Acute Abdomen
Hani Albrahim, MD
Which condition has the highest mortality rate?
- Ruptured AAA (Highest mortality, affects old age, causes major bleeding)
- Perforated peptic ulcer
- Mesenteric ischemia
- Bowel obstruction
”Pain out of proportion” is a characteristic feature of:
- Mesenteric ischemia
- Ruptured AAA
- Perforated peptic ulcer
- Intestinal obstruction
Best modality to diagnose acute cholecystitis is:
- CT Scan with contrast
- CT scan without contrast
- MRI
- Ultrasound (Shows gall stones, thickening of wall, fluid)
- Clinical

1. Introduction
“Acute Abdomen” encompasses a spectrum of surgical, medical, and gynecological conditions—ranging from trivial to life-threatening—that require hospital admission, investigation, and treatment.
Key Concepts
- Definition: An intra-abdominal process causing severe pain requiring admission, which has not been previously investigated or treated, and may need surgical intervention.
- Mortality: Varies with age, highest at extremes of age.
- Highest Mortality Conditions:
- Mesenteric ischemia
- Ruptured Abdominal Aortic Aneurysm (AAA)
- Perforated peptic ulcer
2. Etiology (Causes)
A. Gastrointestinal
| Organ | Conditions & Clinical Pearls |
|---|---|
| Gut | • Acute Appendicitis: RLQ pain, Rebound tenderness. • Intestinal Obstruction: Common in all ages (causes differ). • Perforated Peptic Ulcer: Risk in post-surgical or Hx of ulcer; presents sick/hypotensive. • Diverticulitis: Age >45-50, Left-sided pain. |
| Spleen | • Splenic Infarct: Sickle cell disease. • Rupture: Trauma, associated with left shoulder pain. |
| Liver / Biliary | • Cholecystitis: 100% clinical diagnosis, confirmed by LFT/US. • Cholangitis: Fever + Jaundice + Sick patient. • Hepatitis |
| Pancreas | • Acute Pancreatitis: Most common risk is gallstones, followed by alcohol and hyperlipidemia. |
B. Genitourinary
- Upper UTI: Acute pyelonephritis.
- Lower UTI: Cystitis.
- Ureteric Colic.
C. Vascular (Critical)
- Ruptured Aortic Aneurysm: Very high mortality.
- Mesenteric Embolus: Elderly patients presenting with pain out of proportion to exam.
- Mesenteric Venous Thrombosis: Associated with Atrial Fibrillation (AF) and ↑ Lactic acid.
- Ischemic Colitis.
D. Other Systems
- Abdominal Wall: Rectus sheath hematoma.
- Peritoneum: Primary or Secondary peritonitis.
- Retroperitoneal: Hemorrhage (e.g., anticoagulants).
- Gynecological: Torsion/Rupture of ovarian cyst, Fibroid degeneration, Ectopic pregnancy (RLQ pain, rebound). - ovarian infarction
E. Extra-Abdominal Mimics
- Respiratory: Lobar pneumonia.
- Cardiac: Myocardial Infarction (>40% presentation overlap).
- Hematologic/Metabolic: Sickle cell crisis, DKA (check urgency), Addison’s disease.
3. Clinical Diagnosis
History, physical examination, management
Regional Differential Diagnosis
| Region | Primary Differentials |
|---|---|
| Epigastric | Peptic ulcer disease, Cholecystitis, Pancreatitis, MI |
| Peri-umbilical | Small/Large bowel obstruction, Appendicitis, AAA |
| RUQ | Cholecystitis, Pyelonephritis, Ureteric colic, Hepatitis, Pneumonia |
| LUQ | Gastric Ulcer, Pyelonephritis, Ureteric colic, Pneumonia |
| RLQ | Appendicitis, Ureteric colic, Inguinal hernia, IBD, UTI, Gynae/Testicular torsion |
| LLQ | Diverticulitis, Ureteric colic, Inguinal hernia, IBD, UTI, Gynae/Testicular torsion |
Symptom Correlations
| Associated Symptom | Specific Signs | Likely Cause |
|---|---|---|
| Fever | Vomiting, Diarrhea, Sick contacts | Acute Gastroenteritis |
| Dysuria, Renal angle/suprapubic tenderness | Urinary Tract Infection | |
| Throat Pain, Pharyngeal Erythema | Streptococcal Pharyngitis | |
| Resp distress, Consolidation/effusion | Pneumonia | |
| Vomiting, RUQ pain | Acute Cholecystitis | |
| H/O Surgery, Ileus, Toxicity | Intraabdominal Abscess | |
| Vomiting | Normal abdominal examination | Mesenteric Lymphadenitis |
| Lower Abd Pain | Tenesmus, Blood in stool | Acute Colitis |
Characteristics of Pain
- Site: (See table above). Note: In situs inversus, signs are mirrored (e.g., Appendicitis in LLQ).
- Onset:
- Sudden: Perforation.
- Slow: Inflammation.
- Severity:
- Severe but not lethal: Kidney stone.
- Mild but lethal: Malignancy.
- Ureteric Colic: Rated 10/10 (“worst pain”).
- Pain rating: Patients are often asked to score pain 1‑10 to help differentiate severe colicky episodes from milder inflammatory pain.
- Character:
- Burning: Peptic ulcer.
- Stabbing: Ureteric colic.
- Gripping: Smooth muscle spasm (Obstruction).
- Aching-dull pain poorly localized
- Radiation:
- Back: Pancreatitis, AAA, Duodenal ulcer.
- Shoulder: Cholecystitis (Right), Spleen rupture (Left).
- Loin to Groin: Ureteric colic.
- Sacroiliac region: May indicate ovarian pathology.
- Groin: Can reflect testicular torsion.
- Cessation:
- Abrupt ending: Typical of colicky pains (e.g., ureteric colic).
- Gradual resolution: Seen with inflammatory or biliary pain.
- Progression:
- Constant: Often signifies perforated ulcer or ongoing peritonitis.
- Intermittent/colicky: Characteristic of bowel obstruction or ureteric colic.
- Exacerbating / Relieving Factors:
- Movement / Rest: Worsens spasm‑related pain (obstruction), may relieve colicky pain.
- Food intake: Aggravates peptic ulcer pain, may relieve gall‑bladder pain after meals.
- Positioning: Leaning forward can ease peritonitis; sitting up may worsen reflux‑related pain.
History
- Past Surgical: Adhesions? Previous “appendectomy” (stump appendicitis?).
- Drug Hx:
- Corticosteroids: Mask pain/inflammation.
- NSAIDs: Gastritis/Peptic ulcer.
- Anticoagulants: intra-muralHematoma risk.
- Family Hx
- Colon Cancer
- IBD
- Pain‑related History Checklist (for the present illness):
- Onset speed (sudden vs. gradual)
- Site and radiation
- Severity (patient pain score 1‑10)
- Character (burning, stabbing, gripping, etc.)
- Progression (constant vs. colicky)
- Cessation pattern (abrupt ending vs. gradual resolution)
- Exacerbating factors (movement, food, position)
- Relieving factors (rest, analgesia, posture)
- Associated symptoms (fever, vomiting, urinary changes, etc.)
4. Evaluation Strategy
Physical examination
A. General & vitals
- Position / behaviour
- Motionless — peritonitis / acute appendicitis
- Rolling in bed — ureteric or intestinal colic
- Bending forward — pancreatitis
- Temperature
- Low‑grade — appendicitis / acute cholecystitis
- High‑grade — abscess / pyelonephritis
- General appearance: conjunctival pallor, cyanosis, jaundice, signs of dehydration, lymphadenopathy
Cardio‑pulmonary
- Consider: myocardial infarction, basal pneumonia, pleural effusion
Abdominal examination
- Components: inspection, palpation, percussion, auscultation
- Inspection
- Observe movement with respiration, distension, visible peristalsis, masses, scars
- Check for cough impulse at hernial sites
- Palpation
- Superficial: tenderness, rebound tenderness, guarding, rigidity, palpable masses, hernial orifices
- Deep: organomegaly
- Percussion
- Tympanic note — intestinal obstruction
- Dullness over suprapubic area — acute urinary retention (bladder)
- Auscultation
- Silent abdomen — peritonitis
- Increased bowel sounds — intestinal obstruction
B. Inspection & Auscultation
- Cullen’s Sign: Periumbilical bruising (Pancreatitis/Bleeding).
- Grey Turner’s Sign: Flank bruising.
- Scars: Risk of adhesions.
- Bowel Sounds: Silent (Peritonitis) vs Increased/Tinkling (Obstruction).
Investigation
- Labs: CBC, U&E, LFT, Lipase (Specific for pancreatitis), Urinalysis, Pregnancy Test (Must for reproductive age).
- Imaging Selection:
- CXR: Free air under diaphragm (Standing).
- AXR: Air-fluid levels (Supine/Erect).
- CT with Contrast: Gold standard for general Acute Abdomen.
- CT Non-Contrast: Protocol for Renal Colic.
- Ultrasound: Biliary pathology, Gynaecological, Pediatric.
• CBC • Urea, electrolyte, creatinine, glucose • LFT • Lipase • Urinalysis • Pregnancy test • CXR • AXR • CT SCAN • U/S • Angiography
5. Clinical Cases
Case #1: Acute Appendicitis
Presentation: 24yo Male, 1 day RLQ pain radiating to groin. Vomiting. Exam: Tender RLQ, mild guarding.
- Classic Sequence: Periumbilical pain → Anorexia/Nausea → Localization to RLQ.
- Diagnosis: CT Scan with contrast in male or nonpreganant women (Gold Standard) showing dilated appendix (>6mm), fat stranding. - otherwise use ultrasound
- Treatment: NPO, IVF, Analgesia, Pre-op Antibiotics, Surgery.
Ultrasound showing tubular structure >6mm, non-compressible.

Axial CT scan showing dilated and thickened appendix.
Appendicitis
-
Classic presentation
- Periumbilical pain that often localizes to the right lower quadrant (RLQ)
- Anorexia, nausea, vomiting
- Note: pain localizing to the RLQ occurs in only about ½ to 2/3 of patients
-
Anatomic variations & atypical pain locations
- Retrocecal appendix (~26%): may produce flank pain
- Right upper quadrant (RUQ) location: ~4% of appendices
- Pelvic appendix: suprapubic pain, possible dysuria
- In males, pain can sometimes be referred to the testicles
-
Laboratory testing
- Urinalysis abnormal in ~19–40% of cases (can be misleading)
- CBC is neither sensitive nor specific
-
Imaging
- Ultrasound: useful, operator-dependent (consider in children & pregnancy)
- CT scan (gold standard) — typical findings:
- Pericecal inflammation
- Abscess or localized fluid collection
- Localized fat stranding
-
Clinical tip: combine history, exam, labs, and imaging — atypical presentations are common, so maintain a broad differential.
Treatment
- NPO
- IVFs
- Analgesia
- Preoperative antibiotics – decrease the incidence of postoperative wound infections
Case #2: Acute Pancreatitis
Presentation: 46yo Male, Alcohol abuse. 3 days severe epigastric pain radiating to back. Exam: Tender epigastrium, voluntary guarding.
- Diagnostic Criteria (2 of 3):
- Clinical pain (Epigastric → Back).
- Lipase > 3x normal.
- Imaging confirmation (CT/MRI).
- Signs: Cullen’s (Umbilicus), Grey Turner’s (Flank).
- Treatment: Supportive (Fluids, Pain control, NPO). Antibiotics only if severe/necrotizing.
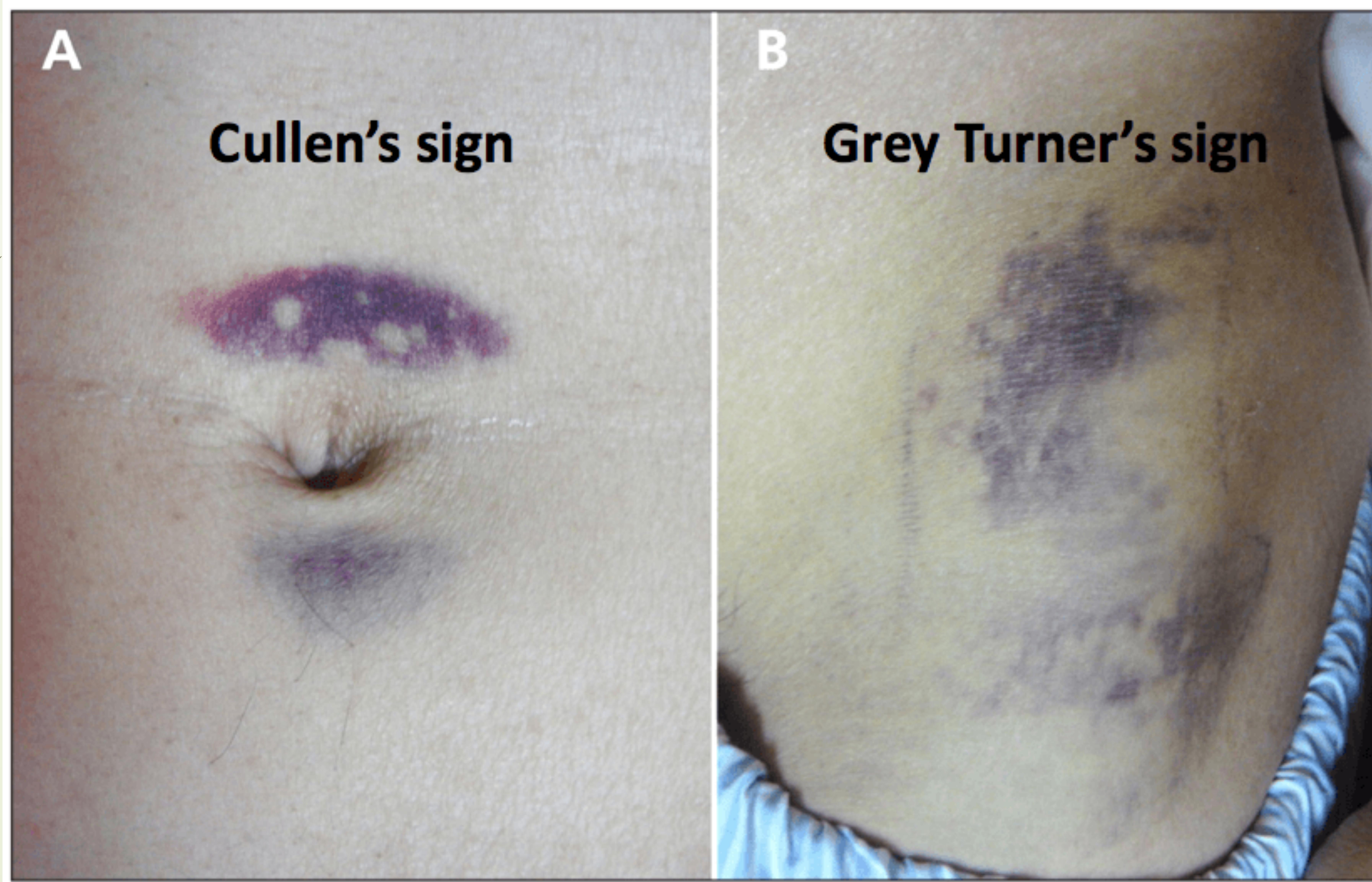
A: Cullen’s sign. B: Grey Turner’s sign.
Pancreatitis – Overview
-
Risk factors
- Alcohol
- Gallstones
- Drugs: amiodarone, antivirals, diuretics, NSAIDs
- Severe hyperlipidemia
- Idiopathic
-
Clinical picture
- Epigastric pain radiating to the back, often severe
- Nausea / vomiting
- Low‑grade fever, tachycardia, possible hypotension
- Late signs: peritonitis, ileus
- Skin signs (rare):
- Cullen sign – bluish discoloration around the umbilicus
- Grey‑Turner sign – bluish discoloration of the flanks
-
Diagnostic criteria (need 2 of 3)
- Typical clinical presentation
- Lipase > 2–3 × upper limit (sensitivity & specificity > 90 %)
- Imaging (CT or MRI) – may be normal early, but useful for complications
Notes
- Amylase is less specific and not required for diagnosis.
- CT is not necessary to confirm pancreatitis but helps assess severity or complications.
-
Management
- NPO (nothing by mouth)
- Aggressive IV fluid resuscitation
- NG tube if severe disease or persistent nausea/vomiting
- Antibiotics only for infected necrosis or severe infection
- Mild cases (tolerating oral fluids): discharge on a liquid diet with follow‑up in 24–48 h
- Other cases: admit for monitoring and supportive care
Case #3: Perforated Peptic Ulcer
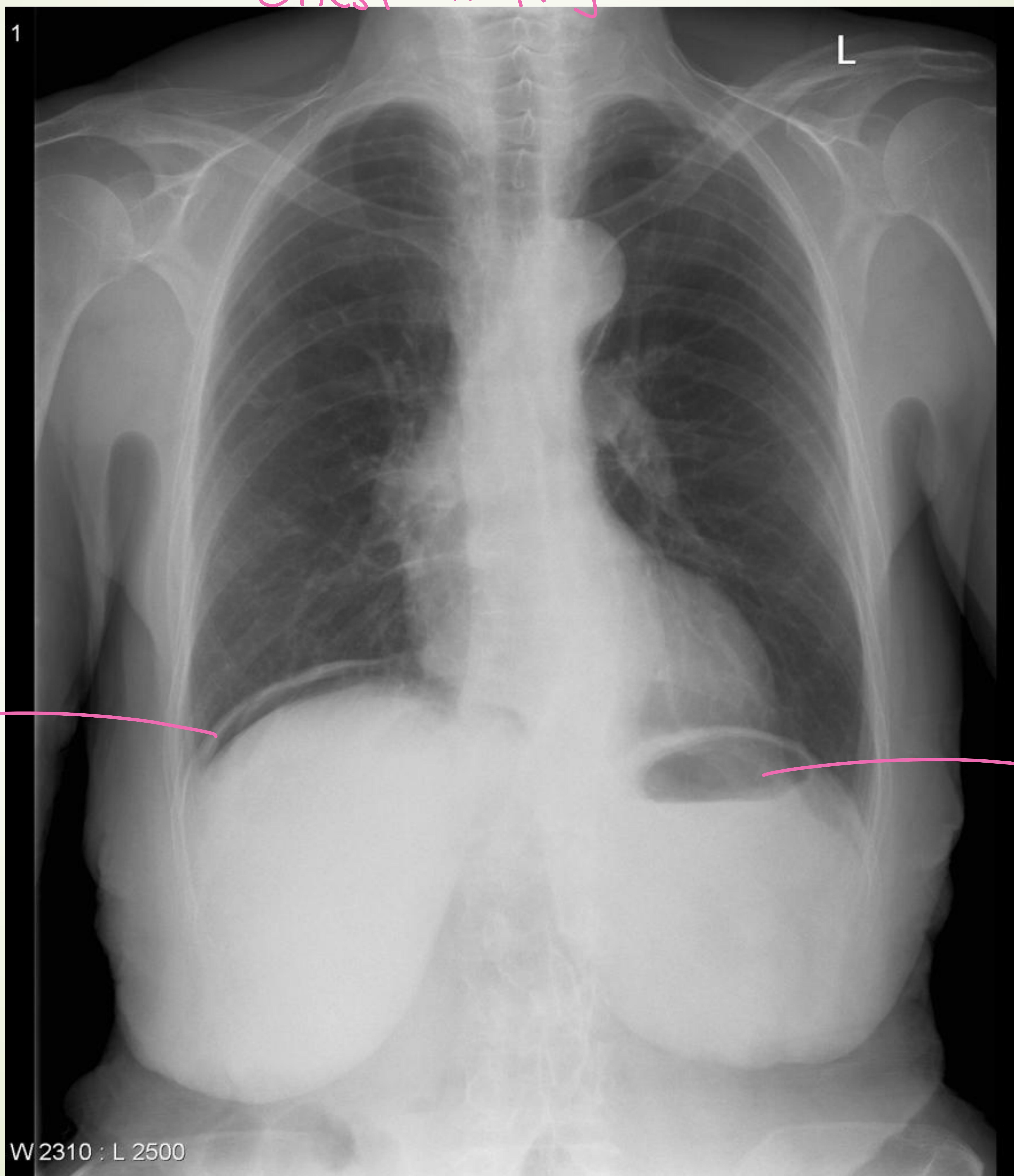
Chest X-Ray showing air under the diaphragm.
Case Summary
72‑year‑old male with CAD on aspirin + Plavix presents after several days of dull upper‑abdominal pain that has become widespread and worsening after lunch. He had mild relief with food until today.
Relevant History
- Medical: CAD, HTN, CHF
- Surgical: Appendectomy
- Medications: Aspirin, Plavix
Physical Exam
- Vitals: T 37.1 °C, HR 70 bpm, BP 90/45 mm Hg, RR 22 /min
- General: thin, ill‑appearing elderly male
- Abdomen: mildly distended, diffusely tender, +rebound & guarding
- Rectal: blood‑streaked stool (+ occult blood)
Differential Diagnosis
- Peptic ulcer disease (possible perforation)
- Acute mesenteric ischemia
- Acute pancreatitis
- Ischemic colitis / colonic perforation
- Small‑bowel obstruction
Immediate Work‑up (Next Steps)
- Labs: CBC, CMP (including LFTs), serum lipase/amylase, coagulation profile, type & crossmatch
- Stool/Rectal: occult blood (already positive)
- Imaging: upright abdominal + chest X‑ray (look for free air, though its absence does not exclude perforation); consider CT abdomen/pelvis with contrast if stable
- Early GI consult: for possible EGD (definitive diagnosis) or therapeutic intervention
- Supportive care: IV fluids, oxygen, cardiac monitoring, analgesia as needed
Key Points on Peptic Ulcer Disease
Clinical Features
- Burning or “hungry” epigastric pain, often relieved by food, milk, or antacids
- May awaken the patient at night
- Can progress to sharp, dull, achy pain or generalized peritonitis if perforated
Risk Factors
- H. pylori infection
- NSAIDs, aspirin, antiplatelet agents (e.g., Plavix)
- Smoking, family history
Physical Findings
- Epigastric tenderness; rebound and guarding suggest perforation
Diagnostic Approach
- Rectal occult blood test (positive in this case)
- CBC, LFTs, lipase (to rule out pancreatitis)
- Definitive: EGD or upper‑GI barium study
Treatment Overview
- Lifestyle: stop smoking, avoid NSAIDs/aspirin when possible
- Medication: PPI or H₂‑blocker; H. pylori eradication regimen if indicated
- When to refer urgently to GI: age > 45 y, weight loss, prolonged symptoms, anemia, persistent vomiting, overt GI bleed
Management of a Perforated Peptic Ulcer
- Recognition: abrupt severe epigastric pain followed by signs of peritonitis
- Resuscitation: IV fluids, oxygen, continuous monitoring
- Investigations: CBC, LFTs, lipase, emergent abdominal X‑ray series (free air may be absent)
- Therapy: broad‑spectrum antibiotics, NPO, surgical consult for possible emergent repair
In this patient, the combination of NSAID/antiplatelet use, acute diffuse peritonitis, and positive occult blood makes a perforated peptic ulcer a leading concern—prompt imaging, aggressive supportive care, and urgent surgical/GI evaluation are warranted.
Case #4: Small Bowel Obstruction (SBO)
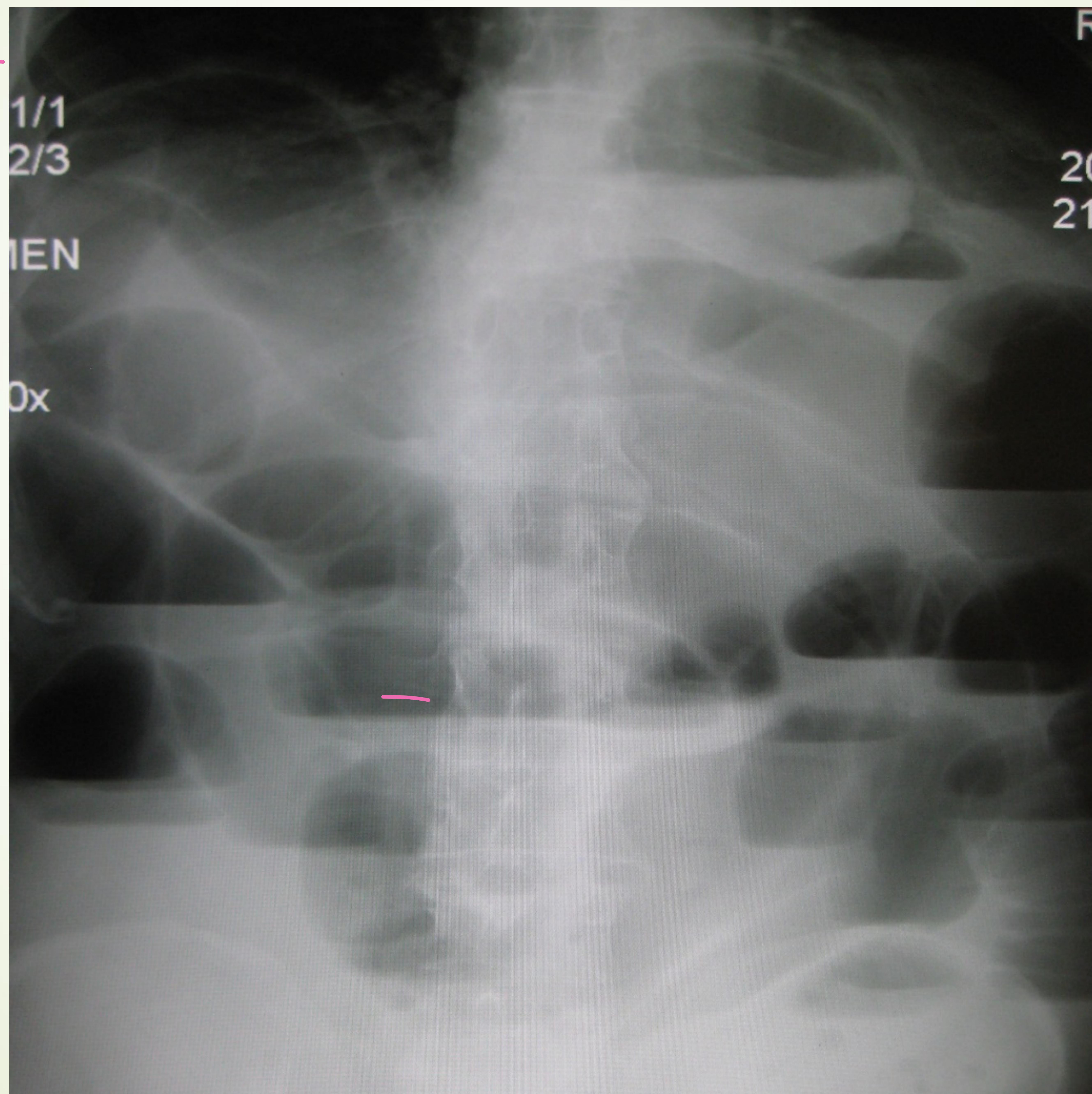
Upright abdominal X-ray showing multiple air-fluid levels.

POCUS: Dilated bowel > 2.5cm with to-and-fro peristalsis.
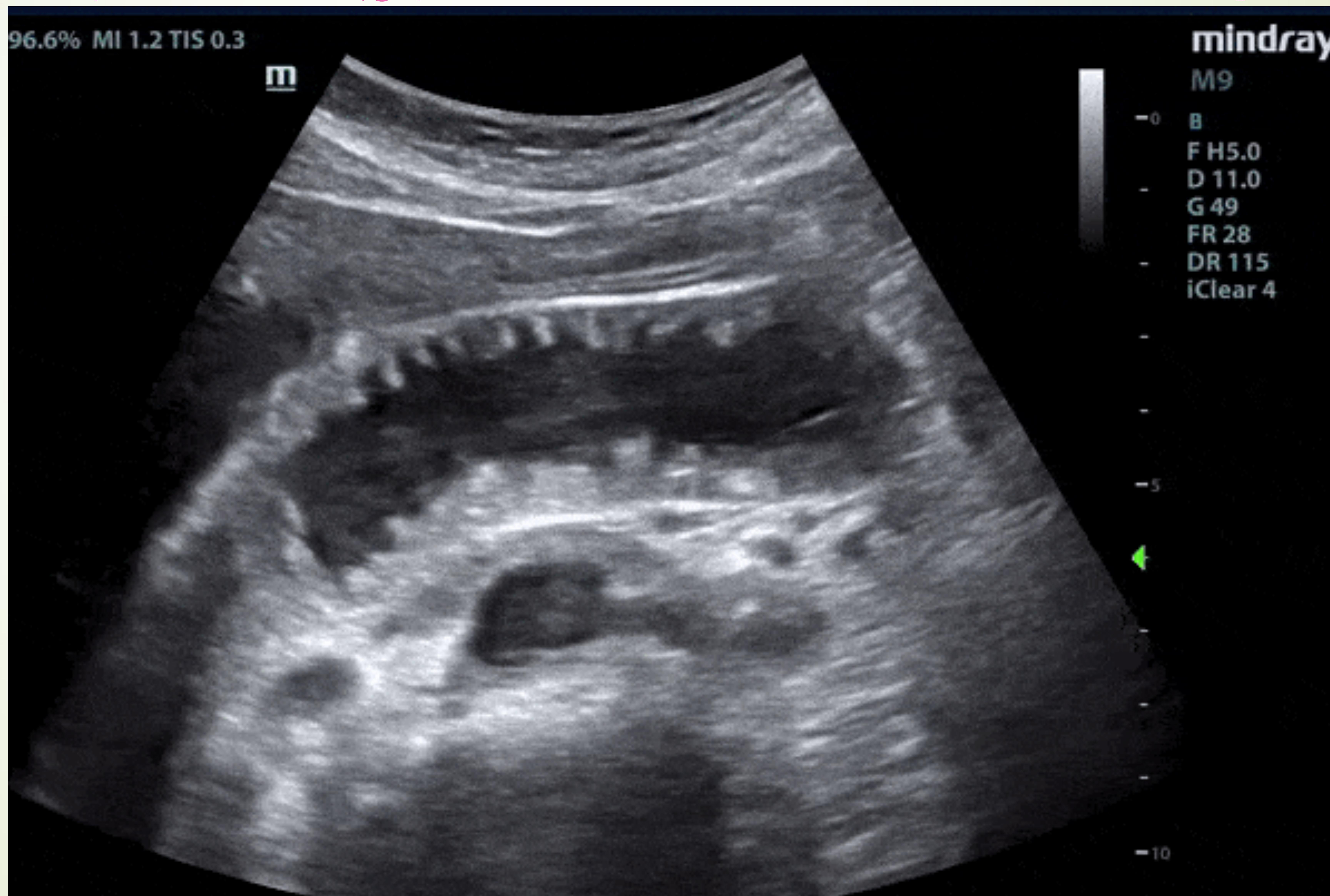
Ultrasound B-mode scan. Case #4
- 35‑year‑old healthy female presents to the ED with nausea, vomiting (since yesterday) and generalized abdominal pain. No fever or chills; anorexia present. Last bowel movement ≈ 2 days ago.
- Medical history: none.
- Surgical history: status post hysterectomy for fibroids (adhesive risk).
Exam
- Vitals: T 36.9 °C, HR 100 bpm, BP 130/85 mmHg, RR 22 /min.
- General: mildly obese, actively vomiting.
- Abdomen: moderately distended, diffusely tender, hypoactive bowel sounds; no rebound or guarding.
Differential & Next Step
- Primary consideration: Small‑bowel obstruction (SBO).
- Mechanical (e.g., adhesions from prior surgery, incarcerated groin hernia)
- Non‑mechanical (functional ileus)
Key Clinical Features of SBO
- Crampy, intermittent pain (periumbilical or diffuse)
- Inability to pass stool or flatus, nausea/vomiting, abdominal bloating, early satiety, anorexia
- Physical signs: distention, high‑pitched or tinkling bowel sounds, varying degrees of tenderness
Diagnostic Work‑up
- Labs: CBC, electrolytes (assess dehydration & infection)
- Imaging:
- Upright/flat abdominal X‑ray + chest X‑ray → look for air‑fluid levels, dilated loops, paucity of gas distal to obstruction.
- CT scan (gold‑standard): confirms obstruction, identifies cause, distinguishes partial vs. complete.
- Point‑of‑care ultrasound (POCUS) can aid early detection:
- Dilated loops > 2.5 cm
- “Tanga” sign (hyperactive to‑fro peristalsis)
- Wall thickening, reduced peristalsis
Management
- Initial resuscitation: generous IV fluids, correct electrolytes.
- Nasogastric tube for gastric decompression.
- Analgesia (avoid masking peritonitis).
- Surgical consult promptly; operative intervention indicated for complete obstruction or clinical deterioration.
- Peri‑operative antibiotics as indicated.
Case #5: Acute Cholecystitis
Presentation: 48yo Obese Female. RUQ pain after eating. Exam: +Murphy’s Sign.
- Gold Standard Image: RUQ Ultrasound (Thickened wall, fluid, stones, sonographic Murphy’s).
- Management: Antibiotics, Cholecystectomy.
• Clinical Features • RUQ or epigastric pain • Radiation to the back or shoulders • Dull and achy → sharp and localized • N/V/anorexia • Fever, chills
Physical findings • Epigastric or RUQ pain • Murphy’s sign • Patient appears ill • Peritoneal signs suggest perforation

Ultrasound showing gallbladder wall thickening and fluid.
Detailed US findings: Wall thickening, Pericholecystic fluid, Gallstones.
Case #6 – Renal Colic
Patient: 34‑year‑old healthy male
Presenting complaint
- Sudden onset (≈4 h) of left flank pain, severe, dull/achy, radiating toward the abdomen/groin (including testicles)
- Nausea & vomiting, diaphoresis; no fever or chills
- Difficulty urinating, feeling the urge but unable to void; no hematuria
Past history
- Medical & surgical: none
- Medications: none; Allergies: NKDA
Vital signs & exam
- T 36.9 °C, HR 110 bpm, BP 150/90 mm Hg, RR 20 /min
- General: appears in severe pain, diaphoretic, unable to sit still
- Abdomen: soft, non‑tender
- Back: mild left‑side tenderness
Differential & Work‑up (Focused on renal colic)
Typical clinical picture – abrupt, severe flank pain with possible radiation to the groin, nausea/vomiting, and diaphoresis; fever is unusual. Physical exam often shows little or only mild tenderness.
Key investigations
- Urinalysis – look for RBCs (stone) and WBCs (possible infection)
- CBC – if infection is suspected
- BUN/Creatinine – especially in older patients, those with a solitary kidney, or suspected severe obstruction
- Imaging –
- Ultrasound for hydronephrosis (quick bedside tool)
- CT scan – gold‑standard for detecting ureteral/kidney stones and assessing size/location
Management Overview
- IV fluid bolus → rehydrate & aid stone passage
- Analgesia
- Narcotics for severe pain
- NSAIDs (first‑line when not contraindicated)
- Urology follow‑up within 1‑2 weeks
- Admission & urology consult if stone > 5 mm, patient appears toxic, or infection is confirmed
- IV antibiotics for confirmed infection
Key points to remember: renal colic presents with acute, severe flank pain and may be mildly tender on exam; CT is the definitive diagnostic tool, and prompt pain control plus hydration are the cornerstones of initial treatment.
Locations of stones: Kidney, Ureter, Bladder.