Approach to Head Trauma
Dr Abdulaziz Alrabiah, MD
Overview
- Definition: An insult to the brain from an external mechanical force, potentially leading to an altered level of consciousness and permanent or temporary impairment of cognitive, physical, and psychosocial functions.
- Accounts for of trauma deaths.
- Leading cause of disability under the age of 40 years.
- Bimodal distribution:
- Young adult males (Risk takers – occupation).
- Elderly (Risk of fall).
Causes
- Mechanisms: Blunt or penetrating.
- Common Etiologies:
- Falls (Most common cause).
- MVC (Cause of most TBI deaths).
- Violence and assaults (Increase nowadays).
- Industrial accidents.
- Sport.
- Special Considerations:
- Non-accidental Injury (NAI) in children = Abuse.
- Elder abuse (دور الرعاية).
- Domestic violence (Couples and always make sure that the wife is not Pregnant).
Classification of Brain Injury
Primary Brain Injury
- Occurs at the time of the traumatic incident direct cellular and tissue injury.
- Note: Cannot be prevented post-event (“I can’t prevent it”).
Secondary Brain Injury (can be prevented)
- Occurs days after the insult if the primary injury is not treated well.
- Further cellular damage.
- Major determinant of neurological outcome.
Grading of Head Injury
- Mild
- GCS 14-15.
- Brief LOC, nausea, cognitive, behavioural, and emotional disturbance.
- Moderate
- GCS 9-13 after non-surgical resuscitation.
- Severe
- GCS < 8 after non-surgical resuscitation.
Glasgow Coma Scale (GCS)
| Glasgow Coma Score | ||
|---|---|---|
| Eye Opening (E) | Verbal Response (V) | Motor Response (M) |
| 4 = Spontaneous | 5 = Normal conversation | 6 = Normal |
| 3 = To voice | 4 = Disoriented conversation | 5 = Localizes to pain |
| 2 = To pain | 3 = Words, but not coherent | 4 = Withdraws to pain |
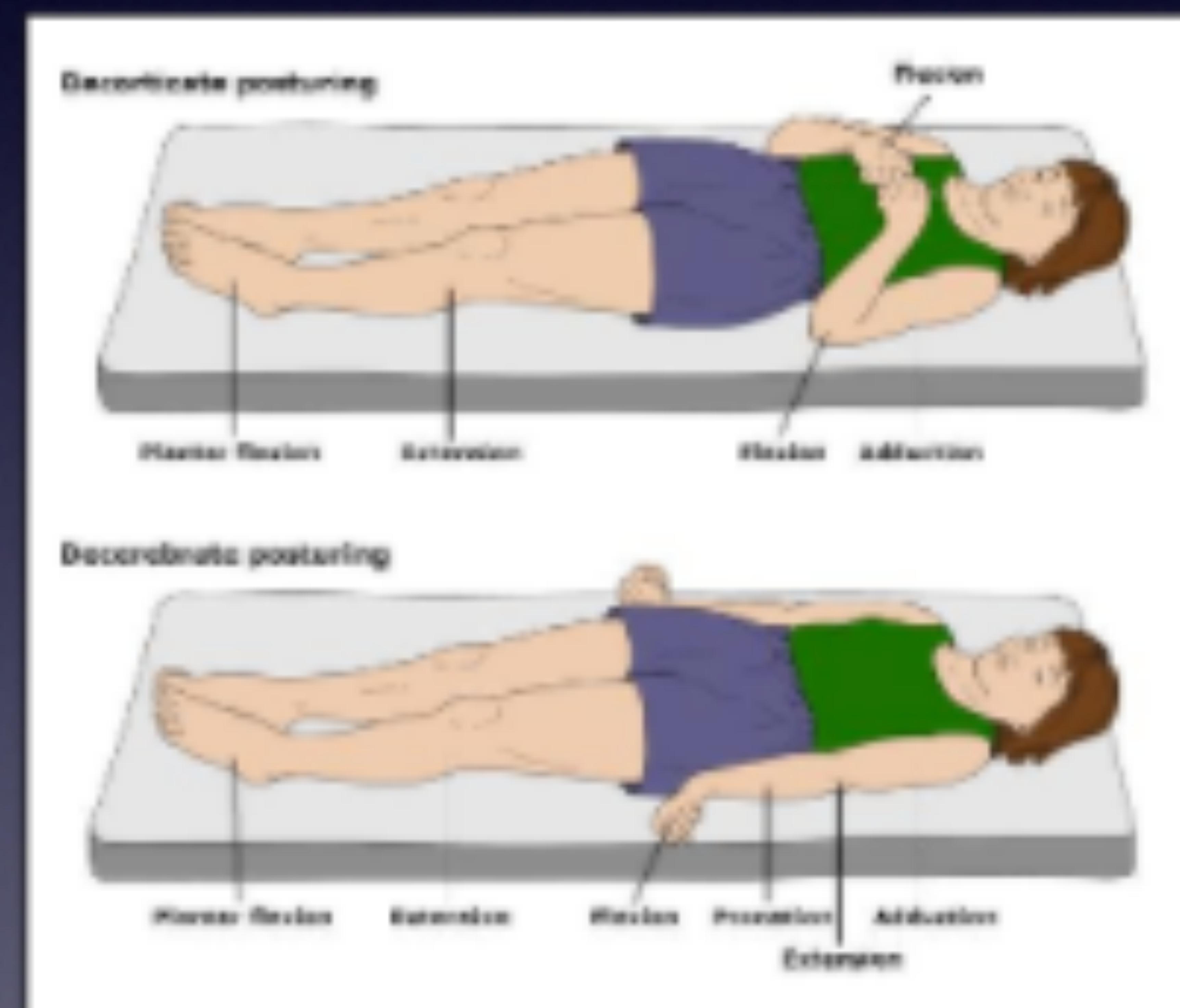
| 1 = None | 2 = No words… only sounds | 3 = Decorticate posture |
| 1 = None | 2 = Decerebrate | |
| 1 = None | ||
| Total = E + V + M |
Indication for Imaging (CT/MRI)
Definite Indications
(Examples)
- LOC for > 5 minutes.
- Focal neurological findings.
- Seizure.
- Failure of mental status to improve over time in an alcohol-intoxicated patient.
- Penetrating skull injuries.
- Signs of a basal or depressed skull fracture.
- Coagulopathy.
- Previous shunt-treated hydrocephalus.
- Infants and children.
- Age > 60.
(Note: “Names only”)
New Orleans Criteria
- Headache.
- Vomiting.
- Age > 60 yrs.
- Drug or alcohol intoxication.
- Deficits in Short Term Memory (STM).
- Evidence of trauma above the clavicles.
Canadian CT Head Rules
High Risk Features (for neurological intervention)
- GCS < 15 for 2 hours post injury.
- Suspected open or depressed skull fracture.
- More than 2 episodes of vomiting.
- Physical evidence of basal skull fracture.
- Age > 65.
- Coagulopathy.
Medium Risk Features (for brain injury detection)
- Antero-grade amnesia for more than 30 min prior to injury.
- Dangerous mechanism:
- Pedestrian vs motor vehicle.
- Ejection from vehicle.
- Fall from > 3 feet.
Specific Types of TBI
Skull Fracture
- From contact force.
- Usually associated with a brief loss of consciousness.
- Linear: Lateral convexities of skull.
- Depressed: Blunt force from an object with a small surface area (e.g., hammer).
- Compound fracture: Open fracture.
- Basal Skull Fracture (BOS): Severe blunt trauma to forehead or occiput.
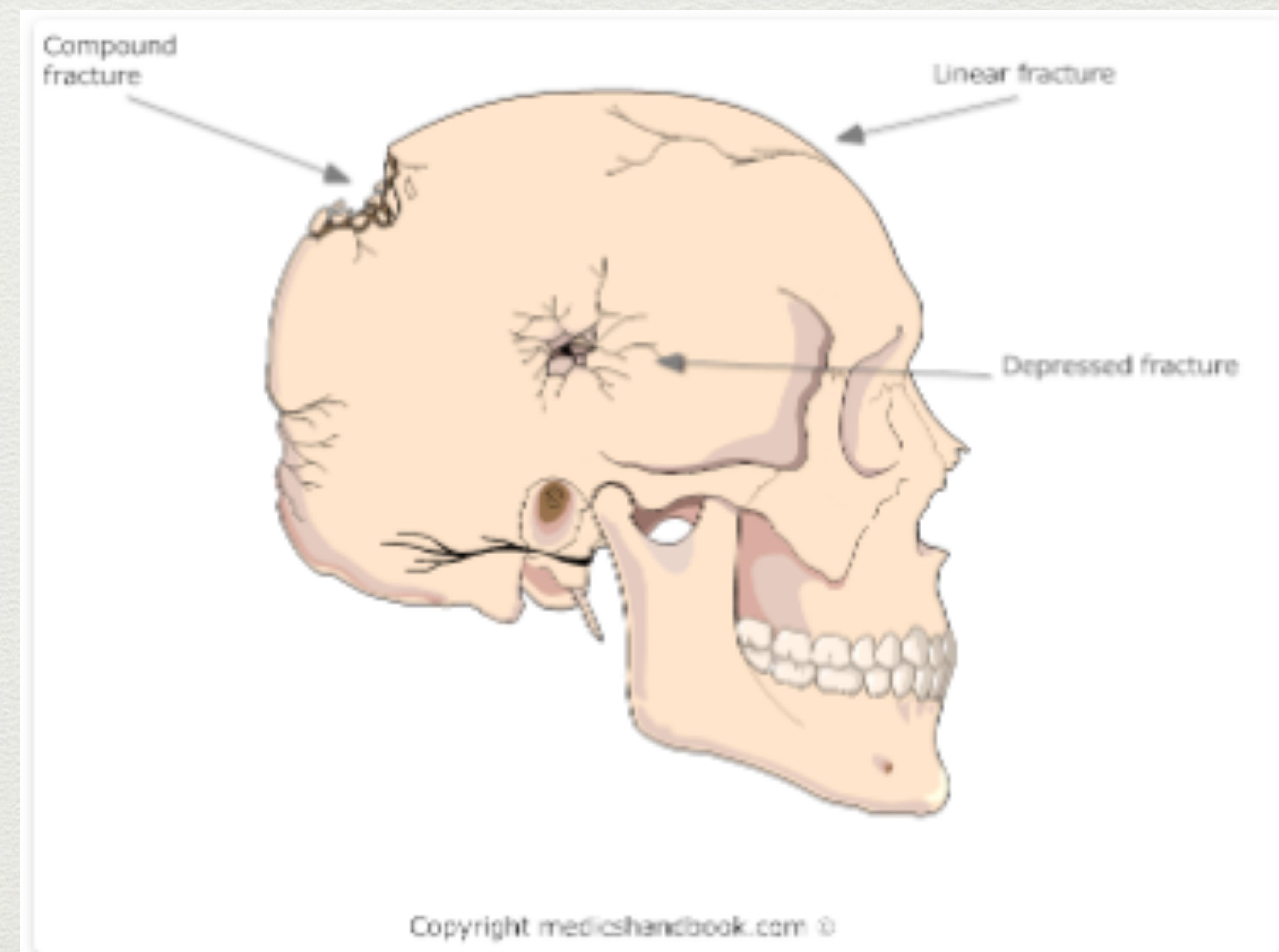 Diagram illustrating types of skull fractures.
Diagram illustrating types of skull fractures.
Subdural Haematoma (SDH)
- Tearing of bridging veins.
- Common in age y/o (mild trauma causes injury because brain shrinkage makes veins fragile).
- Doesn’t expand to contralateral hemisphere.
- Often associated with cerebral contusion underneath.
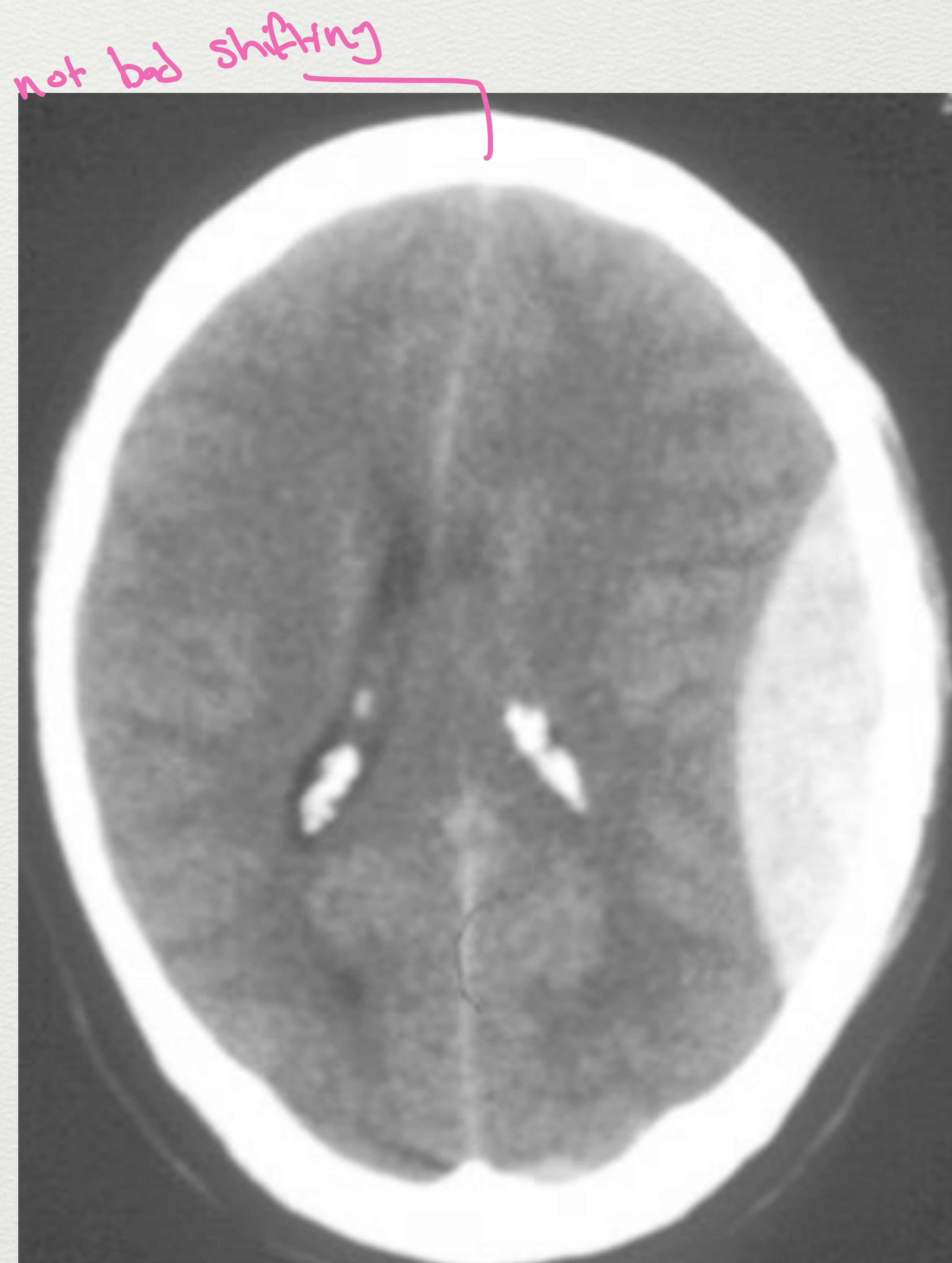
- Appearance: Crescent shape (Moon Shape) + shifting of midline.
 Axial CT scan showing a subdural hematoma as a crescent-shaped hyperdense collection.
Axial CT scan showing a subdural hematoma as a crescent-shaped hyperdense collection.
Epidural Hematoma (EDH)
- Usually from Middle Meningeal Artery tear with associated skull fracture.
- Most are temporal or parietal, but can occur in frontal and occipital lobes (rare in posterior fossa).
- Common in young adults.
- Appearance: Classic lenticular shape.
- Clinical Feature: Lucid Interval (Behaves totally normal then sudden deterioration/arrest).
- Risk: Brain herniation from Foramen magnum due to high pressure.
 Axial CT scan showing a large, hyperdense, biconvex (lenticular) epidural hematoma.
Axial CT scan showing a large, hyperdense, biconvex (lenticular) epidural hematoma.
Subarachnoid Haematoma (SAH)
- Does not produce a haematoma or mass effect.
- May cause post-traumatic vasospasm.
- Appearance: Star sign.
- Management: Conservative treatment.
 Axial CT scan showing subarachnoid haematoma (Star sign).
Axial CT scan showing subarachnoid haematoma (Star sign).
Cerebral Contusions
- Definition: Bruising / Swelling.
- Heterogenous lesions comprising of punctate haemorrhage, oedema, and necrosis.
- Do evolve over time (may not be visible on first CT) Normal.
- Can cause significant mass effect with herniation.
- May cause headache elevated ICP and coma.
Diffuse Axonal Injury (DAI)
- Mechanism: Injury at the level of myelin sheath/axons.
- Lacerations or punctate contusions at the interface between grey and white matter.
- Caused by a rotational vector of injury.
- Common cause of persistent vegetative state or prolonged coma.
- Diagnosis: Often a diagnosis of exclusion (“Rule out everything”) or pathological diagnosis by sample.
Management of TBI
Initial Resuscitation
- Seek and Treat ABC.
- Airway: Intubation if GCS 8 or below.
- Breathing: Treat hypoxia (Target sat ).
- Circulation: Treat hypotension (Fluid, blood, vasopressor).
- Target: SBP mmHg, MAP mmHg.
- Vasopressors mentioned:
- Adrenalin / Nor-adrenalin
- Epinephrin / Dopamin
Measures to Decrease Secondary Brain Injury
- Positioning: Head elevation degrees (gravity helps decrease fluid/ICP).
- Sedation and analgesia.
- Paralysis: If intubated.
- Ventilation: Maintain 30-35 mmHg.
- Causes vasoconstriction Cerebral Blood Flow (Note: text says flow/ICP, but physiology suggests constriction CBF/ICP. Preserved original implied logic of “constriction”).
- Osmotherapy:
- Mannitol: 1 gm/Kg (Diuretic).
- Hypertonic saline: 3%, 3ml/kg over 30 min.
- Surgical: De-compressive craniotomy (Remove bone flap until recovery, 6 months - 1 year).
- General Measures:
- Avoid hyperthermia.
- Seizure prophylaxis (Note: no evidence of benefit).
- DVT prophylaxis (TEDS, heparin/clexane within 2-3 days of injury).
Contact: aalrabiah@ksu.edu.sa