Aspirin Toxicity
Fahad Abuguyan, MBBS, MBA, FRCPC
Assist Prof. Emergency Medicine
Overview
Principle of the disease
Clinical features
Diagnosis
Management
Overview
- Salicylates are profoundly toxic and can be fatal in large quantities.
- Salicylate overdose requires active assessment and treatment measures only. There is no antidote for any of these drugs.
- Salicylism should be considered in the differential diagnosis of altered mental status in the elderly.
Aspirin remains a common:
- Analgesic
- Antiplatelet therapy for patients with IHD
Sources of salicylate:
- Aspirin.
- Many over-the-counter combination medications contain aspirin.
- Topical products.
Principle of the disease
Mechanism of action:
Inhibition of cyclooxygenase results in decreased synthesis of
- Prostaglandins
- Prostacyclin
- Thromboxanes
Absorption and metabolism:
- Rapidly absorbed.
- Peak blood concentrations are usually reached within one hour.
- Aspirin is metabolized in the liver.
- Half-life of two to four hours.
At therapeutic levels, 90% of salicylate is protein bound and therefore limited to the vascular space.
Typical clinical presentations:
- Suicide attempt.
- Chronic overdose in patients chronically using aspirin (often elderly with multiple medical comorbidities).
salicylism will usually present as a mimic
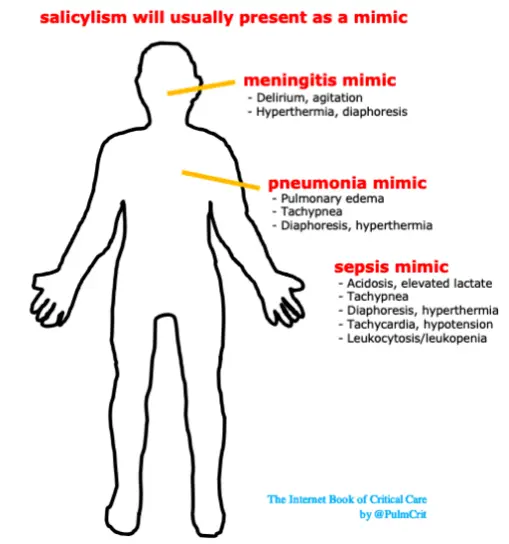
ASA toxicity can cause:
- CNS symptoms
- Acute Kidney injury and renal failure
- ASA-induced pulmonary edema
- Tinnitus
signs & symptoms
- General
- Tachypnea
- Tachycardia
- Diaphoresis
- Hyperthermia
- Neurologic
- Tinnitus, vertigo, ataxia, deafness
- Delirium, agitation, lethargy
- Seizure, coma
- GI
- Nausea/vomiting
- Diarrhea
- Can cause gastritis with hematemesis
- Pulmonary
- Non-cardiogenic pulmonary edema
Acid-base abnormalities:
Acid-base status can suggest salicylate toxicity, but cannot exclude it. Note also that patients with co-ingestion may not manifest with classic acid/base patterns (e.g. aspirin plus opioids may not lead to a respiratory alkalosis).
- (1) First finding is respiratory alkalosis.
- Salicylate affects the medulla directly, increasing respiratory drive.
- (2) Second, an anion-gap metabolic acidosis develops as well, creating a mixed picture.
- Metabolic acidosis reflects increases in keto-acid, salicylic acid, and lactic acid.
(3) Respiratory Acidosis:
- This is often a pre-terminal event (reflecting respiratory exhaustion, ARDS, or severe CNS dysfunction).
- Can also occur with co-ingestion of substances that reduce respiratory drive.
- Acidemia promotes entry of salicylate into the brain, worsening the intoxication.
Diagnosis
High index of suspicion.
Vital signs!!!
Think of ASA toxicity in any case with:
- Unexplained pulmonary edema
- Acute change in level of consciousness
- Mixed acid-base disturbance
Toxic dose of aspirin:
150 to 300mg/kg
Lethal dose :
500mg/kg
Labs:
CBC
Renal Profile with electrolytes
VBG
SERUM ASA LEVEL
UA
LFTs
Lactate
Coagulation Profile
- Hypoglycemia
- Hyperglycemia
- Hypokalemia
- Thrombocytopenia
- DIC
- Renal failure
In patients with mixed acid-base disturbance always think of ASA toxicity
Serum salicylate:
- Therapeutic serum salicylate concentrations fall between 10 to 30 mg/dL (0.7 to 2.2 mmol/L).
- Values above 40 mg/dL (2.9 mmol/L) are associated with toxicity.
- Serum salicylate levels should be repeated every 2 hours until three consecutive levels are both mg/dL and are decreasing by at least 10% to 20% on each measurement while no longer undergoing therapy to enhance elimination.
Fatal aspirin toxicity can occur after the ingestion of 10 to 30 grams by adults and as little as 3 g by children
Generally ASA toxicity does not correlate exactly with serum salicylate concentrations and symptoms.
But..
most patients exhibit signs of intoxication when the serum concentration exceeds 40 to 50 mg/dL (2.9 to 3.6 mmol/L)
Monitoring serum salicylate concentrations
may help:
- Assess the response to therapy
- Determine the need for more aggressive measures, including hemodialysis.
Levels above 100 mg/dL (7.2 mmol/L) are associated with increased morbidity and mortality, and are considered an absolute indication for hemodialysis.
Management
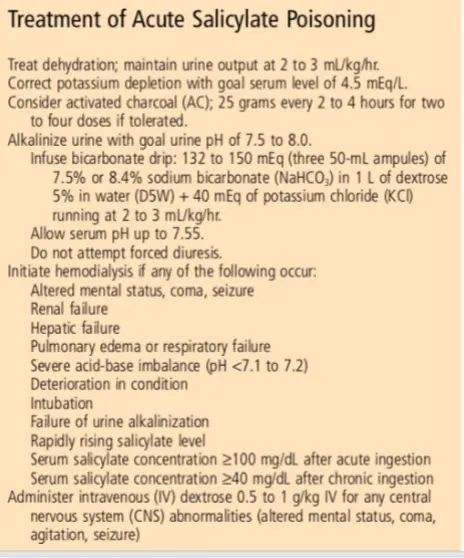
Treatment of salicylate poisoning has two main objectives:
- 1st is to correct fluid deficits and acid-base abnormalities
- 2nd is to increase excretion.
Airway and breathing:
Intubation is indicated only for patients with:
- Refractory shock
- Pulmonary or cerebral edema
- Other manifestations of severe salicylate poisoning.
Activated Charcoal:
Activated charcoal (AC), in a single dose or multiple doses, somewhat reduces salicylate absorption.
May be used within 1 hour of ingestion with large lethal dose provided the airway is well protected.
Intravenous fluids:
Aggressive volume resuscitation is warranted in such patients, unless cerebral edema or pulmonary edema is present.
Potassium depletion must be corrected.
-
Enhanced elimination through urinary alkalization with a sodium bicarbonate drip should be initiated in acute toxicity with a level mg/dL ( mmol/L).
-
Consultation with nephrology and preparation for hemodialysis should occur if the salicylate concentration is mg/dL ( mmol/L) or is rising rapidly.
-
Glucose infusion with CNS symptoms
-
Correct electrolytes, i.e. K, Mg
-
Vitamin K if hypoprothrombinemia
-
Sodium bicarbonate for severe acidosis or before intubation
Hemodialysis is recommended for signs of pulmonary or cerebral edema, coma, seizures, hepatic failure, renal failure, circulatory collapse, or refractory acidosis along with acute levels greater than 100 mg/dL (7 mmol/L) and chronic levels of 40 mg/dL (3 mmol/L).
Treatment of Acute Salicylate Poisoning
Disposition:
In patients with acute intoxication, hospital admission is required for:
-
Pulmonary edema
-
CNS symptoms.
-
Seizures.
-
Acidosis.
-
Electrolyte disorders
-
Dehydration
-
Renal insufficiency
-
Increasing serum levels during serial testing.