Approach to Acute Poisoning
By Fahad Abuguyan
Clinical Scenarios
Case 1: Paracetamol Overdose
25 year-old male presents after ingestion of 20 tablets of paracetamol one hour ago. He is fully conscious, alert and vital signs are stable.
Next step?
- Induce vomiting
- Gastric lavage
- Activated charcoal
➤ Extract blood for investigation and send for level at 4 hours
Case 2: Antiepileptic Medication Overdose
16 year-old female presents with a significant decrease in level of consciousness after ingestion of a large amount of an epilepsy medication. She is unconscious, her BP and HR are normal.
Next step?
- NGT and gastric lavage
- Intubate
- CT brain
- IV fluids
Case 3: Seizure with Depression History
30 year-old with a history of depression, brought in for tonic-clonic seizures. Seizure was aborted with benzodiazepines, the patient was intubated for airway protection due to significantly depressed level of consciousness, BP 100/60, HR 160.
Next step?
- CT brain
- EEG
- ECG
- TOX screen
Overview
Acute poisoning is a dynamic medical illness usually representing an acute and potentially life-threatening exacerbation of a chronic underlying psychosocial disorder.
These patients form a heterogeneous group that requires a systematic approach based on:
- Early resuscitation where needed
- Risk assessment to guide further management
- Early consideration of the underlying psychosocial issues
Epidemiology
- Accounts for 5-10% of all emergency department visits
- 5% of all ICU admissions
- The most commonly implicated poisoning exposures are due to analgesics
- Overall mortality rate from drug overdose and poison exposure: 0.05%
- Mortality rate for hospitalized patients: 1-2%
Pathophysiologic Toxic Mechanisms
Primary Mechanisms:
- Local tissue damage from corrosive substances
- Pulmonary damage through aspiration of toxins
- Central nervous system effects - stimulation or depression leading to coma
- Autonomic nervous system modulation - cholinergic effects
- Cardiovascular effects - myocardial dysfunction, dysrhythmias, blood pressure changes
- Organ toxicity - liver or kidney damage
- Oxygen transport/utilization interference
- Acid-base balance disturbances
- Hematologic toxicity
General Approach
The systematic approach includes:
- Resuscitation
- Examination
- Risk assessment
- Investigation
- Decontamination
- Antidotes
- Supportive Therapy
- Disposition
Toxidromes
Physical findings attributed to a specific class of toxins that can provide important clues to narrow the differential diagnosis.
Sympathomimetic Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| Hyperalert, agitation, hallucinations, paranoia | Mydriasis | Hyperthermia, tachycardia, hypertension, wide pulse pressure, tachypnea, hyperpnea | Diaphoresis, tremors, hyper-reflexia, seizures | Cocaine, amphetamines, cathinones, ephedrine, pseudoephedrine, caffeine, phenylpropanolamine, theophylline |
Key Features: MATHS Mnemonic
- M : Mydriasis
- A : Agitation, arrhythmia, angina
- T : Tachycardia
- H : Hypertension, hyperthermia
- S : Seizure, sweating

Anticholinergic Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| Hypervigilance, agitation, hallucinations, delirium with mumbling speech, coma | Mydriasis | Hyperthermia, tachycardia, hypertension, tachypnea | Dry flushed skin, dry mucous membranes, decreased bowel sounds, urine retention, myoclonus, choreoathetosis, picking behavior, seizures (rare) | Antihistamines, tricyclic antidepressants, cyclobenzaprine, orphenadrine, antiparkinson agents, antispasmodics, phenothiazines, atropine, scopolamine, belladonna alkaloids |
Cholinergic Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| Confusion, coma | Miosis | Bradycardia, hypertension or hypotension, tachypnea or bradypnea | Salivation, urinary and fecal incontinence, diarrhea, emesis, diaphoresis, lacrimation, GI cramps, bronchoconstriction, muscle fasciculations, seizures, weakness | Organophosphate and carbamate insecticides, nerve agents, nicotine, pilocarpine, physostigmine, edrophonium, bethanechol, urecholine |
Opioid Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| CNS depression, coma | Miosis | Hypothermia, bradycardia, hypotension, apnea & bradypnea | Hyporeflexia, pulmonary edema, needle marks | Opioids (heroin, morphine, methadone, oxycodone, hydromorphone, diphenoxylate) |
Key Features: CPR-3H Mnemonic
- C : Coma
- P : Pinpoint pupils
- R : Respiratory depression
- H : Hypotension
- H : Hypothermia
- H : Hyporeflexia
Note: Meperidine (Demerol) will not cause miosis
start with 0.04 mg nalaxone antidote, titrate up q 2-3 mins as need for ventillation to 0.5 mg 2 mg 5 mg up to max 10-15 mg
Sedative-Hypnotic Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| CNS depression, confusion, stupor, coma | Miosis (usually) | Hypothermia, bradycardia, hypotension, apnea & bradypnea | Hyporeflexia | Benzodiazepines, barbiturates, carisoprodol, meprobamate, glutethimide, alcohols, zolpidem |
Withdrawal Toxidrome
| Mental Status | Pupils | Vital Signs | Other Manifestations | Toxic Agents |
|---|---|---|---|---|
| Altered mental status | Mydriasis | Hyperthermia, tachycardia, hypertension & hyperventilation | Tremors, hyperreflexia, seizures, nausea, vomiting | Withdrawal (EtOH, BDZ, opiates) |
Comparison: Anticholinergic vs Sympathomimetic Toxidromes
| Feature | Anticholinergic | Sympathomimetic |
|---|---|---|
| Skin | Dry | Diaphoresis |
| Bowel sound | Inhibited | Hyperactive |
| Urine retention | Present | Absent |
| Pupil | Dilated fixed | Dilated reactive |
Resuscitation
Initial Approach
- Target potential life threats in appropriately staffed and equipped resuscitation area
- Extended ABC approach (low threshold for intubation)
- VITAL SIGNS! are crucial
Consider Intubation In:
- Depressed level of consciousness
- Severe acidosis
- Respiratory failure
- Risk of aspiration (gastric lavage)
Early Detection of:
- Seizure (benzodiazepine)
- Hypoglycemia
- Hypothermia
- Hypotension
- Arrhythmia
In cardiac arrest from toxicological causes, resuscitation should be prolonged.
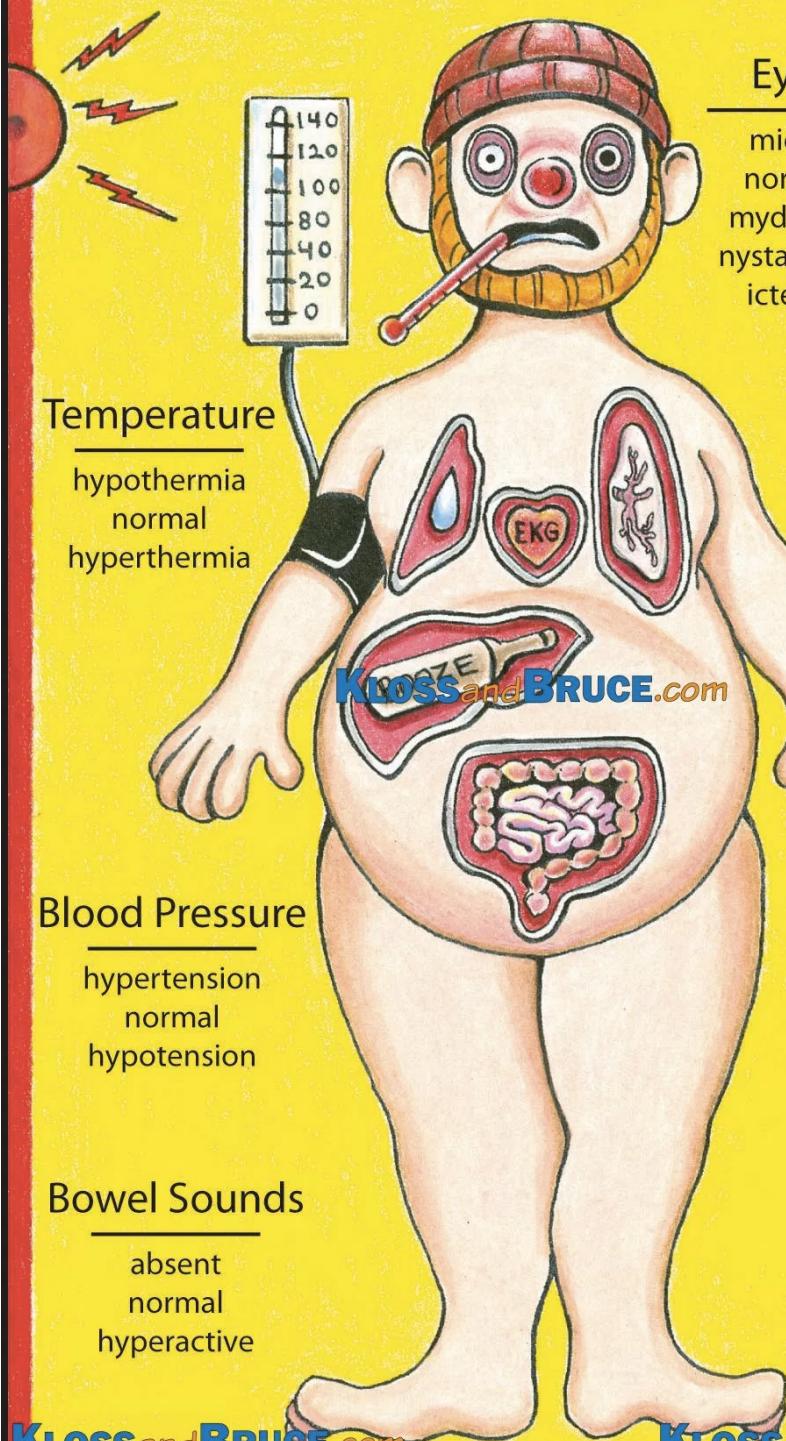
Clinical Examination
Detailed Examination Components:
- Vital signs
- Eyes - pupil size, reactivity, nystagmus, icterus
- Mucous membranes - moisture, color
- Breath and bowel sounds - rate, character
- Skin assessment - temperature, color, moisture
- Reflexes - deep tendon, pathological
Pupil Size Assessment
Miosis (COPS)
- Cholinergics, clonidine, carbamates
- Opioids, organophosphates
- Phenothiazines, pilocarpine, pontine hemorrhage
- Sedative-hypnotics
Mydriasis (SAW)
- Sympathomimetics
- Anticholinergics
- Withdrawal syndromes
Risk Assessment
Key Assessment Components:
- Agent(s) involved
- Dose(s) ingested
- Time since ingestion
- Current clinical status
- Patient factors (age, comorbidities, medications)
Investigations
Routine Laboratory Studies:
- Random blood glucose, electrolytes, renal function tests, liver function tests, CBC
- More useful than toxicology screens for acute management
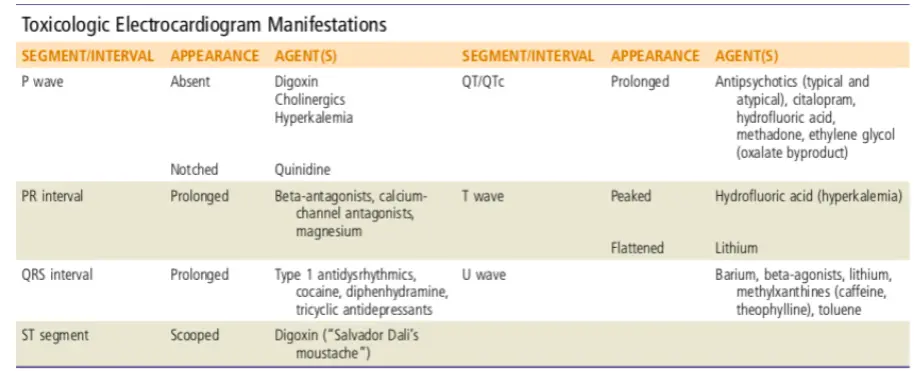
- ECG is mandatory - provides diagnostic and prognostic information
- Paracetamol level should be part of routine testing
Specific Drug Levels (when clinically significant):
- Measure levels for toxins with known therapeutic/toxic thresholds
- Timing is crucial (e.g., 4-hour paracetamol level)
Toxicology Screens:
- Used for confirmatory purposes only
- Does not typically modify acute management
- Most helpful for forensic or psychiatric follow-up
Radiological Studies:
- Chest X-ray - aspiration pneumonia, non-cardiogenic pulmonary edema
- Abdominal X-ray - useful for radio-opaque materials (iron, heavy metals)
Advanced Diagnostics:
- Anion gap calculation: Na⁺ - (Cl⁻ + HCO₃⁻)
- Normal: 4-12 mmol/L - An elevated anion gap strongly suggests the presence of a metabolic acidosis.The normal anion gap varies with different assays, but is typically 4 to 12 mmol/L
- Elevated gap suggests metabolic acidosis
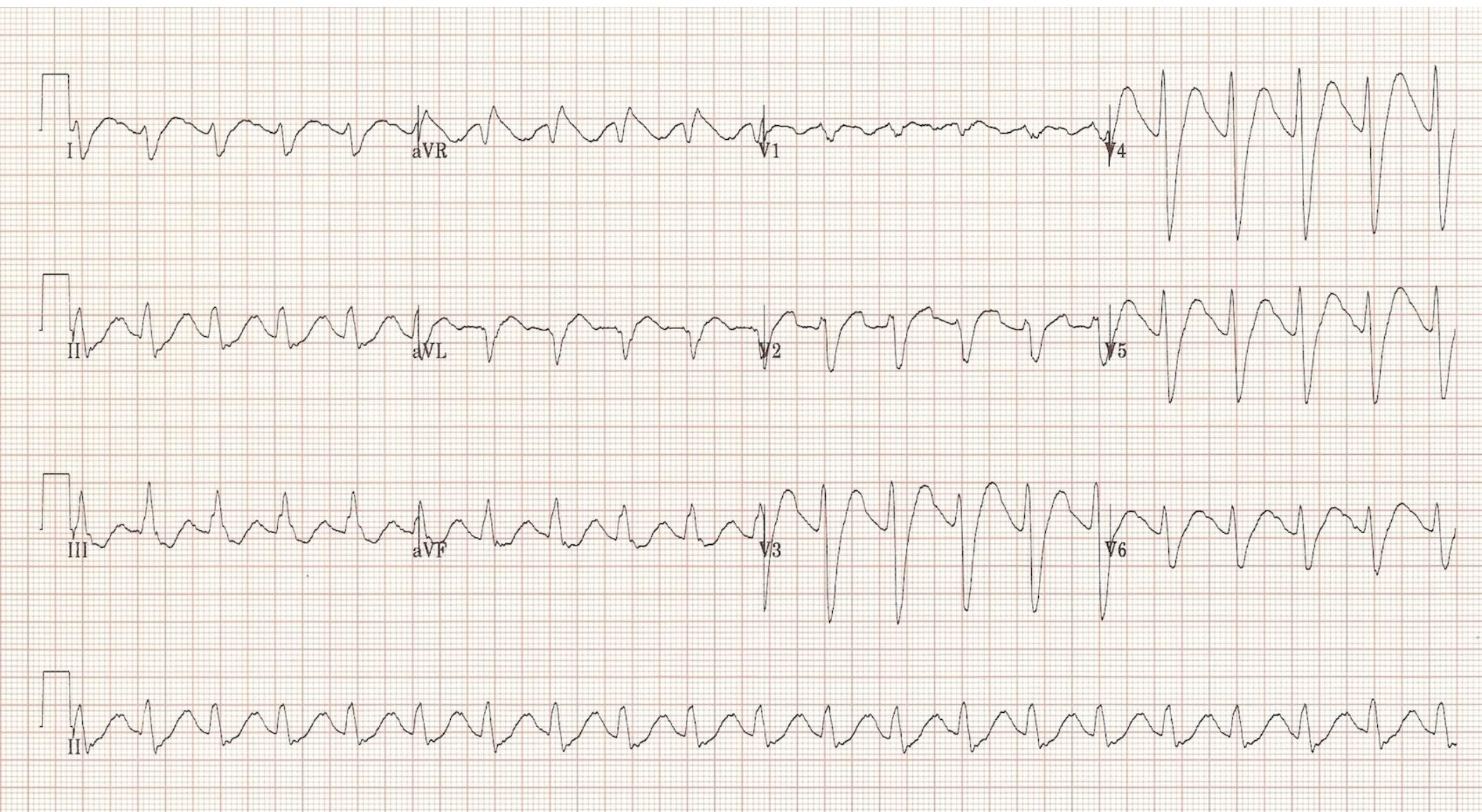
Toxicologic ECG Manifestations
High Anion Gap Metabolic Acidosis
Mnemonic: A CAT PILES MUD
- A - Alcoholic ketoacidosis
- C - Cyanide, Carbon monoxide, Colchicine
- T - Toluene
- P - Paraldehyde, Phenformin
- I - Isoniazid, Iron, Ibuprofen (large ingestions)
- L - Lactic acidosis
- E - Ethylene glycol
- S - Salicylates
- M - Methanol, Metformin, Massive ingestions
- U - Uremia
- D - Diabetic ketoacidosis
Decontamination
The sooner decontamination is performed, the more effective it is at preventing continued poison absorption.
Key Considerations:
- Severity of poisoning
- Time from ingestion
- Risk of intervention
Surface Decontamination
Skin Decontamination:
- Indicated for corrosives, hydrocarbons, and rapidly absorbed toxins (e.g., organophosphates)
- Remove contaminated clothing
- Irrigate with copious water
Eye Decontamination:
- Copious irrigation with water or saline
- Immediate intervention for caustic chemicals and irritants
- Continue until pH normalizes (typically 15-30 minutes)
Gastrointestinal Decontamination
Activated Charcoal:
- Dose: 1 g/kg (typically 50-100g)
- Timing: Most effective within 1 hour of ingestion
- Contraindications:
- Depressed consciousness without protected airway
- Corrosive ingestion
- Intestinal obstruction
- Substances that don’t bind to charcoal
• The patient should be alert, able, and willing to cooperate with administration, and anticipated to remain alert and protective of airway reflexes. • Best indicated in patients with ingestion of high toxic substance eg. Verapamil and Colchicine .
Substances That Do Not Bind to Activated Charcoal
PHAILS Mnemonic:
- P - Pesticides
- H - Heavy metals
- A - Acids/alkalis
- I - Iron
- L - Lithium
- S - Solvents
Gastric Lavage:
- Indication: Life-threatening poison ingestion within 1 hour
- Requirements: Protected airway, toxic lethal dose
- Contraindications: Corrosives, caustics, acids, petroleum products
- Complications: Visceral damage, aspiration
American Association of Poison Centers: “Within an hour of ingestion of a potentially life-threatening poison which does not adsorb to activated charcoal or for which no antidote exists” and, even then, in a center with “sufficient expertise” to perform the procedure safely.
Whole-Bowel Irrigation:
- Agent: Polyethylene glycol solution
- Rate: 1-2 L/hr (adults) until clear rectal effluent
- Indications:
- Ingestions of substances not bound by charcoal
- Sustained-release formulations
- Body packers/stuffers
- Foreign bodies
- Contraindications: Bowel obstruction, perforation, hemodynamic instability
Enhanced Elimination Techniques
Indications:
- Life-threatening toxicity
- Failure to respond to supportive care
- Toxins amenable to removal
Methods:
- Forced diuresis - limited utility
- Hemodialysis - most effective for small, water-soluble compounds
- Hemoperfusion - effective for protein-bound substances
- Hemofiltration - continuous removal
- Exchange transfusion - rare, specific indications
Characteristics of Dialyzable Toxins:
- Low molecular weight
- Low protein binding
- High water solubility
Dialyzable Toxins - STUMBLED Mnemonic:
- S - Salicylates
- T - Theophylline
- U - Uremia (as an indication)
- M - Metformin/methanol
- B - Barbiturates
- L - Lithium
- E - Ethylene glycol
- D - Depakote (valproic acid - in massive overdose)
Antidotes
Key Principles:
- Antidotes dramatically reduce morbidity and mortality in specific intoxications
- Used in only about 1% of cases
- Mechanisms:
- Prevent absorption
- Bind and neutralize poisons directly
- Antagonize organ effects
- Inhibit conversion to more toxic metabolites
Selected Antidotes and Indications
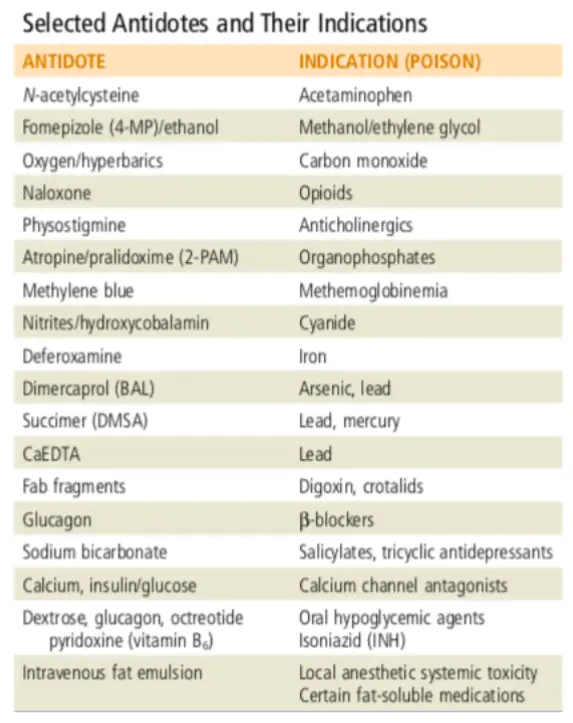
Important Antidotes Details:
Naloxone (for Opioid Overdose):
- Starting dose: 0.04 mg
- Titration: Increase q 2-3 min as needed for ventilation (0.04 → 0.5 → 2 → 5 → 10-15 mg max)
- Goal: Restore adequate ventilation, not complete consciousness
Intravenous Fat Emulsion (IFE) (Intralipid):
- Indication: Poison-induced cardiogenic shock
- Mechanism: Lipid sink theory
- First described: Local anesthetic toxicity (bupivacaine)
- Uses: Anesthetic agents, β-blockers, calcium channel blockers, cyclic antidepressants, cocaine
- Side effects: Extreme lipemia, acute pancreatitis, acute respiratory distress syndrome
Supportive Care
Most Important Aspect of Treatment:
- Supportive care is the cornerstone of toxicology management
- Similar to care for other critically ill patients
- Focus on maintaining organ function while toxin is eliminated
Specific Management Issues:
Drug-Associated Agitated Behavior: Z
- First-line: Benzodiazepine administration
- Adjunct: High-potency neuroleptics (e.g., haloperidol) as needed
- Avoid: Physical restraints when possible (may worsen hyperthermia)
General Supportive Measures:
- Airway protection - early intubation when indicated
- Hemodynamic support - fluids, vasopressors as needed
- Temperature control - cooling or warming measures
- Seizure control - benzodiazepines first-line
- Electrolyte management - correct abnormalities
- Cardiac monitoring - continuous ECG monitoring
Disposition
Emergency Department Observation:
- Indications: Mild toxicity, low predicted severity
- Duration: 4-6 hours observation period
- Discharge criteria: Asymptomatic with normal vital signs and mental status
Admission Indications:
- Moderate observed toxicity or risk of developing toxicity
- Location: Intermediate-care floor or appropriate observation unit
- Monitoring: Continued monitoring and treatment
ICU Admission Criteria:
- Severe toxicity
- Hemodynamic instability
- Respiratory failure requiring mechanical ventilation
- Need for enhanced elimination techniques
- Requirement for multiple antidotes or continuous infusions
Psychiatric Evaluation:
- All intentional overdoses require psychiatric assessment
- Timing: After medical stabilization
- Documentation: Capacity, safety planning, follow-up arrangements
Summary and Key Points
Emergency Department Approach:
- Common ED problem - systematic approach essential
- Look for toxidrome - patterns guide diagnosis and treatment
- ABC first - airway, breathing, circulation
- ECG mandatory - provides diagnostic and prognostic information
- Paracetamol and aspirin levels - when indicated
- Antidotes - use when available and indicated
- Supportive care - cornerstone of management
Remember:
- Polydrug overdoses may present with mixed or confusing syndromes
- When in doubt, provide supportive care and consult toxicology/poison control
- Consider underlying psychosocial issues in all intentional ingestions