ABDOMINAL TRAUMA
Dr. Abdulaziz Alrabiah
Classification of Abdominal Trauma
- Blunt
- Penetrating
Blunt Abdominal Trauma
- Common mechanisms: Road traffic crashes, falls, sports injuries, and assaults.
- Organs most affected: Spleen > Liver > Small and large intestine.
- Management: Often managed conservatively, though interventional radiology and surgery are indicated for severe injuries.
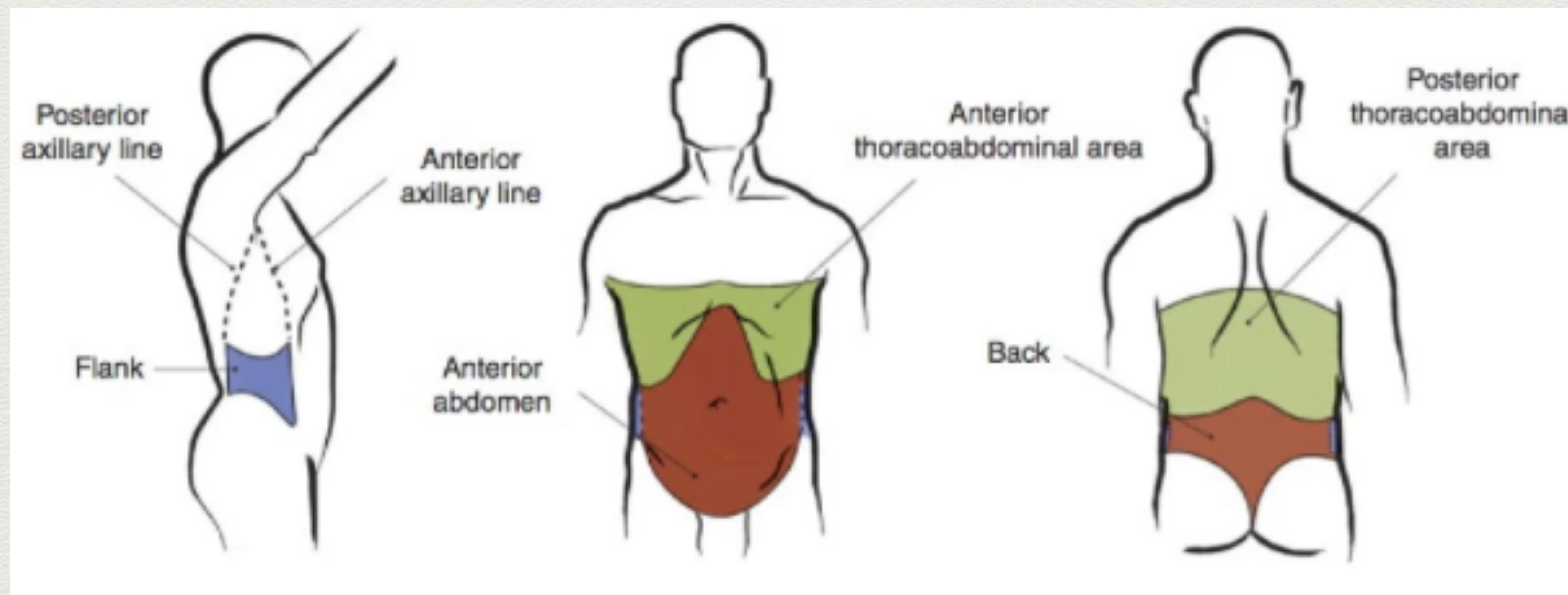
Penetrating Abdominal Injury
Liver
- Definition: Any wound between the nipple line (T4) and the groin creases anteriorly, and from T4 to the curves of the iliac crests posteriorly is potentially a penetrating abdominal injury.
Assessment of Abdominal Trauma
- Primary Survey: ABCDE
- Secondary Survey:
- Inspection:
- Abrasions, wounds.
- Bruising.
- Seat belt marks: Indicate bad sign.
- Lap belt: 30% chance of mesenteric or intestinal injury (not used anymore).
- Retroperitoneal haemorrhage: Ecchymosis of the periumbilical area (Cullen’s sign) and the flanks (Grey-Turner’s sign).
- Genital and perineum examination.
- Palpation:
- Fullness: Suggests haemorrhage.
- Crepitation of lower rib cage: Suggests hepatic or splenic injury.
- Peritonism: Ruptured viscus with leakage.
- Rectal or vaginal examination.
- Inspection:
Investigations
- Trauma Series: e.g., CXR, pelvis XR (
c-spine XR). - Trauma Blood Panel: e.g., FBC, UEC, LFTs, lipase, coags, group and hold, BHCG.
- Imaging: Bedside FAST scan, +/- CT abdomen if haemodynamically stable and imaging warranted.
FAST Scan (Focused Assessment with Sonography for Trauma)
Protocol:
- Positive (+) & Patient Stable → CT scan.
- Positive (+) & Patient Unstable → Operation.
Details:
- Sensitivity: 70-95%.
- 4 Regions Analyzed:
- Subxiphoid: Pericardial space + rough assessment of contractility and filling.
- RUQ (Right Upper Quadrant).
- Splenorenal Recess.
- Pelvis.
Pros:
- Quick to perform with immediate results.
- Repeatable.
- Patient doesn’t have to leave Emergency Department.
- Sensitivity approaching 96% in detecting >800mls blood.
Cons:
- Requires >250 mL free fluid to collect in Morison’s pouch for a positive result.
- Operator dependent.
- Doesn’t specify anatomical structures injured.
- Does not distinguish other causes of intraperitoneal fluid (e.g., ascites, residual fluid after DPL, bladder rupture).
- Shows only intraperitoneal bleed; does not show retroperitoneal bleed.
- Doesn’t look at solid organs, hollow viscera, or retroperitoneal structures.
- Can be technically difficult in obese patients, those with lots of bowel gas, or if subcutaneous emphysema is present.
Diagnostic Peritoneal Lavage (DPL) y
- Rarely performed; minor surgical procedure.
- Pros:
- Highly sensitive for intraperitoneal hemorrhage (>97%).
- Rapid.
- Performed at the bedside.
- Cons:
- Invasive.
- Doesn’t specify anatomical structures injured.
- False positives may result from trauma during the procedure (up to 25% negative laparotomy rate).
- Rarely performed, practitioners have become deskilled.
- Residual fluid following DPL makes subsequent FAST scans unreliable.
- Modified technique required if pregnant, pelvic fracture, or midline scarring.
CT Abdomen and Pelvis
- Prerequisite: Patient must be stable.
- Indications:
- Trauma patients with abdominal tenderness.
- Trauma patients with altered sensorium.
- Distracting injuries or injuries to adjacent structures.
- Pros:
- Identifies specific anatomical structures injured, allows grading of severity, and helps guide management.
- Concurrent imaging of other body compartments is frequently indicated.
- Images retroperitoneal structures.
- Provides imaging of the thoracolumbar vertebrae and other skeletal structures.
- Blush of IV contrast: Strong predictor of failure of non-interventional management.
- Cons:
- Patient usually has to leave the ED.
- Patient transfers are time-consuming.
- Requires IV contrast and risk of adverse reactions.
- Radiation exposure.
- Less sensitive with pancreatic, diaphragmatic, and hollow viscus injuries.
- Poor access to patient during the scan should they deteriorate.
- Requires additional skilled staff (CT radiographers and radiologists).
Management
- Address ABCDE.
- IV lines (i.e., 16G, 18G).
- Fluids, Bloods +/- Vasopressors.
Laparotomy
✓ Indications:
- Peritonism.
- Free air.
- Evisceration.
- Penetrating abdominal trauma + hypotension (unstable).
- Gunshot wound traversing peritoneum or retroperitoneum.
- GI bleeding following penetrating trauma.
- Penetrating object is still in situ (risk of precipitous haemorrhage on removal).
- Blunt abdominal trauma + hypotension with positive FAST scan, positive DPL, or peritonism.
(Note: Assess before laparotomy)
Interventional Radiology
- Main Role: Stop bleeding without the physiological stress of surgery.
- Sources of Bleeding: Typically spleen, liver, pelvis, retroperitoneal, or gastrointestinal haemorrhage.
- Techniques: Embolisation and balloon occlusion.
- May be performed in conjunction with operative intervention in some centres.
Damage Control Surgery
- Concept: Open the area, apply packing and gauze, then send to tertiary care or ICU.
- Integral to Damage Control Resuscitation (along with permissive hypotension and hemostatic resuscitation). is integral to the concept of damage control resuscitation
- Derived from military experience and increasingly adopted into civilian trauma management.
Pelvic Trauma
Classification: Open Book Fracture

Pelvic X-ray showing a large separation (diastasis) between the pubic bones, characteristic of an open book pelvic fracture (>3cm).
Treatment
- ✓ Pelvic Binder
- ✓ Blood Transfusion (Blindly/Empirically)
- ✓ Call for Interventional Radiology
 Medical brace/pelvic binder.
Medical brace/pelvic binder.
 Medical support belt.
Medical support belt.
 Patient with surgical drain and IV line.
Patient with surgical drain and IV line.
Thank You aalrabiah@ksu.edu.sa