Approach to Trauma Patient
Dr. Abdulaziz Alrabiah, MD
Objective
- Fun part of Emergency Medicine (EM)
- Primary Survey
- Secondary Survey
- Investigations in each survey
Why is it the fun part?
- Everyone tries to participate
- Well-structured approach
- Courses available (EMST, ATLS)
Primary Survey
Goal: Ensure the patient is not in a life-threatening situation. If you find a pathology at any step, do not proceed to the next step unless you correct the pathology.
A: Airway and C-Spine Immobilization
Assessment:
- Evaluate for patent airway.
- If the patient is able to talk clearly → patent airway (i.e., clear from obstruction).
- Pathology Check:
- Visible foreign body (FB).
- Bleeding.
- Stridor (e.g., expanding neck hematoma).
Management:
- Remove visible FB.
- Suction blood.
- Intubation if stridor is present.
- Caution: If FB is not visible, do not try blindly to remove it.
C-Spine Immobilization:
- Must be immobilized (e.g., application of C-collar, foam pads taped to forehead, or ask the patient to keep still).
- If C-spine is fractured, keep neck immobilized. Once airway is patent, move to Breathing.
Immobilization Methods:
- Single Immobilization (C-Collar): Patient is less immobilized; there is still a ~20% chance of movement.
- Backboard: More stable.
- Multiple Methods: Foam pads + Neck Collar + Backboard is better.
Image showing a patient immobilized on a backboard using multiple methods: foam pads, a neck collar, and a backboard, resulting in greater stability, most importantly conscious to be told dont move
B: Breathing
Assessment:
- Paradoxical movement of chest wall segment: The opposite of normal; chest wall moves in with inspiration and out with expiration (Flail chest/Fracture).
- Tracheal deviation.
- Chest wall tenderness.
- Equal air entry bilaterally.
Pathology: Tension Pneumothorax
- Definition: Air in Pleural Cavity.
- Diagnosis: Clinical diagnosis.
- Signs: Tachycardia, hypotension, tracheal deviation to opposite side, decreased air entry on the same side, hyper-resonant to percussion. (Heart competition + Low oxygen saturation = Tension Pneumothorax).
- Treatment:
- Needle decompression: 5th intercostal space, mid-axillary line.
- Chest drain insertion: 5th intercostal space, between anterior and mid-axillary line.
 Anterior chest wall landmarks: Angle of Louis, Mid-clavicular line, Anterior axillary line, Mid-axillary line.
Anterior chest wall landmarks: Angle of Louis, Mid-clavicular line, Anterior axillary line, Mid-axillary line.
C: Circulation and Bleeding Control
Assessment:
- Vital signs: Pulse, Blood Pressure (BP).
- Skin color.
- Peripheral pulses: Check presence in Upper & Lower limbs (See all 4 pulses).
Management:
-
Control Bleeding:
- Direct pressure (The Best).
- Limb elevation.
- Vascular clamp.
- Tourniquet: Apply proximal to the wound (Max 2 hours to avoid skin changes).
-
IV Access:
- Place two large IV access points (14G, 16G, 18G).
- Peripheral: Small, direct to heart.
- Intraosseous (IO): If peripheral fails (proximal tibia, humerus).
- no Central: Femoral, subclavian (Time-consuming, requires antiseptic procedure).
-
Fluid Replacement:
- Ringer’s Lactate > Normal Saline (to avoid hyperchloremic metabolic acidosis).
- Give 1 L. If no response → Start blood transfusion.
- Do not give another 1 L of crystalloid (prevents dilution and coagulation problems).
- Massive Transfusion Protocol: RBC, PLT, FFP at ratio of 1:1:1.
-
Tranexamic Acid (TXA):
- Give within the first 3 hours of trauma.
- Dose: 1g IV stat, then 1g infusion over 8 hours.
-
Coagulopathy:
- Reverse anticoagulants if any.
- Monitor coagulation (TEG or ROTEM).
Access Types:
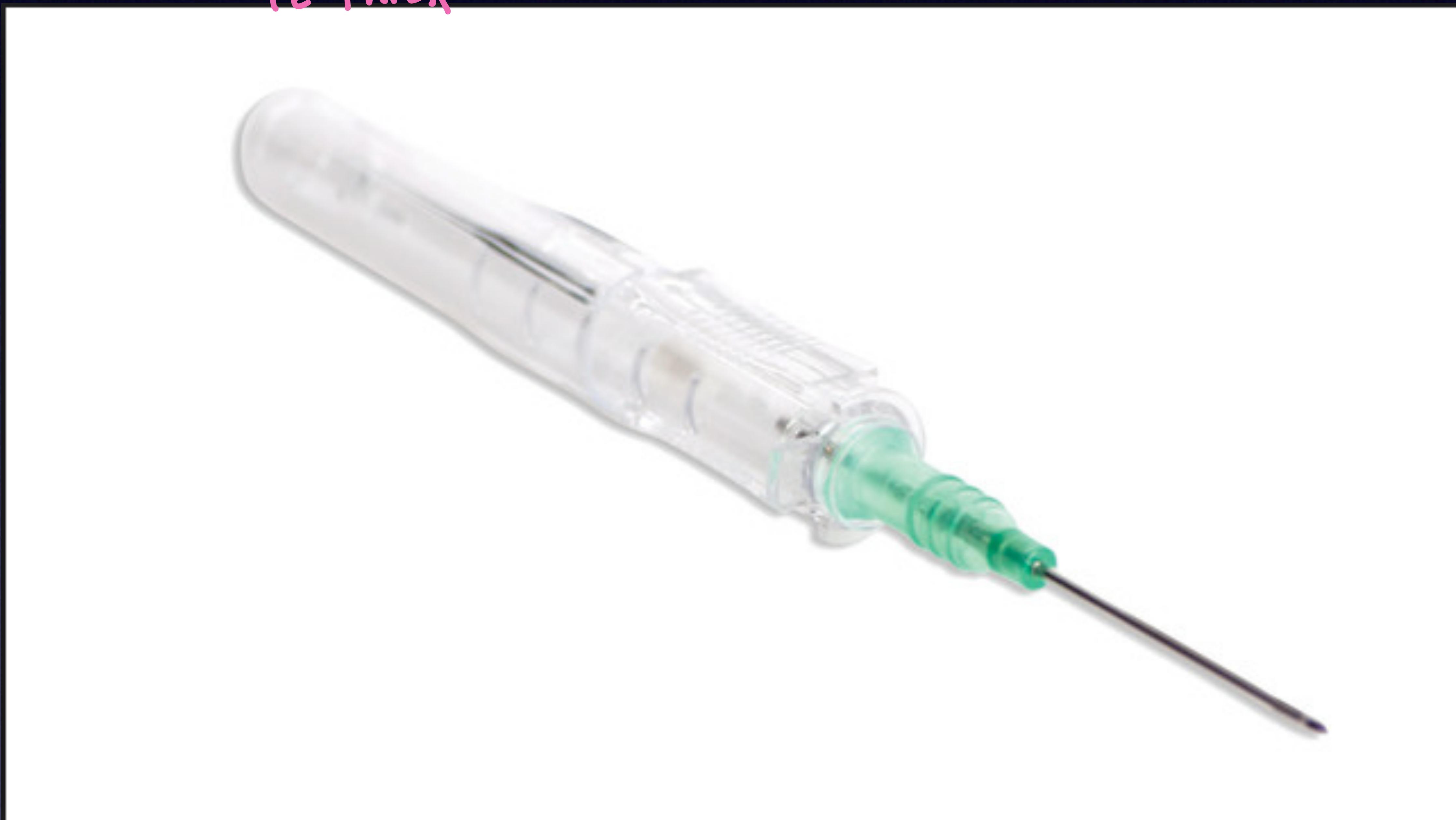 Peripheral IV catheter.
Peripheral IV catheter.
 Intraosseous kit: Drill, Needles (Yellow/Adult, Blue/Pediatric), and connection tubing.
Intraosseous kit: Drill, Needles (Yellow/Adult, Blue/Pediatric), and connection tubing.
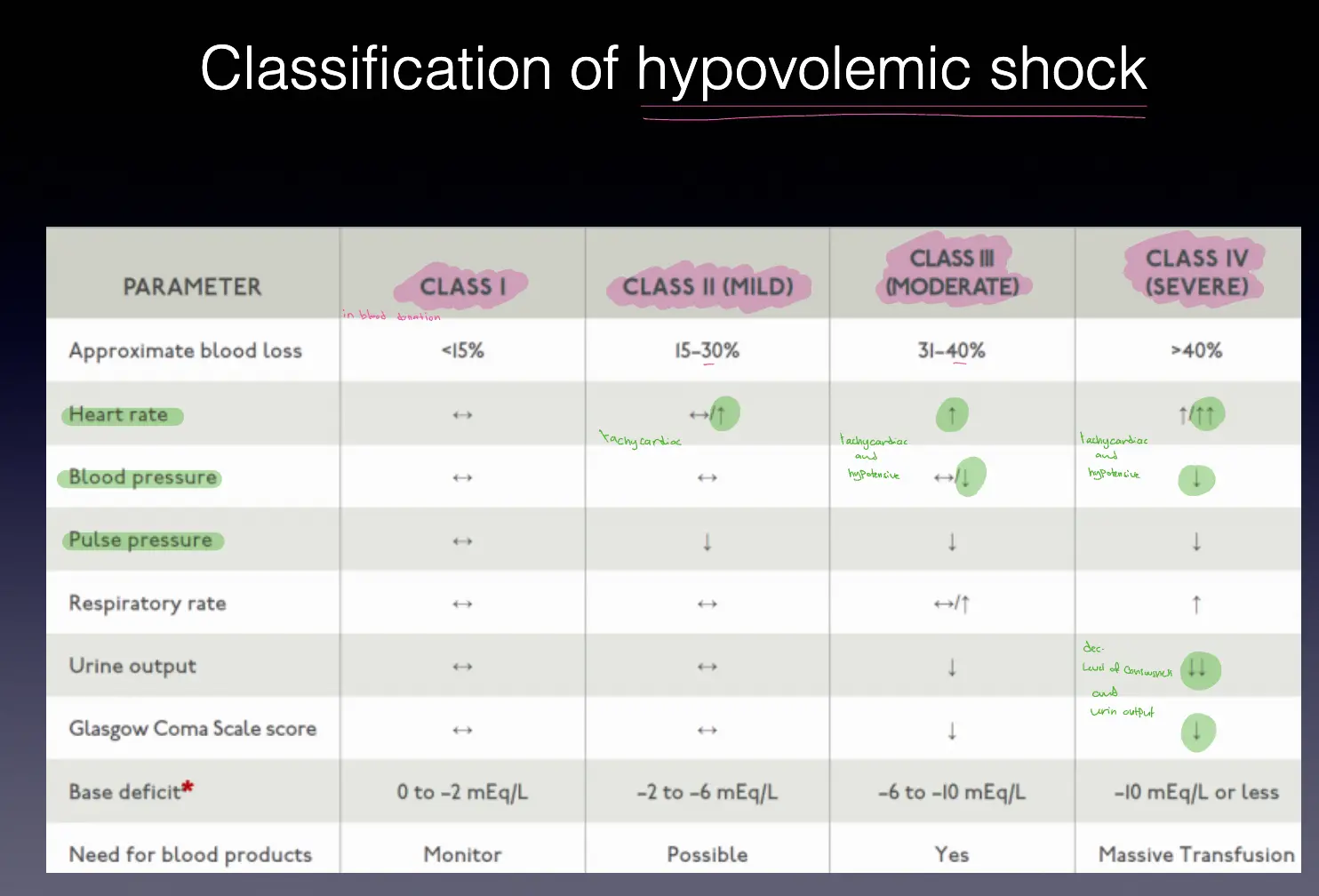
Classification of Hypovolemic Shock:
| PARAMETER | CLASS I | CLASS II (MILD) | CLASS III (MODERATE) | CLASS IV (SEVERE) |
|---|---|---|---|---|
| Approximate blood loss | <15% | 15-30% | 31-40% | >40% |
| Heart rate | ↔ | ↔/↑ | ↑ | ↑↑↑ |
| Blood pressure | ↔ | ↔ | ↔/↓ | ↓ |
| Pulse pressure | ↔ | ↓ | ↓ | ↓ |
| Respiratory rate | ↔ | ↔ | ↔/↑ | ↑ |
| Urine output | ↔ | ↔ | ↓ | ↓↓ |
| Glasgow Coma Scale | ↔ | ↔ | ↓ | ↓ |
| Base deficit | 0 to -2 | -2 to -6 | -6 to -10 | -10 or less |
| Need for blood | Monitor | Possible | Yes | Massive Transfusion |
D: Disability (Neurology)
Two-Part Exam:
-
GCS (Glasgow Coma Scale): Level of consciousness.
- Max score: 15.
- Min score: 3.
- Severity: Mild (14-15), Moderate (9-13), Severe (<8).
- Action: If GCS ≤ 8 → Intubate.
-
Pupil Exam:
- Normal: 3 mm, equal and reactive to light.
- Unequal pupils in trauma usually indicates bleeding.
Glasgow Coma Score Table:
| Glasgow Coma Score | ||
|---|---|---|
| Eye Opening (E) | Verbal Response (V) | Motor Response (M) |
| 4 = Spontaneous | 5 = Normal conversation | 6 = Normal |
| 3 = To voice | 4 = Disoriented conversation | 5 = Localizes to pain |
| 2 = To pain | 3 = Words, but not coherent | 4 = Withdraws to pain |
| 1 = None | 2 = No words (only sounds) | 3 = Decorticate posture |
| 1 = None | 2 = Decerebrate | |
| 1 = None | ||
| Total = E + V + M |
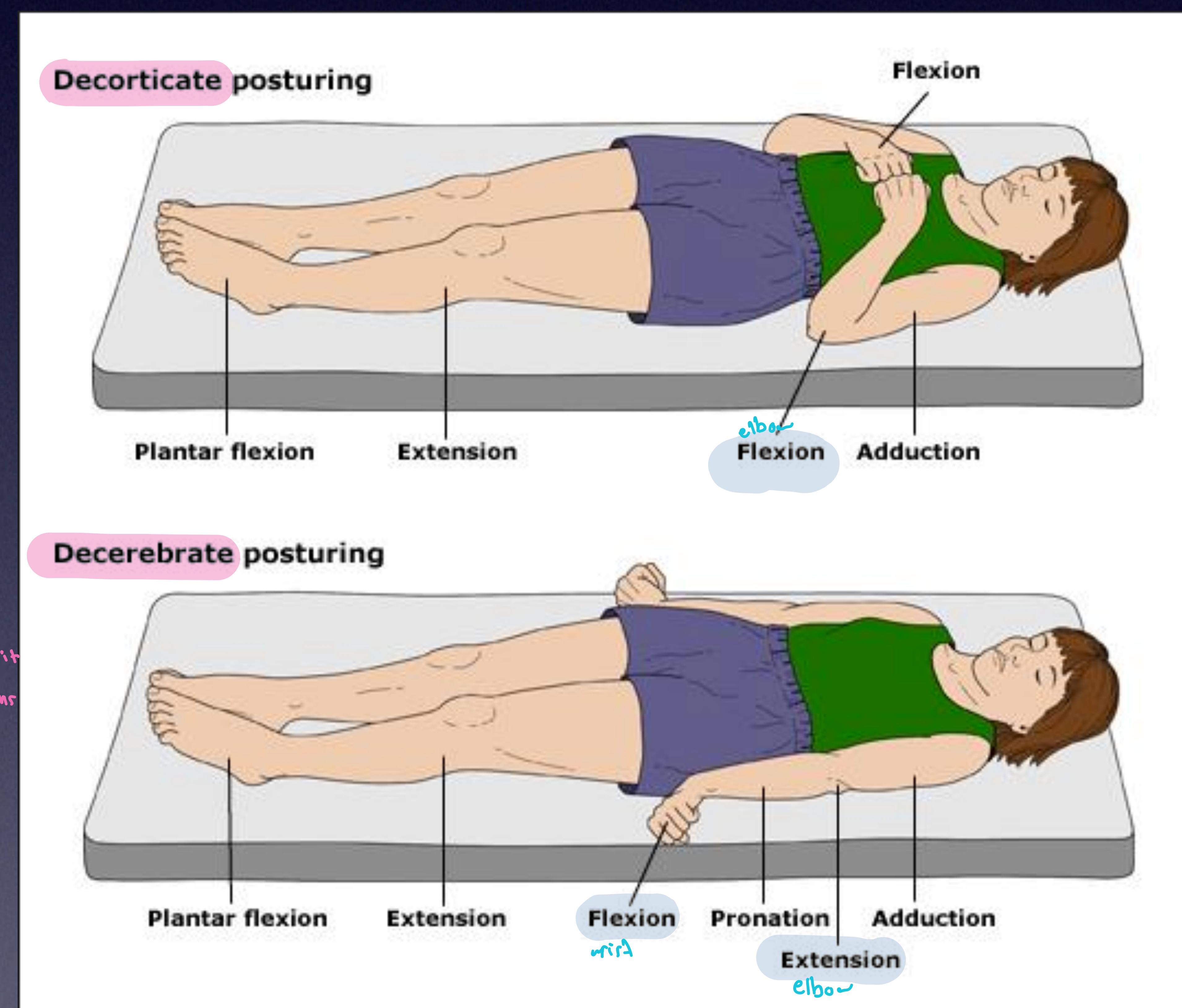 Top: Decorticate posturing (Flexion). Bottom: Decerebrate posturing (Extension).
Top: Decorticate posturing (Flexion). Bottom: Decerebrate posturing (Extension).
Case Example: 17 y/o girl involved in MVA.
- Opens eyes to name call (3)
- Confused when asked (4)
- Localizes to pain (5)
- GCS = 12
E: Exposure
- Expose the patient (cut clothes) to look for any injury, bruises, or deformity.
- Prevent Hypothermia: Immediately cover the patient.
- Correct correctable pathology (e.g., reduce deformed limb).
The 3 Killers in ER:
- Hypothermia
- Acidosis
- Coagulation Problems
Adjuncts to Primary Survey
Investigations
1. BGL (Blood Glucose Level)
- Do not ever forget glucose!
2. X-ray
- Chest X-ray
- Pelvic X-ray
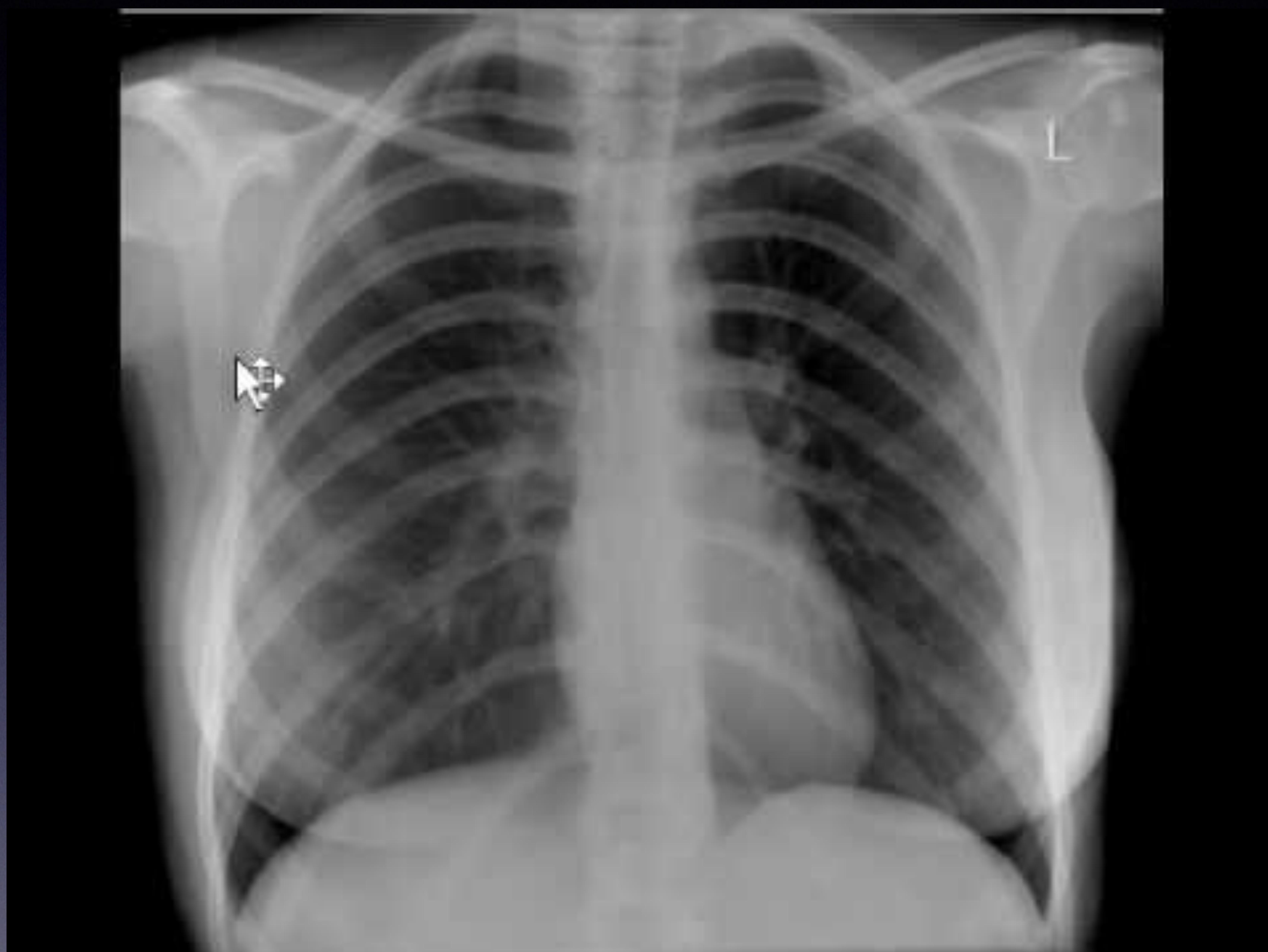 Anteroposterior chest X-ray showing a suggestive pulmonary nodule/mass.
Anteroposterior chest X-ray showing a suggestive pulmonary nodule/mass.

3. eFAST Scan
- Ultrasound of Chest and Abdomen.
- Aim: Detect pneumothorax, intraperitoneal bleed, and pericardial effusion.
RUQ Scan (Morrison’s Pouch)
Liver and Kidney interface.
normal
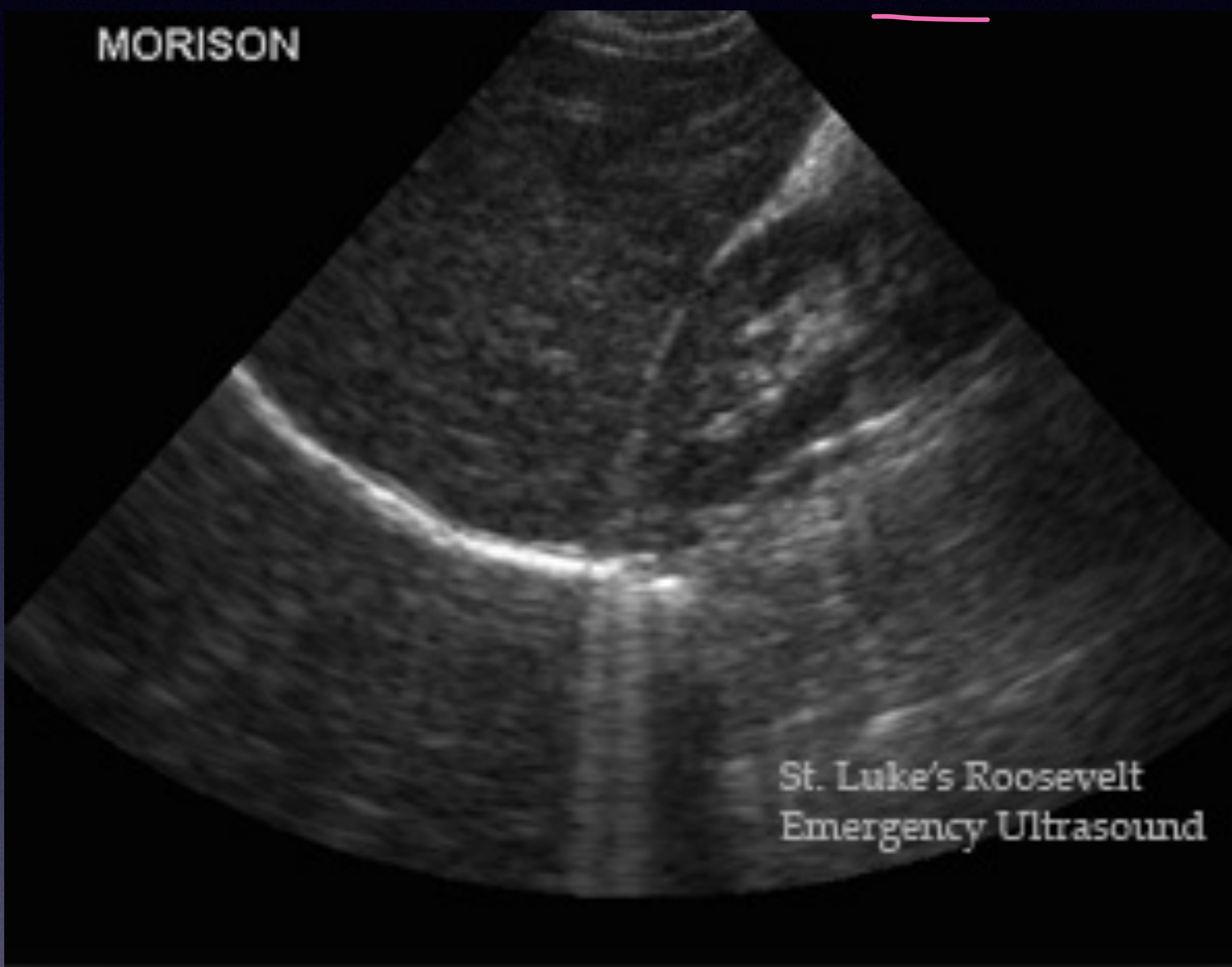 Normal Morrison’s pouch.
Normal Morrison’s pouch.
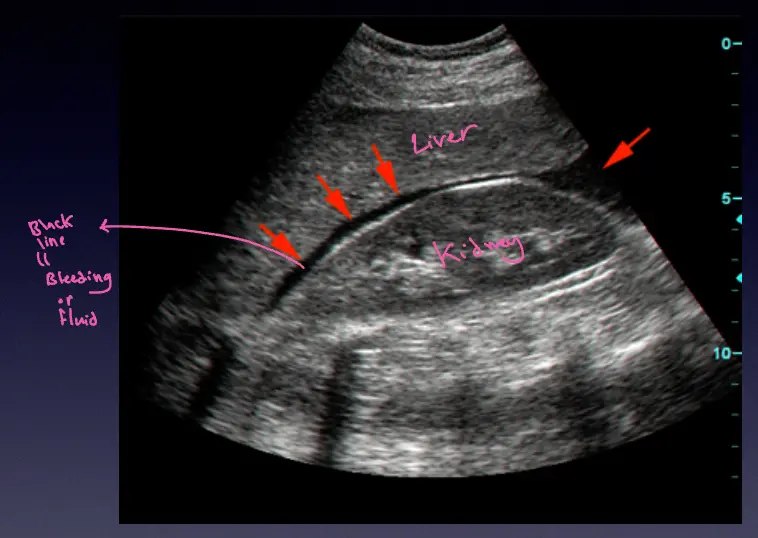 bleeding
bleeding
LUQ Scan (Splenorenal)
Spleen and Kidney interface.
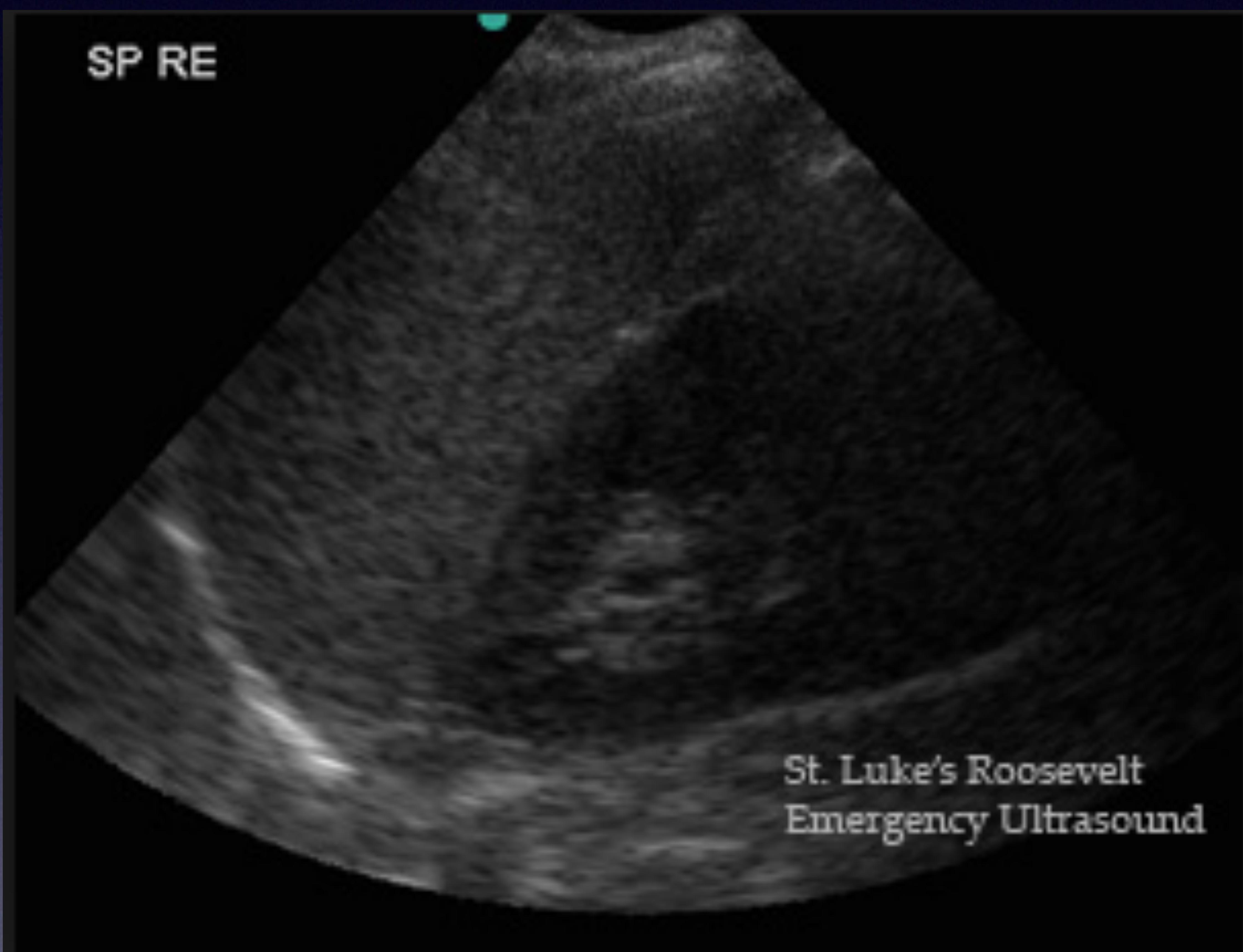 Splenorenal view.
Splenorenal view.
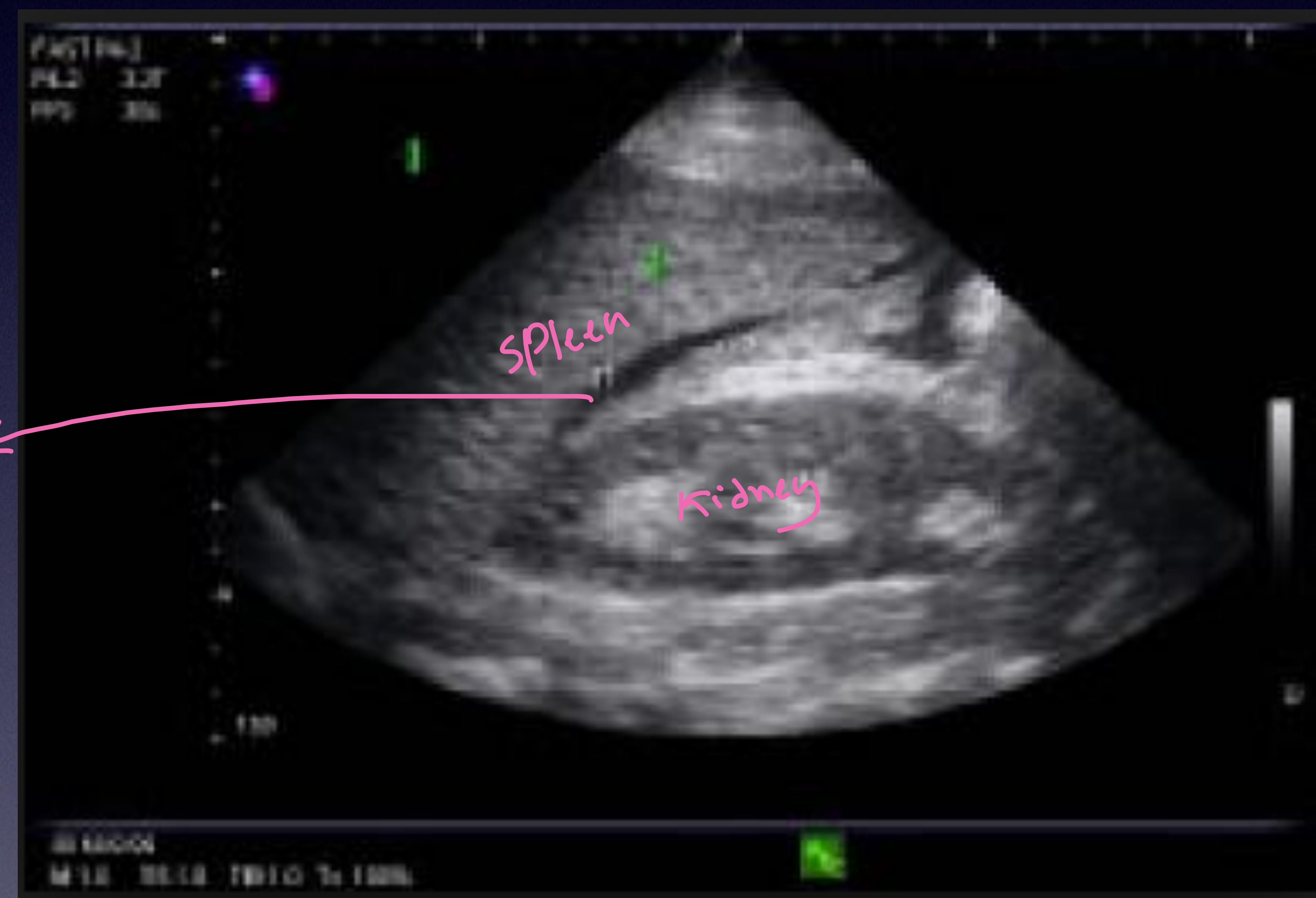 Spleen, Kidney, and Blood.
Spleen, Kidney, and Blood.
Bladder Scan (Suprapubic)
Midway between umbilicus and pubic bone.
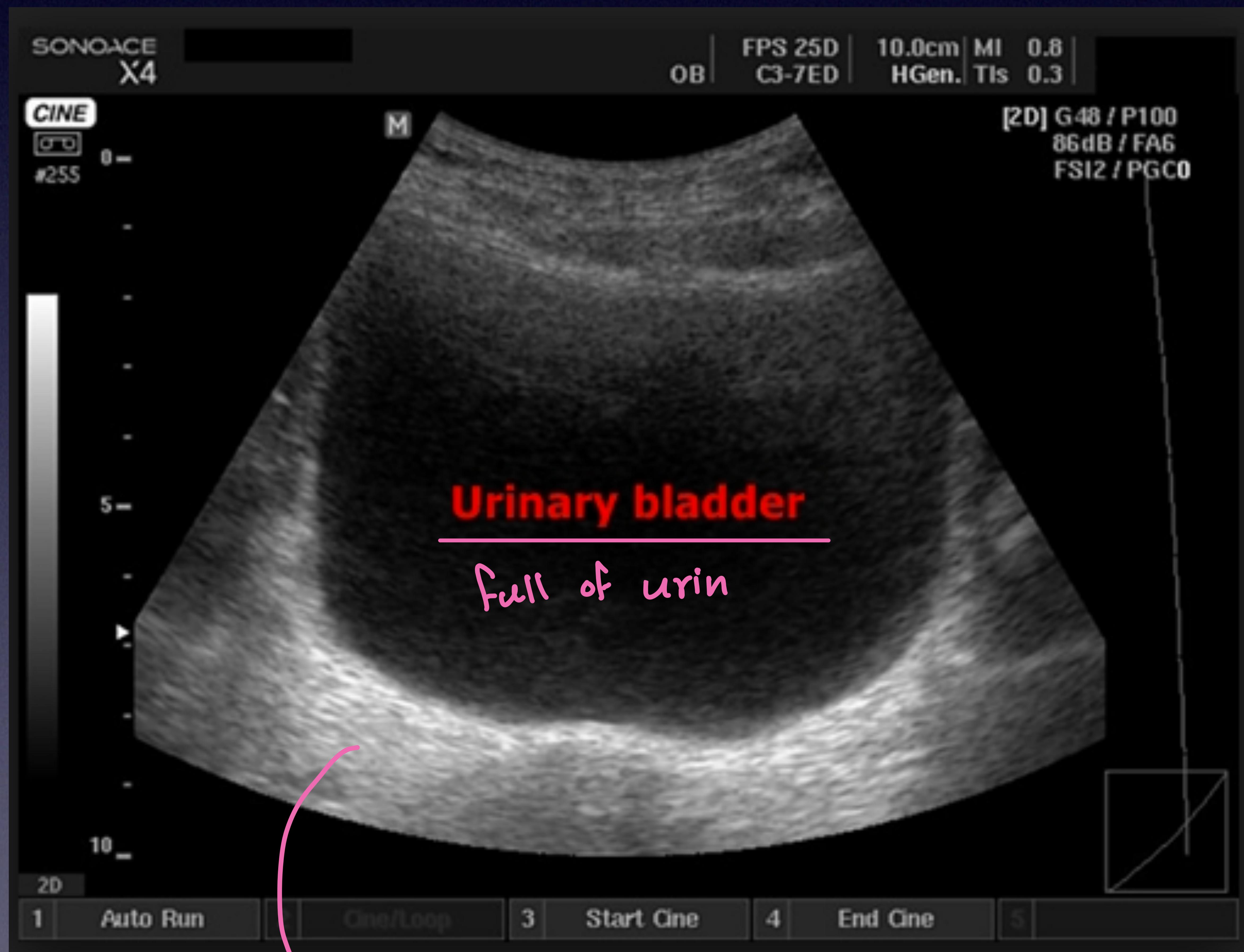 Bladder full of urine (transverse view).
Bladder full of urine (transverse view).
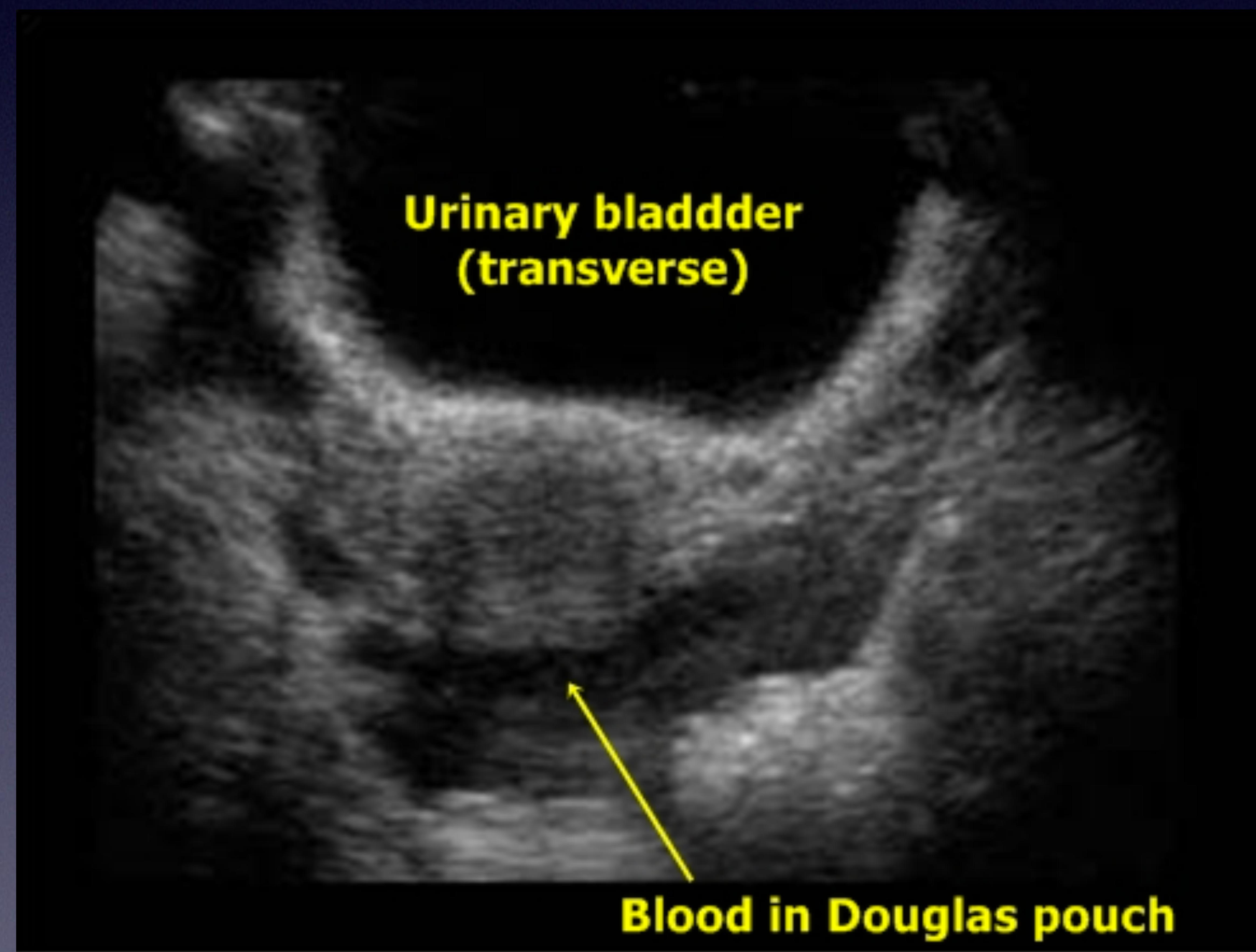 Blood in Douglas pouch (inferior to bladder).
Blood in Douglas pouch (inferior to bladder).
Pericardial Scan
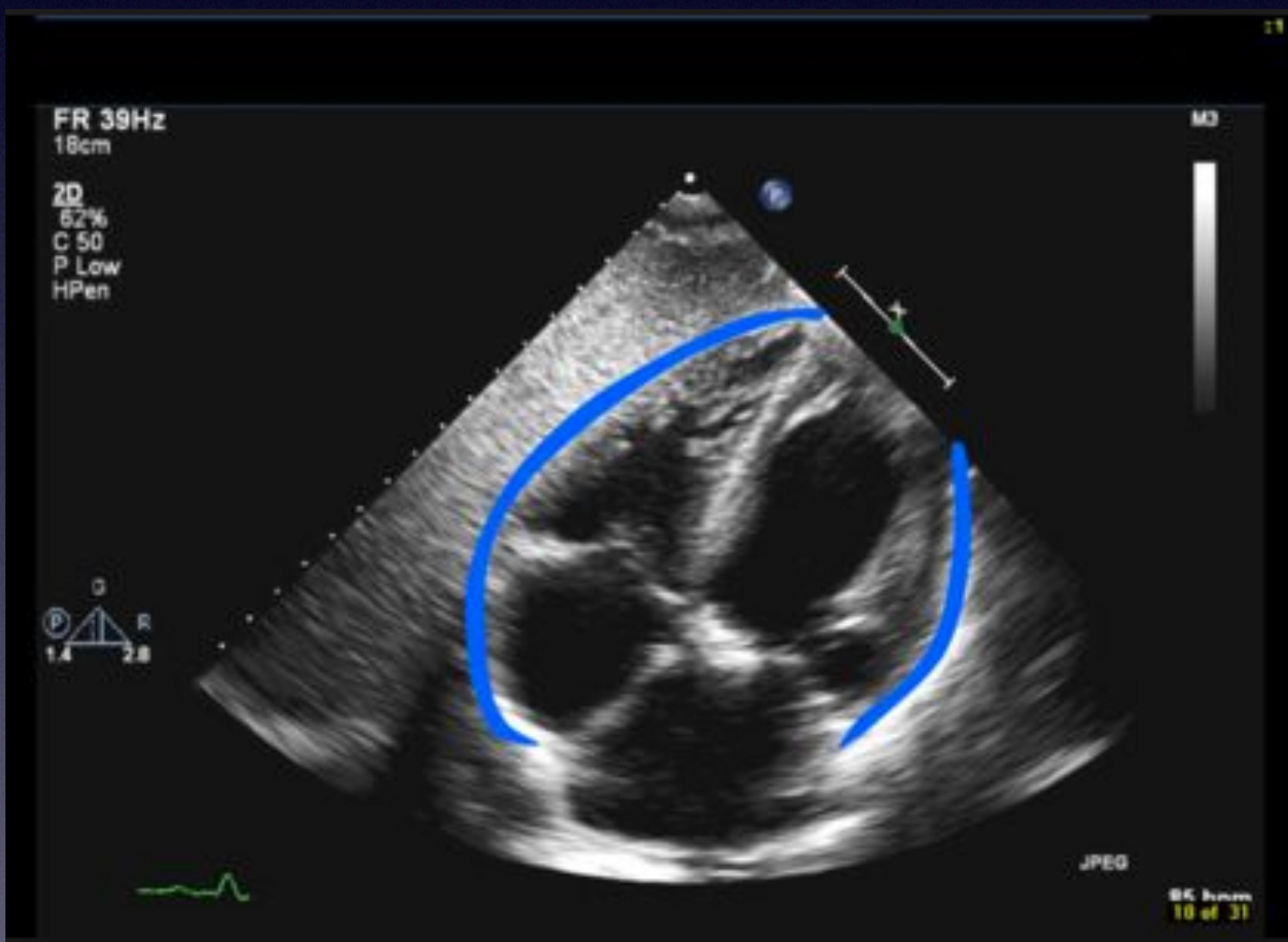 Pericardial space showing fluid accumulation (effusion).
Pericardial space showing fluid accumulation (effusion).
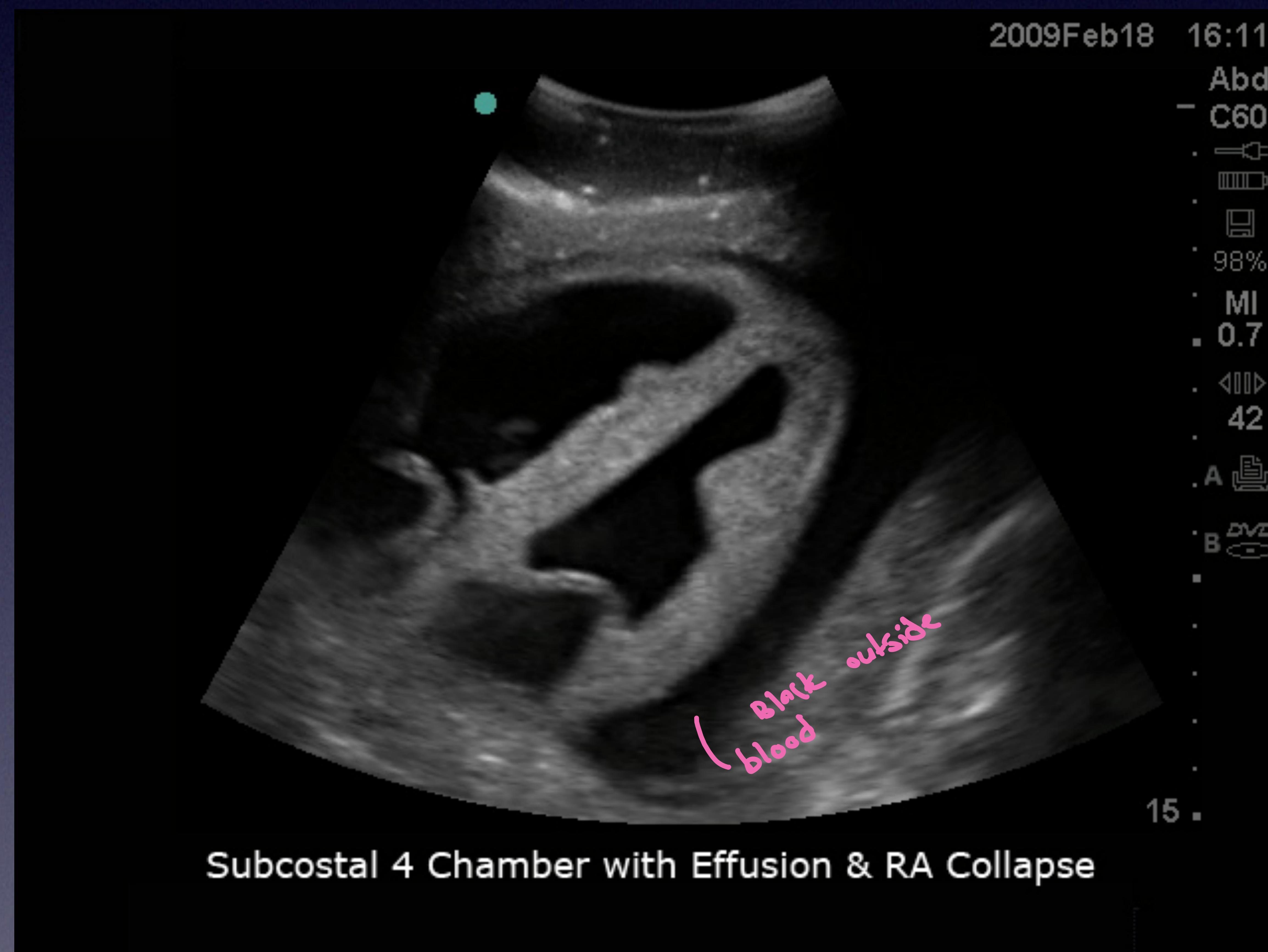 Subcostal 4 Chamber view with Effusion & RA Collapse.
Subcostal 4 Chamber view with Effusion & RA Collapse.
Lung Scan
- Normal: Sliding sign, Seashore Sign (M-mode).
- Pneumothorax: No sliding sign, Barcode/Stratosphere Sign (M-mode).
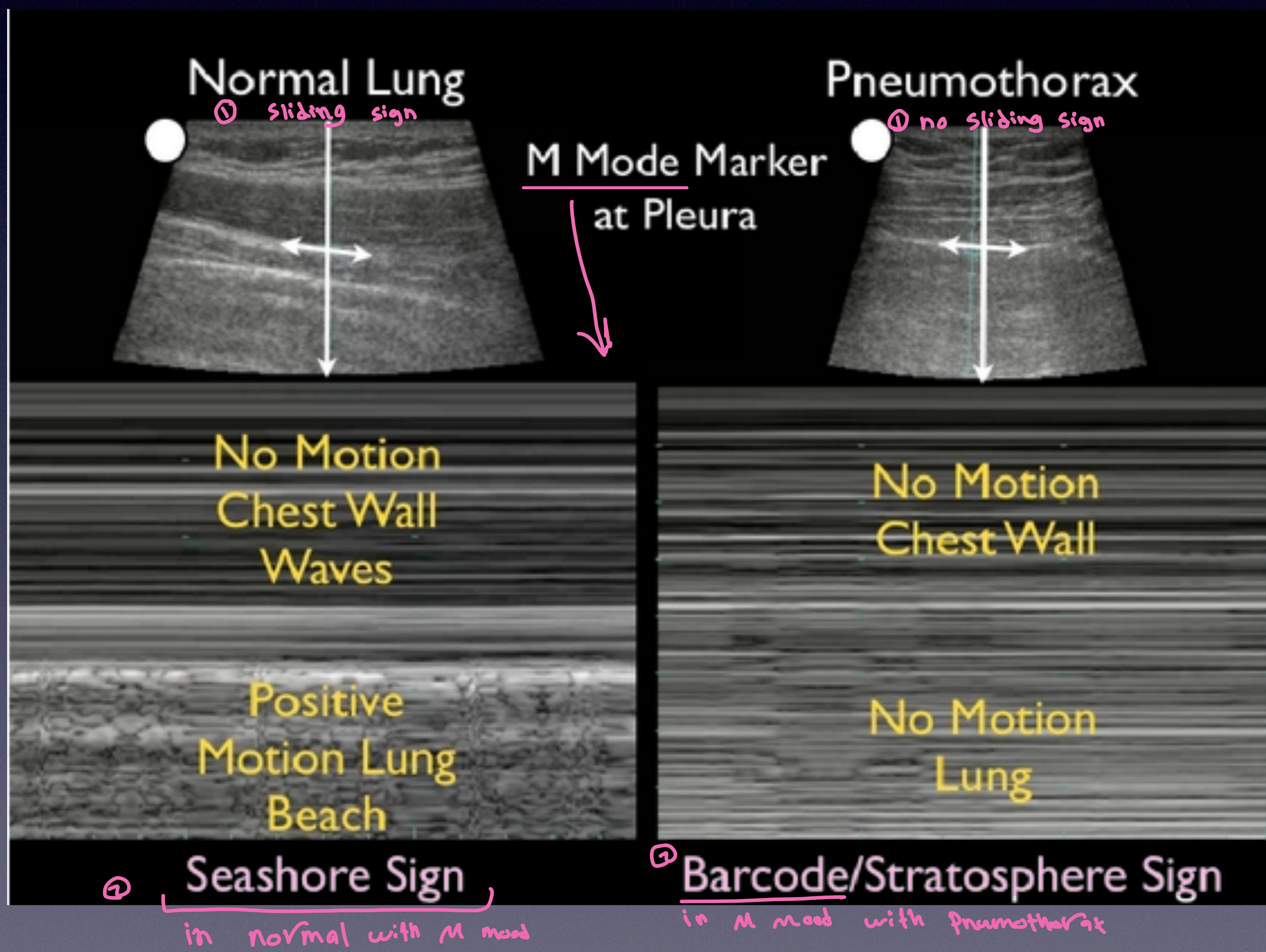 Comparison of Normal Lung (Seashore sign) vs Pneumothorax (Barcode sign).
Comparison of Normal Lung (Seashore sign) vs Pneumothorax (Barcode sign).
Present seashore & barcode - normal
Secondary Survey
Goal: Once life-threatening conditions are managed, proceed with details.
- AMPLE History
- Head to Toe Exam
History (AMPLE)
- A: Allergy
- M: Medications
- P: Past medical/Surgical History, Pregnancy
- L: Last meal and drink
- E: Event (Mechanism of injury)
Head & Face Exam
- Check for: Laceration, bleeding, deformity, missing teeth, CSF leakage.
- Signs:
- Raccoon’s eye: Periorbital ecchymosis.
- Battle sign: Mastoid ecchymosis.
 Severe facial trauma showing Raccoon’s eye sign.
Severe facial trauma showing Raccoon’s eye sign.
 Battle sign (bruising behind the ear) indicative of basilar skull fracture.
Battle sign (bruising behind the ear) indicative of basilar skull fracture.
Neck Exam
- Bruise, wound, bleeding.
- Hematoma (expanding).
Chest Exam
- Re-evaluate Primary Survey findings.
- Cardio exam.
- Chest wall tenderness.
Abdomen Exam
- Bruise, wounds.
- Distension, tenderness.
Pelvis Exam
- Lateral compression of pelvis to check for instability (at greater trochanter, not ASIS).
Genital Exam
- Blood at urethral meatus indicates urethral injury.
- Do NOT insert urinary catheter blindly.
- Action: Perform retrograde urethrogram or suprapubic catheter.
Upper and Lower Limb Exam
- Deformity.
- Pulse (loss of pulse).
- Motor and sensory function.
Back Exam
- Log Roll: Need 4 people.
- Spine exam: Top to bottom, looking for spinal tenderness, deformity.
- Check for wounds, lacerations, bruises.
- Rectal Exam: Generally not needed (“don’t do rectal exam” - likely useless). Sensation check and asking patient to squeeze is usually sufficient.
 Medical team performing a log roll.
Medical team performing a log roll.
Adjuncts to Secondary Survey
- X-rays (Limbs)
- CT scans
- Blood tests
- Group and Save blood
- Urine test (Blood and Pregnancy)
Review Questions
Q1: A 32-year-old male involved in MVC brought to ED by ambulance complaining of left-sided chest pain. How do you approach this patient? A: Follow the ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure).
Q2: What are the adjuncts to Primary Survey? A:
- Blood Gas / BGL
- ABG (implied/often included)
- Labs / Lung scan
- X-Ray (Chest, Pelvis)
- eFAST (extended Focused Assessment with Sonography in Trauma)
Q3: What are the areas of eFAST? A:
- RUQ (Right Upper Quadrant)
- LUQ (Left Upper Quadrant)
- Suprapubic (Bladder)
- Chest (Lung)
- Pericardiac (Heart)
Contact:
- Email: aalrabiah@ksu.edu.sa
- Twitter: @azizalrabiah