Chest and CVS Trauma
Dr. Abdulaziz Alrabiah
Objectives
- Different life-threatening injuries
- Assessment
- Management
Tension Pneumothorax
“It will kill the patient”
- Air between visceral and parietal pleura.
- One-way valve → allows air to go inside the pleural space but not out.
- It is a clinical diagnosis, do not wait for chest X-ray.
Presentation
- Distended neck veins
- Tracheal deviation to the opposite side
- Hypotension / evidence of hypoperfusion (e.g., decreased LOC, tachycardia)
- Absent breath sounds on the ipsilateral side
Treatment
- High flow O2 (15 L)
- Needle decompression (14G): 5th intercostal space
- Intercostal chest drain: 5th intercostal space, between mid and anterior axillary lines
Chest X-ray
Warning: Not for diagnostic use in Tension Pneumothorax (Clinical diagnosis).
Clinical Diagnosis Triad:
- Hypotension
- Shortness of Breath
- Tracheal deviation
 0845HRS | L | PORTABLE | AP | Air | Lung
0845HRS | L | PORTABLE | AP | Air | Lung
Pneumothorax
“Will not kill the patient” (Normal Blood Pressure)
- Air in the pleural space.
Signs
- ✓ Decreased breath sounds
- ✓ Hyper-resonant on percussion
- ✗ No signs of tension if no tracheal deviation, normal BP
Management
Treatment is decided according to the size of the pneumothorax.
Sizing (Collins Method estimate):
- Horizontal line from 3rd rib.
- Formula:
(Apical line + Middle line + Lower line) / 3 - Each 1 cm roughly corresponds to 10%.
Treatment Protocol: If BP and Pulse are good:
- < 20%: High flow O2, repeat X-ray after 4 hours.
- If improved: No need for chest tube.
- If worse: Needs chest drain.
- > 20%: Put chest drain.
Open Pneumothorax

Definition & Signs
- Penetrating chest trauma.
- Communication between pleural space and outside environment (i.e., sucking chest wound).
- May be associated with hemothorax.
- Clinical signs:
- Visible wound
- Plus tension pneumothorax features
Treatment
- High flow O2 (15 L)
- 3-way dressing: Allows air to escape but prevents air from entering the pleura.
- Chest drain: Insert away from the wound (usually one space up).
3-Way Dressing & Chest Tube

 Chest X-ray consistent with Pleural Effusion (PE) or Hemothorax.
Chest X-ray consistent with Pleural Effusion (PE) or Hemothorax.
Massive Hemothorax
Definition
- > 1500 ml of blood immediately after chest drain placement.
- > 200 ml/hr of blood drained for 4 hours.
- Note: Do not rely on color. On Chest X-ray: > 2/3 of the available space in the hemithorax.
Causes
- Lung parenchymal injury
- Intercostal artery injury
- Internal mammary artery injury
Clinical Signs
- Decreased breath sounds on the affected side
- Dullness on percussion on the affected side
chest X-ray
Treatment
- High flow O2 (15 L)
- Chest drain
- Operative Thoracotomy indicated if:
- Drained > 1500 ml of blood immediately ⇒ operative thoractomy
- Drained > 200 ml/hr for 4 hours ⇒ operative thoractomy
Pulmonary Contusion
“Bruising with no bleeding”
Overview
- Suspect in any significant thoracic trauma.
- May occur in small children in the absence of fractures due to high compliance of the chest wall.
- Signs: Respiratory distress, hemoptysis, cyanosis.
- Exam: Decreased breath sounds and crackles in the affected lung area.
- Labs: Hypoxia and/or hypercapnia on ABG.
- Diagnosis:
- Detectable on bedside ultrasound.
- Alveolar opacities on CXR.
Management
- High flow O2 (15 L/min).
- Analgesia for pain.
- Respiratory support: Severe cases require intubation and mechanical ventilation.
- Fluid restriction: May reduce size of contusion but might not affect outcomes (controversial).
 Chest X-ray: “fluid but not in Pleura, in lung itself”.
Chest X-ray: “fluid but not in Pleura, in lung itself”.
Pneumomediastinum
- It is a sign of other serious injuries: Larynx, trachea, major bronchi, pharynx, esophagus.
- Causes: Foreign Body (FB) aspiration, perforation of esophagus/trachea.
Signs
- Subcutaneous emphysema: Crepitus when touching the skin.
- Hamman’s sign: Crunching sound over the heart.
Treatment
- Treat the underlying cause (trachea, esophagus, etc.).
Cardiac Tamponade
Fluid in pericardial space
- More common in penetrating thoracic trauma than blunt trauma.
- 50-75 ml of blood in pericardial sac may result in tamponade.
Clinical Features
- Anxiety and agitation.
- Obstructive shock: Tachycardia, hypotension, cool peripheries.
- Beck’s Triad: Z
- Muffled heart sounds
- Hypotension
- Distended neck veins
- Pulsus paradoxus: Drop in systolic blood pressure > 10 mmHg on inspiration. Z
Diagnosis
- Mostly diagnosed following identification of a pericardial effusion on FAST exam.
- Clinical diagnosis.
Management
- High flow oxygen (15 L/min via non-rebreather).
- May transiently respond to fluid challenge.
- Needle pericardiocentesis: Preferably ultrasound-guided (may be lifesaving).
- Thoracotomy: If patient arrests.
- Pericardiotomy: Definitive treatment.
 Ultrasound image showing pericardial effusion. only tempound - its clinically
Ultrasound image showing pericardial effusion. only tempound - its clinically
 Technique for needle pericardiocentesis (A: Xiphoid process).
Technique for needle pericardiocentesis (A: Xiphoid process).
Aortic Dissection
Blood entering the medial layer of the wall with the creation of a false lumen, caused by a tear.
Classification
| Percentage | 60% | 10–15% | 25–30% |
|---|---|---|---|
| Type | DeBakey I | DeBakey II | DeBakey III |
| Stanford | Type A (Proximal) | Type A (Proximal) | Type B (Distal) |
| Note | Involves Ascending + Descending | Ascending only | Descending only |
| Management | Surgery | Surgery | Medical (Beta Blockers, Control BP) |
Clinical Features
- Chest pain: Tearing sensation.
- Radiation: Radiates to back between shoulder blades.
- History of:
- HTN
- Aortic regurgitation
- Ischaemic heart disease
- Syncope, Seizure
- Flank pain
Risk Factors: Y
- Marfan’s syndrome, Ehlers-Danlos syndrome, Turner syndrome
- HTN
- Syphilis
- arteritis??????Arthritis
- Cocaine abuse
- Iatrogenic
Clinical Exam Y
- BP: Check BP in the arm with the best radial pulse (look for asymmetrical pulses: carotid, brachial, femoral).
- Aortic Regurgitation is common.
- Shock: Ominous signs (tamponade, hypovolemia, vagal tone).
- Heart Failure.
- Neurological deficits: Limb weakness, paraesthesiae, Horner’s syndrome.
- SVC syndrome: Compression of SVC by aorta.
- Haemothorax.
Complications Y
- Aortic rupture
- Aortic Regurgitation (AR)
- Acute Myocardial Infarction (AMI)
- Tamponade
- End-organ ischaemia (brain, limbs, spine, renal, gut, liver)
- Death
Investigations
1. Chest X-ray
Note: Normal in 11-16% of cases. Not sensitive.
- Widened mediastinum (> 8 cm) (56-63%)
- Abnormal aortic contour (48%)
- Aortic knuckle double calcium sign (> 5 mm) (14%)
- Pleural effusion (Left > Right, obliterated angle)
- Tracheal shift
- Left apical cap
- Deviated NGT
 Chest X-ray showing findings of aortic dissection: shifted trachea, calcium sign, widened mediastinum, hemothorax, effusion, left apical cap.
Chest X-ray showing findings of aortic dissection: shifted trachea, calcium sign, widened mediastinum, hemothorax, effusion, left apical cap.
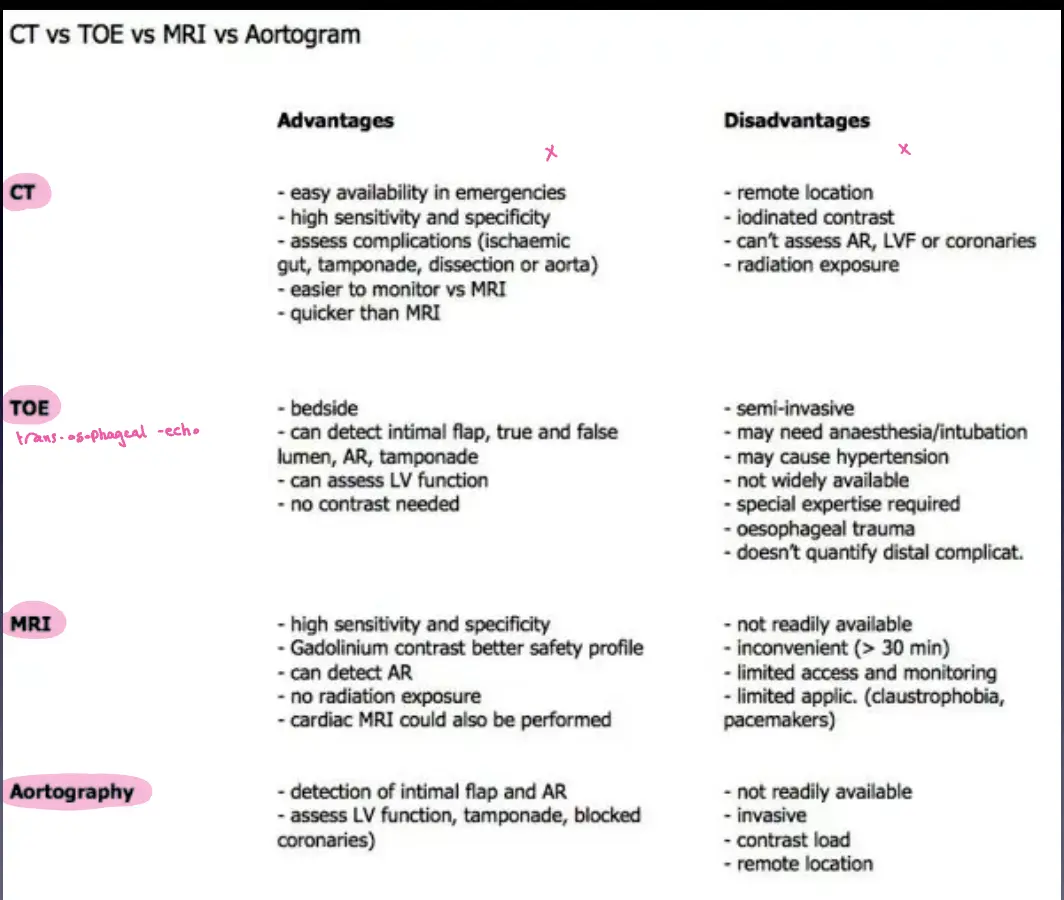
2. Imaging Comparison
| Modality | Advantages | Disadvantages | Notes |
|---|---|---|---|
| CT | • Bedside • Detects intimal flap, true/false lumen, AR, tamponade • Assess LV function • Quick | • Iodinated contrast • Radiation exposure • Can’t assess coronaries well | Semi-invasive. |
| TOE (Transesophageal Echo) | • High sensitivity/specificity • Safe contrast (Gadolinium) • Detects AR • No radiation | • Not readily available • Inconvenient (>30 min) • Limited access/monitoring | |
| MRI | • Detects intimal flap & AR • Assess LV function, tamponade, blocked coronaries | • Not readily available • Invasive (contrast) • Long duration | Remote location. |
| Aortography | Gold Standard | ||
 |
Treatment
- Medical Management:
- Control BP (Labetalol, GTN).
- Aim for SBP 100-120 mmHg and Pulse 60-80/min.
- Fluid and blood resuscitation.
- Call Cardiothoracic Surgeon.
- Indications for Surgery:
- Persistent pain
- Type A Dissection
- Branch Occlusion
- Leak
- Continued extension despite optimal medical management