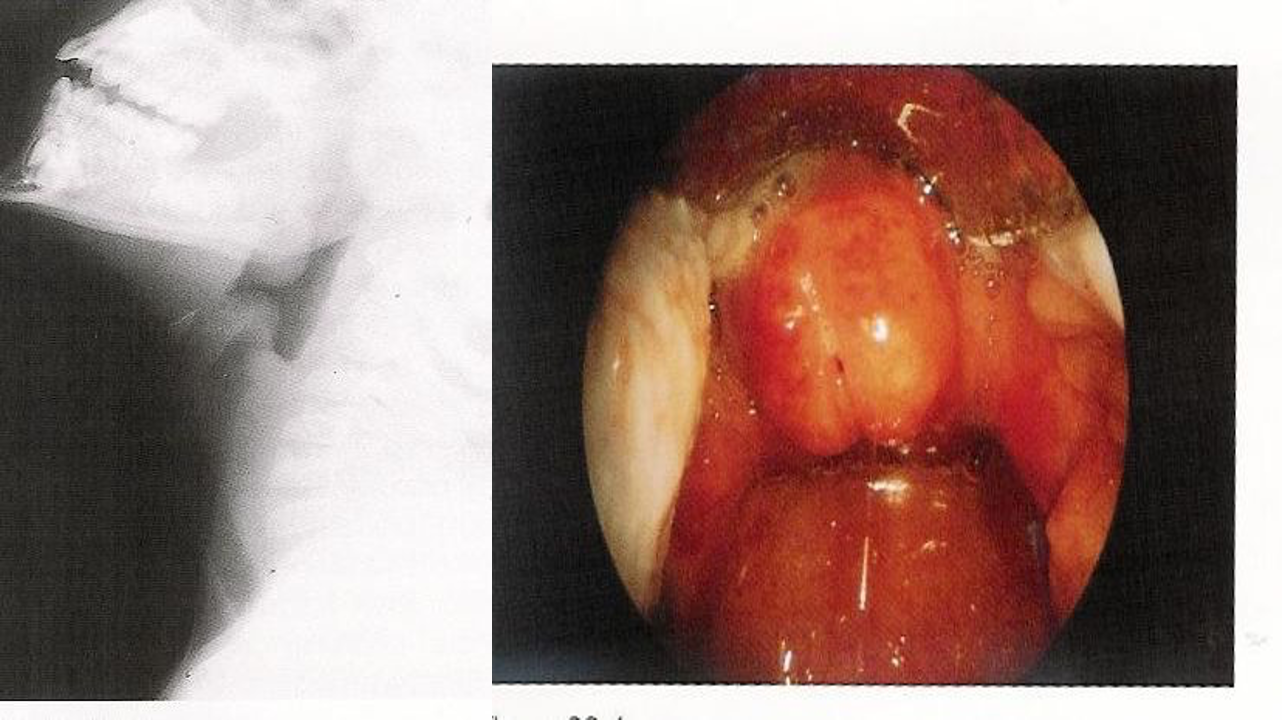
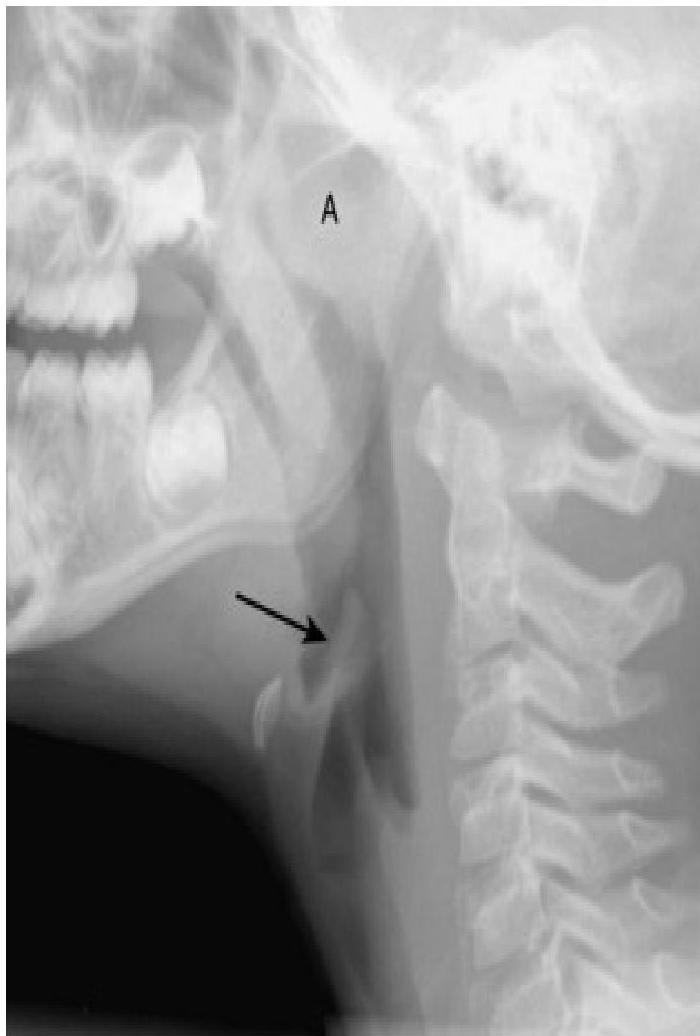
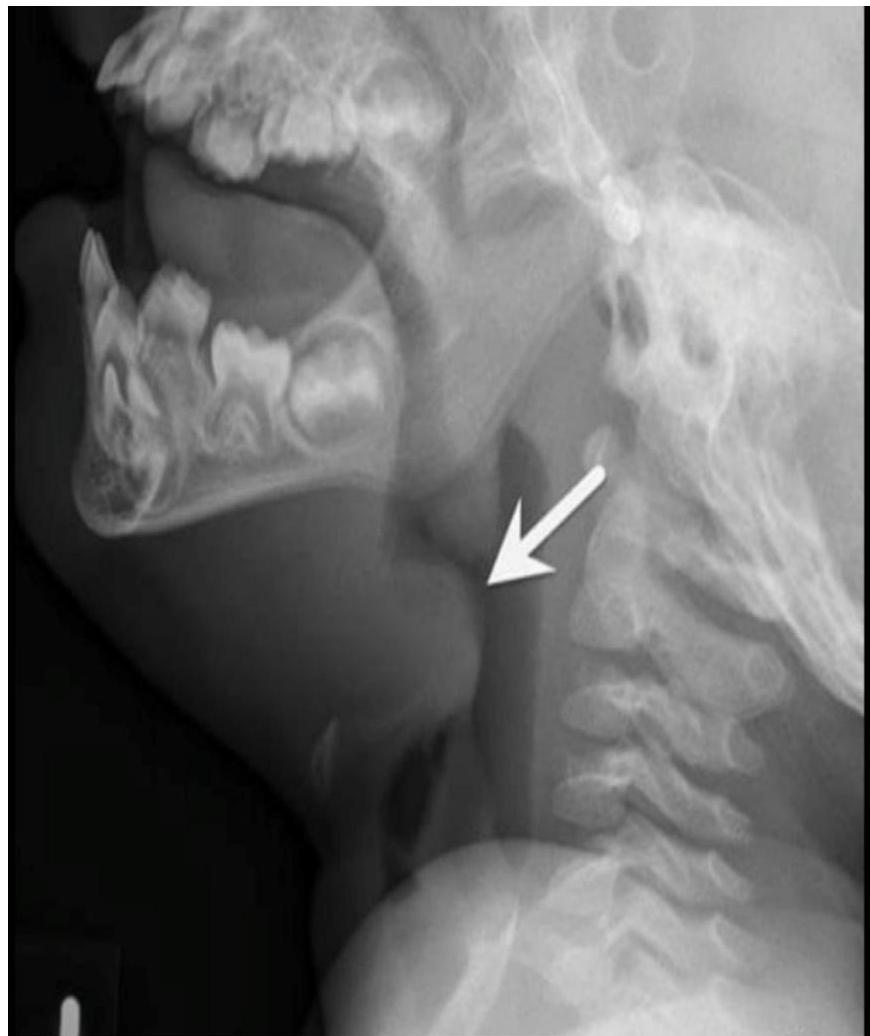
- Feature: An enlarged epiglottis protruding from the anterior wall of the hypopharynx (the “thumb sign”).
- Other findings: Thickened aryepiglottic folds, loss of vallecular air space, distended hypopharynx.
- Direct Visualization: Preferred if clinical suspicion is high. Performed during airway management in the operating suite. Shows a swollen, cherry-red epiglottis with an endotracheal tube passing posteriorly.
- Laboratory Studies (After airway is secured):
- Complete blood count (CBC) with differential.
- Blood culture.
- Epiglottal culture (in intubated patients).


 swollen cherry-red epiglottitis with an endotracheal tube passing posteriorly
swollen cherry-red epiglottitis with an endotracheal tube passing posteriorly
Management of Epiglottitis
Immediate Emergency Management
- Do NOT irritate the child: Keep them on the parent’s lap.
- AVOID: Sedation, inhalers, or nebulizers.
- Procedures to Avoid: Oropharyngeal examination with a tongue blade or other instruments (may provoke anxiety or crying with abrupt airway obstruction).
- Diagnostic Tests: Avoid IV access, phlebotomy, or cultures in young children (≤ 6 years) until the airway is secured.
- Airway Management: The most urgent priority.
- Assess level of distress before any other workup.
- Ensure ENT and Anesthesiology are available before tracheal intubation.
- Airway equipment including that for cricothyrotomy and tracheotomy must be ready.
- Supplemental, humidified O2 if possible (highest concentration that does not cause agitation).
Medical Management
- ICU Monitoring: All patients should be monitored in a pediatric intensive care unit.
- Antibiotics:
- Ceftriaxone or Cefotaxime
- PLUS Clindamycin or Vancomycin (for community or hospital S. aureus).
- Corticosteroids: May be added to minimize swelling of the epiglottis.
- Prophylaxis: Rifampin for close contacts.
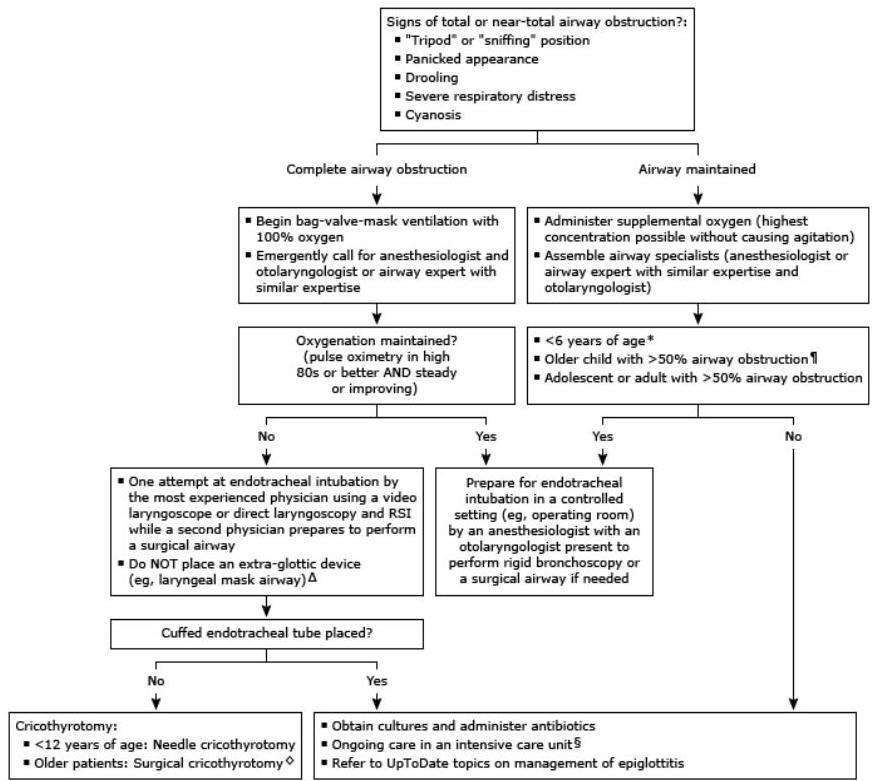
Rapid Overview of Emergency Management (Tables summary)
- Preparation: Get emergency assistance from airway specialists (anesthesiologist/critical care and otolaryngologist).
- Sudden Deterioration:
- Attempt bag-valve mask ventilation with 100% oxygen.
- Unable to oxygenate (pulse oximetry < high 80s or falling): Attempt endotracheal intubation by RSI with surgical/needle cricothyrotomy as backup.
- Able to oxygenate (pulse oximetry high 80s and steady/improving): Intubation by the most capable provider, preferably in the OR.
- Airway Maintained: Supplemental O2, upright position of comfort (child on caregiver’s lap), and constant monitoring. Do not image if it delays definitive management.
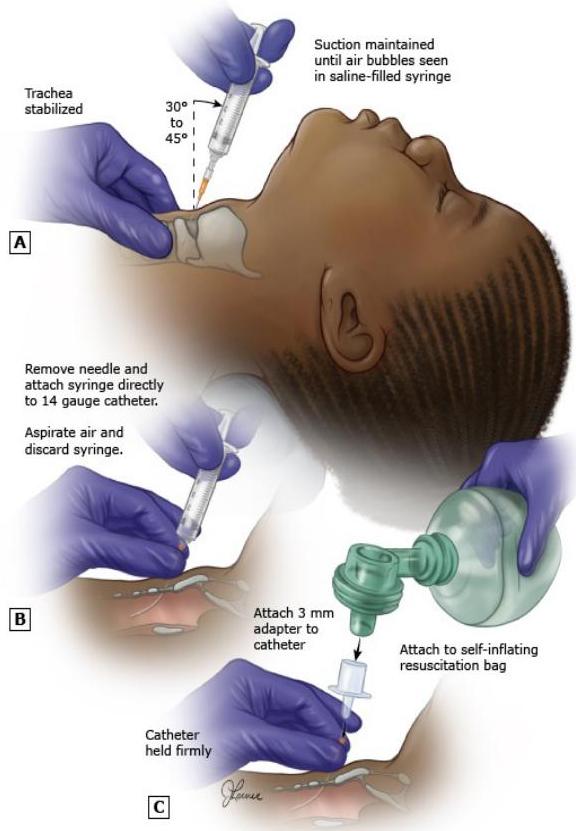
Needle Cricothyroidotomy
- Procedure: The needle (14 gauge) is angled caudally at 30 to 45 degrees and inserted through the cricothyroid membrane until bubbles are seen in a fluid-filled syringe.
- Advancement: The catheter is advanced as the needle is removed.
- Ventilation: Secure catheter and connect to a self-inflating ventilation bag (using a 3.0 or 7.0 ET tube adaptor).
- Note: Needle cricothyroidotomy can be performed on children of any age. Surgical cricothyrotomy age recommendations vary from 5 to 12 years.
ENT
Acute Epiglottitis
Overview
Acute Epiglottitis is a life-threatening, rapidly progressive condition primarily caused by Haemophilus influenzae type B. It typically affects children aged 2-7 years.
Symptoms
- High Fever
- Dysphagia
- Drooling
- Dyspnea
- Stridor
- Toxic-looking child (sitting upright with head extended)
- Sniffing position
- No cough
- Normal voice
Diagnosis
- X-ray: Look for the thumbprint sign.
Treatment
NO EXAMINATION SHOULD BE DONE IN ER !!!
- Intubation in the Operating Room (OR).
- Tracheostomy may be necessary.
- IV Antibiotics.
- Corticosteroids.