Mohammed Alageel
Bronchial asthma
Goals
- Review burden of disease
- Review pathophysiology of airway obstructive disease
- Review the subtypes of asthma disease
Entomology
- Greek “ασυμα”, signifying panting, and was used initially as a synonym for “breathlessness.”
- Subsequent definitions of asthma highlight concepts of airway hyper-responsiveness, bronchospasm, and reversible airway obstruction.
CONTENTS
BRONCHIAL
ASTHMA
- INTRODUCTION
- CLASSIFICATION
- RISK FACTORS
- Diagnosis
- Treatment & Prevention
Introduction
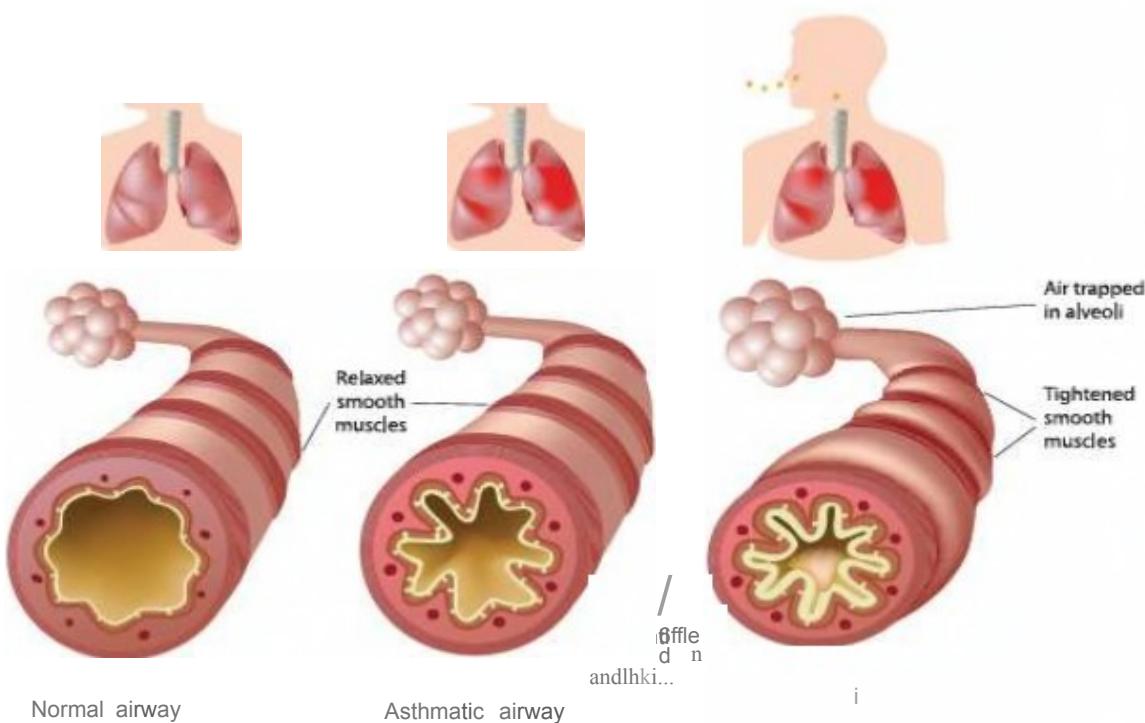
- Asthma is a chronic inflammatory disorder of the airways that is characterized: syndrom
clinically by recurrent episodes of wheezing, breathlessness, chest tightness, and cough, particularly at night/early morning.
physiologically by widespread, reversible narrowing of the bronchial airways and a marked increase in bronchial responsiveness. ↑ secretions, edema many cells and cellular elements play a role. With variable reversibility
Pathology
- Permanent structural airway changes (airway remodeling) may contribute to increased airway obstruction and hyper-responsiveness and decrease the response to therapy.
- This is routinely used to assess asthma and monitor the disease.
- Nitric oxide (NO) produced by airway epithelial cells in the large and small airways and alveoli is a reflection of ongoing airway inflammation.
- The American Thoracic Society (ATS) guidelines recommend FeNO as part of the initial diagnosis of asthma and for monitoring of airway inflammation. FeNO has also been shown to be a predictive factor for asthma exacerbations, with higher levels being associated with a greater number of exacerbations.
- Most asthma begins in childhood and resolves with age.
Burden of Disease
- In 2015, 358 million people globally had asthma, up from 183 million in 1990.
- It caused about 397,100 deaths in 2015, most of which occurred in the developing world.
- Asthma impacts patients, their families, and the community as a whole in terms of lost work and school days, poor quality of life, frequent emergency department (ED) visits, and hospitalizations
Age and race distribution
- Despite the advancements in the contemporary medicine, there are 40–70% of patients who have uncontrolled asthma
- Asthma impacts patients, their families, and the community in terms of lost work and school days, poor quality of life, frequent emergency department (ED) visits, and hospitalizations
- Asthma is more prevalent in children than adults, in females more than males and in African descent more than Caucasians and Hispanics
- Developed nations have higher rates of asthma, which suggests that urbanization and westernization are correlated with increased asthma prevalence.
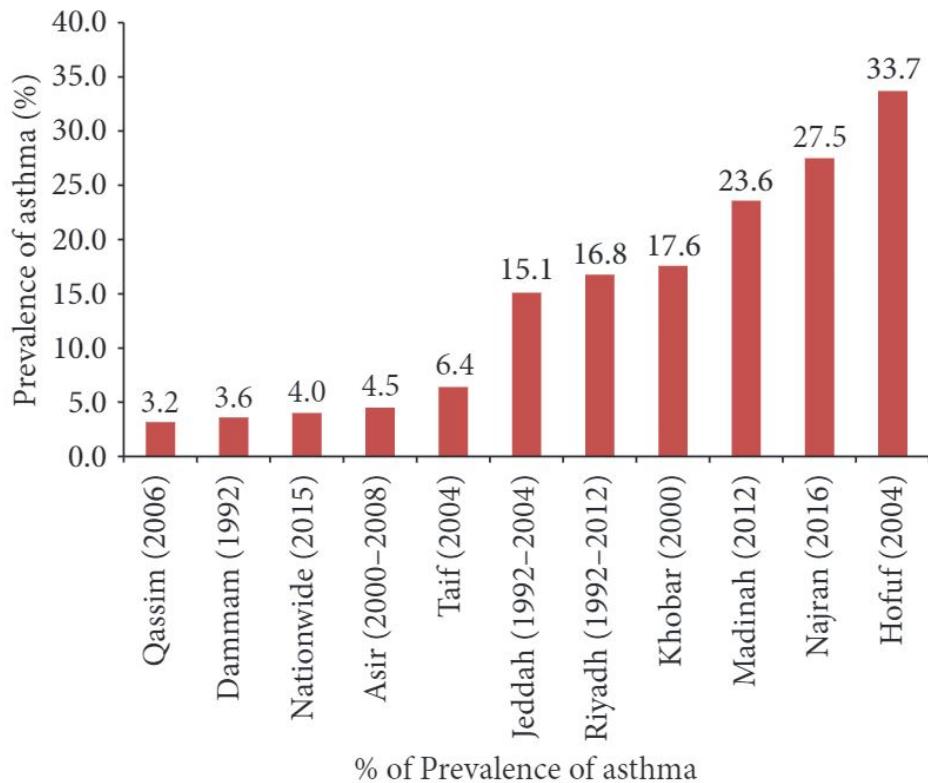
KSA asthma burden
- Asthma affects more than 2 million Saudis, and recent studies suggest that majority of them have uncontrolled asthma with their quality of life adversely being impacted
- prevalence of asthma to a host of factors including change in lifestyle, socioeconomic status, dietary habits and allergens, dust, tobacco smoke, sandstorms, and industrial and vehicular pollutants
- According to Ministry of Health, SA, the prevalence of asthma ranges from 15 to 25%
CLASSIFICATION
Classification
■ A heterogeneous disorder.
► Atopic /extrinsic /allergic ( 70%):
- Most common type
- Environmental agent: dust, pollen, food, animal dander → Cause Histamen release
- Family history - present
- Serum IgE levels - increased
- Skin test with offending agent - wheal flare
Classification
- Non-atopic/ intrinsic /non-allergic( 30%)
- Triggered by respiratory tract infection
- Viruses - most common cause
- Family history uncommon
- IgE level normal
- No associated allergy
- Skin tests NEGATIVE
- Cause- hyperirritability of bronchial tree
Classification
most of Asthmatic will not get worse with NSAIDs
Drug induced asthma aka Aspirin-exacerbated respiratory disease (AERD)
- Several pharmacologic agents
- Aspirin sensitive asthma
- Increased bronchoconstrictor leukotrienes.
- sensitive to small doses of aspirin.
- Inhibits COX pathway, without affecting LPO pathway
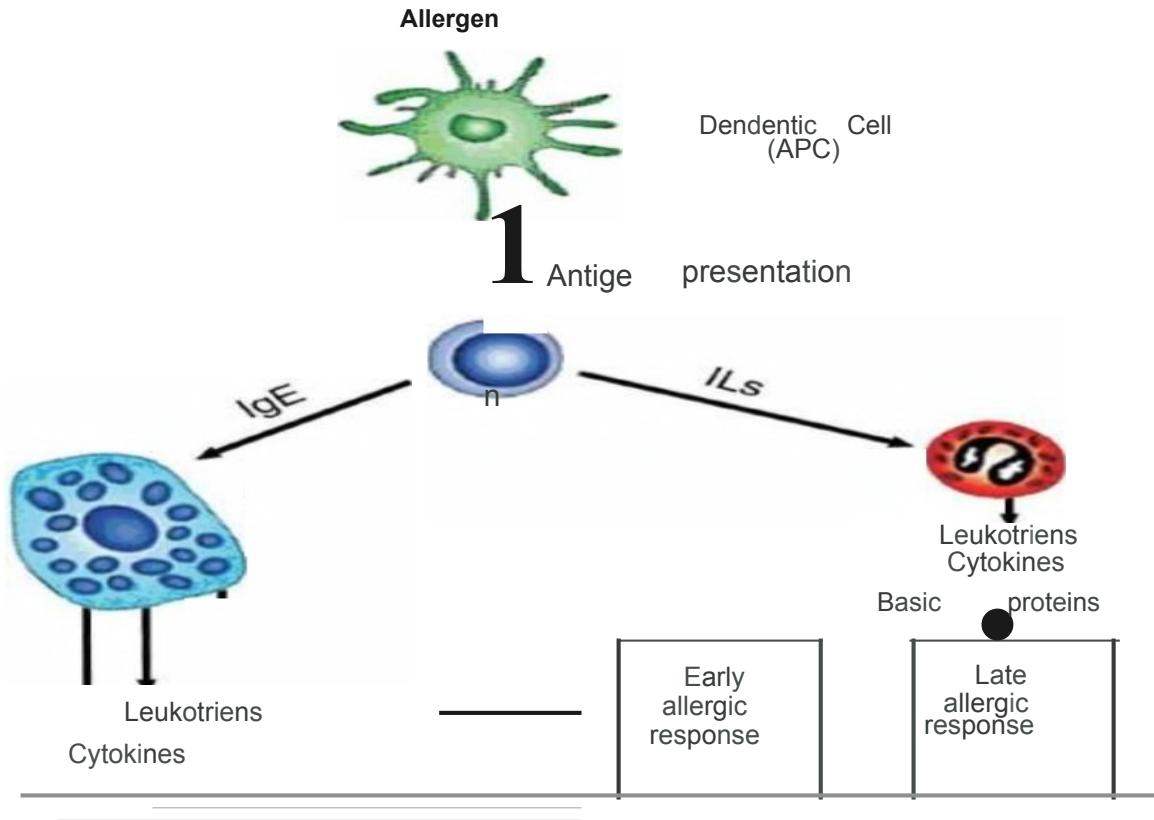
Pathophysiology
I. Chronic inflammation
II. Airway Hyperresponsiveness
asthma is not a single disease but a syndrome with various phenotypes.
Pathophysiology
I. Inflammation
-
Chronic inflammatory state
-
Involves respiratory mucosa from trachea to terminal bronchioles, predominantly in the bronchi. so there’s thickning of Airway
-
Activation of mast cell, infiltration of eosinophils & T-helper type 2 (Th2) lymphocytes
-
Exact cause of airway inflammation is unknown.
-
Thought to be an interplay between endogenous and environmental factors.
□ Endogenous factors
► Atopy
- Genetic predisposition to IgE mediated type I hypersensitivity
- The major risk factor for asthma
► Genetics
Environmental factors
- Viral infections: RSV, Mycoplasma, Chlamydia
- Air pollution
- Allergens :house dust mite
II. Airway Hyperresponsiveness (AHR)
- The excessive bronchoconstrictor response to multiple inhaled triggers that would have no effect on normal airways.
- Characteristic physiologic abnormality of asthma.
*Reversible disease
if we don’t treat it we’ll become Chronic
Pathophysiology
Risk factors
► Host factors:
- predispose individuals to, or protect them from, developing asthma
i. Genetic non-modifiable factor
-
o Atopy Same modifiable and the others non-modifiable
-
o Airway hyperresponsiveness
i i. Gender non-modifiable factor
iii. Obesity modifiable factor
Risk factors
➤ Environmental factors: Very Important to ask if it. the prevention could be the treatment.
- influence susceptibility to development of asthma in predisposed individuals, precipitate asthma exacerbations, and/or cause symptoms to persist
- Indoor allergens, Outdoor allergens
- Occupational sensitizers
- Tobacco smoke, Air Pollution
- Respiratory Infections
- Diet
Triggers
Asthma Triggers
- Allergens
- Virus Infections
- Drugs
- Exercise
- Food
- Air pollutants
- Physical factors
- GERD
- Stress
- Occupational factors
DIAGNOSIS
Clinical manifestations
➤ Symptoms
- Wheezing, dyspnea and cough.
- Variable – both spontaneously and with therapy.
- Symptoms worse at night.
- Nonproductive cough
- Limitation of activity
► Signs Hyperresonant
- ↑ respiratory rate, with use of accessory muscles
- Hyper-resonant percussion note
- Expiratory rhonchi abnormal lung Sound
- No findings when asthma is under control or b/w attacks
Classification for asthma severity
| Grade | Symptoms | Night-time Symptoms |
|---|---|---|
| Mild intermittent | Symptoms ≤ 2 times/week | ≤ 2 times/month |
| Mild persistent | Symptoms ≥ 2 times/week but ≤ 1/day | ≥ 2 times/month |
| Moderate persistent | Daily Symptoms | ≥ 1/week |
| Severe persistent | Continued Symptoms Limited physical activity | Frequent |
Clinical manifestations

Dyspnea

Weakness
Cough

Night cough
Wheezing

Headache

Tachycardia

Allergy

Shortness of breath

Laboratory diagnosis
Gold standard
Pulmonary function
tests: For diagnosis and evaluation of treatment responsiveness
- Using Spirometry
- estimate degree of obstruction
- FEV1, FEV1/FVC, PEF.

Laboratory diagnosis
Recently not needed we do it only if we think that it isn’t Asthma
➤ CXR: as well as Blood test
■ hyperinflation, emphysema
➤ Arterial blood-gas not Indicated
analysis(not useful generally)
■ hypoxia & hypocarbia
➤ Skin hypersensitivity test
➤ Sputum & blood eosinophilia
➤ Elevated serum IgE levels
monitoring
the disease
TREATMENT
Management
I. Non-Pharmacological
II. Pharmacological
Non-Pharmacological
- Reduce exposure to indoor allergens - SMR to avoid triggers
- Avoid tobacco smoke
- Avoid vehicle emission
- Identify irritants in the workplace
- Explore role of infections on asthma development, especially in children and young infants
Non-Pharmacological
Influenza Vaccination
- should be provided to patients with asthma when vaccination of the general population is advised
- routine influenza vaccination of children and adults with asthma does not appear to protect them from asthma exacerbations or improve asthma control
Prophylaxis
- Preservation of the environment, healthy life-style (smoking cessation, physical training) – are the basis of primary asthma prophylaxis. for weight loss
- These measures in combination with adequate drug therapy are effective for secondary prophylaxis.
Pharmacological treatment
Classification of drugs
-Bronchodilators : rapid relief, by relaxation of airway smooth muscle
- β2 Agonists
- Anticholinergic Agents
- Methylxanthines
- -Controllers : inhibit the inflammatory process
- Glucocorticoids
- Leukotrienes pathway inhibitors
- Cromones
- Anti-IgE therapy
in ER
β2 Agonists in asthma
- Potent bronchodilators.
- Usually given by inhalation route.
or mask - Effects: may cause tachycardia
Relaxation of airway smooth muscle
- Inhibition of mast cell mediator release
- Reduction in plasma exudation
- Increased mucociliary transport
- Inhibition of sensory nerve activation
No effect on airway inflammation
That’s why we don’t use it alone.
add Corticosteroid
a) Short-Acting Agonists E.g 2-3h salbutamol, terbutaline
Convenient, rapid onset, without significant systemic side effect
- Bronchodil. of choice in acute severe asthma
- Used for symptomatic relief
- Only treatment required for mild, intermittent asthma.
Use >2 times a week indicates need of a regular controller therapy. “Prophylactic therapy”
b) Long-Acting Agonists
- E.g salmeterol, formoterol
- Duration of action - >12 hrs.
- Used in combination with inhaled corticosteroid therapy.
- Improve asthma control and reduce frequency of exacerbations.
- Should not be used as monotherapy (increased mortality).
- Not effective for acute bronchospasm.
Instructions for Metered-Dose Inhaler (MDI) Use
make sure that pit is using it well
Box 73-3
- Remove cap from the MDI container.
- Assemble the MDI and hold it upright.
- Shake the canister.
- Place the mouthpiece loosely between the teeth (or hold it 3-4 cm in front of the open mouth).
- Exhale fully (to functional residual capacity).
- Actuate the inhaler at the beginning of a slow and full inhalation (as if sipping hot soup) lasting 5 or 6 seconds.
- Hold breath for at least 10 seconds.
- Wait 1 minute before reuse.
► Anticholinergic agents
not at home use only in hospital because of its side effect:
- Dysgeusia
- urine retention
- Myopia
E.g. Ipratropium bromide, tiotropium.
Prevent cholinergic nerve induced bronchoconstriction.
Less effective than agonists.
Response varies with existing vagal tone.
Use in asthma (not regular)
- Intolerance to inhaled agonist.
- Status asthmaticus – additive effect with agonist
■ Ipratropium:
- slow, bitter taste
- precipitate glaucoma
- paradoxical bronchoconstriction(rare)
■ Tiotropium:
- longer acting, approved for treatment of COPD.
- Dryness of mouth
► Methylxanthines use in refractory asthma pit
- Medium potency bronchodilator
- E.g Theophylline, theobromine, caffeine
- Recently interest has declined in this class of drugs:
- Side effects
- Need for plasma drug levels(toxicity)
- Pharmacokinetics
- Availability of other effective drugs
- Still widely used drugs especially in developing countries due to their lower cost.
■ Adverse effects
- Anorexia, nausea, vomiting, abdominal discomfort
- headache, and anxiety
- Seizures or arrhythmias
- Diuresis
■ Doxylphylline
- long acting, oral
> Corticosteroids in asthma
-
Effective drugs for treatment of asthma.
-
Development of inhaled corticosteroids is a major advance in asthma therapy.
-
Used prophylactically as a controller therapy.
-
Reduce the need for rescue agonist.
-
Benefit starts in 1 week but continues up to several months.
-
If asthma not controlled at low dose of ICS then addition of long acting agonist is more effective than doubling steroid dose.
-
Effects: Broad anti-inflammatory effects: by
-
Marked inhibition of infiltration of airways inflammatory cells.
-
Modulation of cytokine and chemokine production
-
Inhibition of eicosanoid synthesis
-
Decreased vascular permeability.
-
Potentiate effect of agonist.
■ Inhaled corticosteroids (ICS)
✗ Use of Agonists >2 times a week indicates need of a ICS
○ E.g Beclomethasone, Budesonide, Fluticasone
- Adverse effects:
- Oropharyngeal candidiasis, dysphonia
- Decreased bone mineral density.
- Skin thinning, purpura
- Growth retardation in children
change in Voice
only in exacerbation
Systemic(oral/IV) steroids in asthma
Indication
- Acute exacerbation (lung function predicted)
- Chronic severe asthma
- A 5-10 day course of prednisolone 30-45mg/d is used.
- 1% of patients may require regular maintenance therapy.
> Leukotrienes pathway inhibitors
- Inhibition of 5-lipoxygenase, thereby preventing leukotriene synthesis. Zileuton.
- Inhibition of the binding of LTD4 to its receptor on target tissues, thereby preventing its action. E.g. Zafirlukast, montelukast.
- Oral route.
- Adverse effects
- Liver toxicity
- vasculitis with eosinophilia
- They are less effective than ICSs in controlling asthma
- Use in asthma
- Patients unable to manipulate inhaler devices.
- Aspirin induced asthma.
- Mild asthma – alternative to ICS.
- Moderate to severe asthma – may allow reduction of ICS dose
> Cromones
- E.g Cromolyn sodium & nedocromil sodium
- On chronic use (four times daily) reduce the overall level of bronchial reactivity.
- have no effect on airway smooth muscle tone and are ineffective in reversing asthmatic bronchospasm; they are only of value when taken prophylactically.
- Inhalation route
- May act by stabilization of Mast cells with inhibition of mediator release
Uses
- Asthma - Prevention of asthmatic attacks in mild to moderate asthma
Adverse effects
- Well tolerated drugs
- Minor side effects- throat irritation, cough, and mouth dryness, rarely, chest tightness, and wheezing
► Anti-IgE therapy: if fit take it means he has bad disease
-
Omalizumab
-
recombinant humanized monoclonal antibody targeted against IgE.
-
Action:
- IgE bound to omalizumab cannot bind to IgE receptors on mast cells and basophils, thereby preventing the allergic reaction at a very early step in the process.
-
Use in asthma
-
Persons >12 years of age with moderate-to-severe persistent asthma.
-
Omalizumab is not an acute bronchodilator and should not be used as a rescue medication or as a treatment of status asthmaticus. -
Expensive drug
-
Has to be given under direct medical supervision due to the risk of
anaphylaxis
In the Emergency departmentFactors related to poor outcomes
-
Inadequate patient and physician assessment of an acute episode resulting in undertreatment
-
Overuse of prescribed or over-the-counter medications leading to delays in seeking treatment
-
Failure of physicians to consider previous ED visits, hospitalizations, or life-threatening episodes of asthma
-
Failure to initiate corticosteroid therapy early during an exacerbation.
ACUTE exacerbations of asthma classified by severity
Mild, moderate or severe (Status asthmaticus)
- Reflected by the degree of airway obstructions and acute response to bronchodilators
- Also assessed by degree of physiological response and hemodynamic compromise
Table 73-1 Objective Findings in Asthma Assessment Y
| FACTOR | SEVERE ASTHMA ( L) |
|---|---|
| Pulse rate (beats/min) | but may be less with equally severe asthma |
| Respiratory rate (breaths/min) | but most are , therefore nondiscriminating |
| Pulsus paradoxus (mm Hg) | but may be absent with equally severe asthma in 50% of cases |
| Pulse rate , respiratory rate , pulsus paradoxus | If all three abnormal, 90% with severe asthma, but only 40% with L have all three abnormal |
| Use of accessory muscles of respiration | If present, may indicate severe asthma; if absent, may have equally severe asthma in 50% of cases |
| ABG analysis (mm Hg) | or indicates severe asthma; all other values difficult to interpret unless or known |
| Pulmonary function studies | and measure directly the degree of airflow obstruction; most useful in assessing severity and guiding treatment decisions |
ABG, arterial blood gas; , forced expiratory volume in 1 second; , partial pressure of carbon dioxide in arterial blood; , partial pressure of oxygen in arterial blood; , peak expiratory flow rate.
Box 73-2 The Differential Diagnosis of Asthma z
- Cardiac conditions
- Valvular heart disease
- Congestive heart failure in old age
- COPD exacerbation
- Pulmonary infection
- Pneumonia
- Allergic bronchopulmonary aspergillosis
- Löffler’s syndrome
- Chronic eosinophilic pneumonia
- Upper airway obstruction
- Laryngeal edema
- Laryngeal neoplasm
- Foreign body
- Vocal cord dysfunction
- Endobronchial disease
- Neoplasm
- Foreign body
- Bronchial stenosis
- Pulmonary embolus
- Carcinoid tumor
- Allergic or anaphylactic reaction in children
- Miscellaneous conditions
- GERD
- Noncardiogenic pulmonary edema
- Addison’s disease
- Invasive worm infection
not all wheeze
mean asthma
COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease.
Trx algorithm
| MILD TO MODERATE | SEVERE | |
|---|---|---|
| FEV 1 or PEFR (% predicted/personal best) | ≥40% | Unable or <40% |
| Oxygen therapy | Maintain SaO 2 ≥90% | Maintain SaO 2 ≥90% |
| Nebulized albuterol solution | ||
| Levalbuterol (optimal) | 1.25 mg q20min for up to three doses | 1.25 mg q20min for three doses |
| Racemic albuterol | 2.5 mg q20min for up to three doses | Continuous for 1 hr if severe 5.0 mg q20min for three doses Continuous for 1 hr if severe |
| Albuterol MDI with VHC | ||
| Levalbuterol (45 µg/puff) (optimal) | 6-12 puffs q20min for up to three doses WS | Same for three doses (if able to do), WS |
| Racemic albuterol (90 µg/puff) | 6-12 puffs q20min for up to three doses WS | Same for three doses (if able to do), WS |
| Ipratropium therapy | ||
| Nebulized solution | If previous response (same dose as for severe) | 0.5 mg q20min for three doses (may mix with albuterol solution) |
| MDI (18 µg/puff) with VHC | If previous response (same dose as for severe) | 8 puffs q20min for three doses |
| Systemic corticosteroids | ||
| Oral (preferred) | 40-80 mg of prednisone or prednisolone per day if no immediate response to albuterol | 40-80 mg of prednisone or prednisolone per day |
| Intravenous (unable to take orally or absorb) | 40-80 mg of methylprednisolone per day | 40-80 mg of methylprednisolone per day |
| Intravenous magnesium sulfate | Not indicated | 2-3 g over 20 min (or at rates of up to 1 g/min) if FEV 1 ≤ 25% predicted |
FEV1, forced expiratory volume in 1 second; MDI, metered-dose inhaler; PEFR, peak expiratory flow rate; SaO2, oxygen saturation in arterial blood; VHC, valved holding chamber; WS, with supervision.
Pearls
- Most patients suffering asthma are poorly controlled
- If B agonists are used more than twice a week, then controlling therapy should be initiated
- Long-acting B agonists should not be used in isolation to treat asthma
- Magnesium plays a therapeutic role in moderate to severe asthma
Doesn’t work in asthma nowadays
- * give IV B agonist in severe asthma - we may use ephedrine
(when contraindicated put Pit in BIPAP)