Chest Pain
Bader Alyahya
Objectives
- Overview of chest pain
- Differential diagnosis of chest pain
- Typical vs. atypical chest pain
- Evaluation of chest pain
- Review patient cases
Overview
- Chest pain accounts for 6 million annual visits to EDs in the United States.
- It is the second most common ED complaint.
- Patients present with a wide spectrum of signs and symptoms.
- The clinician’s priority is to recognize life-threatening causes.
Life-Threatening Differential Diagnosis (The “Big 5”)
- ACS (Acute Coronary Syndrome) - Give “Jive Xhong” [sic] & aspirin to decrease morbidity.
- PE (Pulmonary Embolism)
- Aortic Dissection
- Tension Pneumothorax
- Pericarditis (Note: listed in intro, also consider Tamponade)
- Esophageal Rupture (Mediastinitis)
Initial Approach
- ABC’s first: Always look for conditions requiring immediate intervention; assess appearance and vital signs.
- Aspirin: Administer for potential ACS.
- EKG: Obtain within 10 minutes.
- Monitoring: Continuous cardiac and vital sign monitoring.
- Pain Relief: Provide appropriate analgesia.
- History & Physical: Guided by the wide differential diagnosis.
- Logical/Physical Exam Notes: “Hishog” [sic]
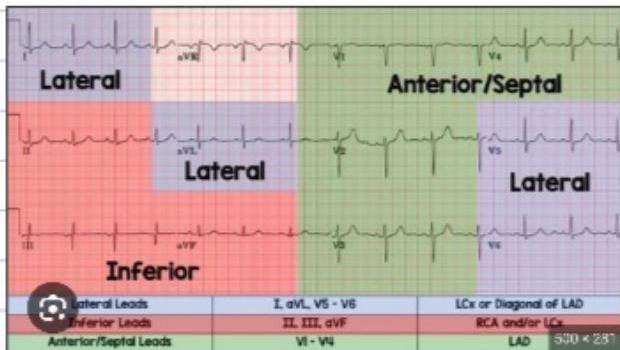
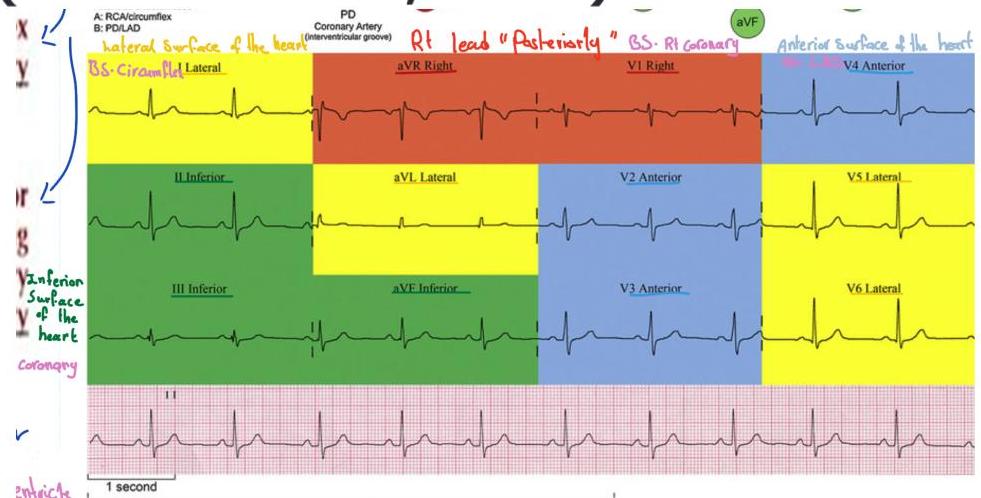
ECG Interpretation & MI Localization
| Territory | Leads |
|---|---|
| Inferior | II, III, aVF |
| Anteroseptal | V₁, V₂, V₃, V₄ |
| Anterolateral | V₁, V₂, V₃, V₄, V₅, V₆ |
| Extensive Anterolateral | V₁-V₆, I, aVL |
| Lateral | V₅, V₆ |
| High Lateral | I, aVL |
| Inferolateral | (7) V₂, V₃, V₅, V₆, I, aVL |
ECG Notes:
ECG Interpretation Notes
Posterior MI
- Detection: Not shown on a standard 12-lead ECG.
- Clinical Suspicion: Suspect when there is Typical Chest Pain with ST depression in V₁, V₂, V₃ and prominent R-waves (these are reciprocal changes).
- Extended ECG: Place leads posteriorly to confirm:
- V₇: Posterior axillary line (same level as V₆).
- V₈: Tip of the scapula (mid-scapular line).
- V₉: Left paraspinal region (between scapula and spine).
Right Ventricular (RV) Infarct
-
Association: Suspect in all Inferior MIs (occurs in ~20% of cases).
-
Diagnostic Move: Move lead V₄ to the right side (V₄R).
-
Treatment Protocol:
- Give Fluids: Preload dependent.
- DO NOT Give Nitroglycerin: This may precipitate cardiac arrest due to a critical decrease in preload.
-
Prognosis: If an acute inferior MI is present, checking for RV involvement is crucial as mortality is higher if both are present.
Cardiogenic Shock & Hypotension
- Assessment: If the patient is hypotensive, check lung sounds:
- Lungs Clear: Likely RV Infarct → Treat with Fluids.
- Rales/Congestion Present: Likely extensive Anterior MI (Pump failure) → Treat with Inotropes.
Reciprocal Changes
- Definition: Mirror images of ST elevation (finding these increases the sensitivity/specificity for diagnosing an MI).
- Patterns:
- Posterior Anterior (Septal leads V₁-V₃): ST depression in V₁-V₃ is reciprocal to posterior elevation.
- Anterior Inferior: LAD occlusion may show reciprocal changes in II, III, aVF.
- Inferior Lateral (High Lateral): Inferior elevation often shows depression in aVL (and vice versa).
- Lateral Inferior: (Removed “Septal” as it is less standard).
High Lateral MI
- Unique Feature: Often described as the only MI pattern that may not strictly follow the “consecutive leads” rule in early presentation.
- Criteria: Isolated ST elevation in aVL is a subtle but high-risk sign.
- Key confirmation: Look for reciprocal ST depression in Lead III.
- If you see elevation in aVL + depression in III, treat as High Lateral MI until proven otherwise.
Clinical Presentation
History (OPQRST)
- O - Onset
- P - Provocation / Palliation
- Q - Quality / Quantity
- R - Region / Radiation
- S - Severity / Scale
- T - Timing / Time of onset
Physical Exam
- General Appearance and Vitals: “Sick vs. Not Sick.”
- Chest Exam:
- Inspection: Scars, heaves, tachypnea, work of breathing.
- Auscultation: Murmurs, rubs, gallops, breath sounds.
- Percussion: Dullness.
- Palpation: Tenderness, PMI.
- Key Finding: Reproducible chest pain “points toward a musculoskeletal” cause.
Differential Diagnosis
Life-Threatening Causes
- Acute Coronary Syndrome (Unstable Angina, NSTEMI, STEMI)
- STEMI: ST elevation in 2 continuous leads.
- NSTEMI: Aspirin; pain management; Cath within 2nd day.
- Unstable Angina: Emergency Cath if pain is ongoing.
- Note: NSTEMI with -ve troponin → becomes +ve troponin.
- Aortic Dissection
- Pulmonary Embolism
- Tension Pneumothorax
- Pericardial Tamponade
- Mediastinitis (e.g. esophageal rupture)
- Pericarditis: Previous URI infection; pain changes with position of the patient.
Comprehensive Differential (UpToDate 2012)
| Category | Conditions |
|---|---|
| Non-ischemic Cardiovascular | Aortic dissection, Myocarditis, Pericarditis |
| Pulmonary | Pleuritis, Pneumonia, Pulmonary embolus, Tension pneumothorax |
| Psychiatric | Affective disorders (depression), Anxiety, Hyperventilation, Panic disorder, Somatiform, Thought disorders |
| Gastrointestinal | Biliary (Cholangitis, Cholecystitis, Colic), Esophageal (Spasm, Reflux, Rupture), Pancreatitis, PUD (Perforating vs Nonperforating) |
| Chest Wall | Cervical disc disease, Costochondritis, Fibrositis, Herpes zoster (pre-rash), Neuropathic pain, Rib fracture, Sternoclavicular arthritis |
Typical vs. Atypical Chest Pain
Typical Cardiac Pain
- Described as discomfort/pressure rather than “pain.”
- Duration > 2 minutes.
- Provoked by activity/exercise.
- Radiation (i.e. arms, jaw).
- Does not change with respiration or position.
- Associated with diaphoresis/nausea.
- Relieved by rest or nitroglycerin.
Atypical (Unlikely Cardiac) Pain
- Pain localized with one finger.
- Constant pain lasting for days.
- Fleeting pains (seconds).
- Pain reproduced by movement or palpation.
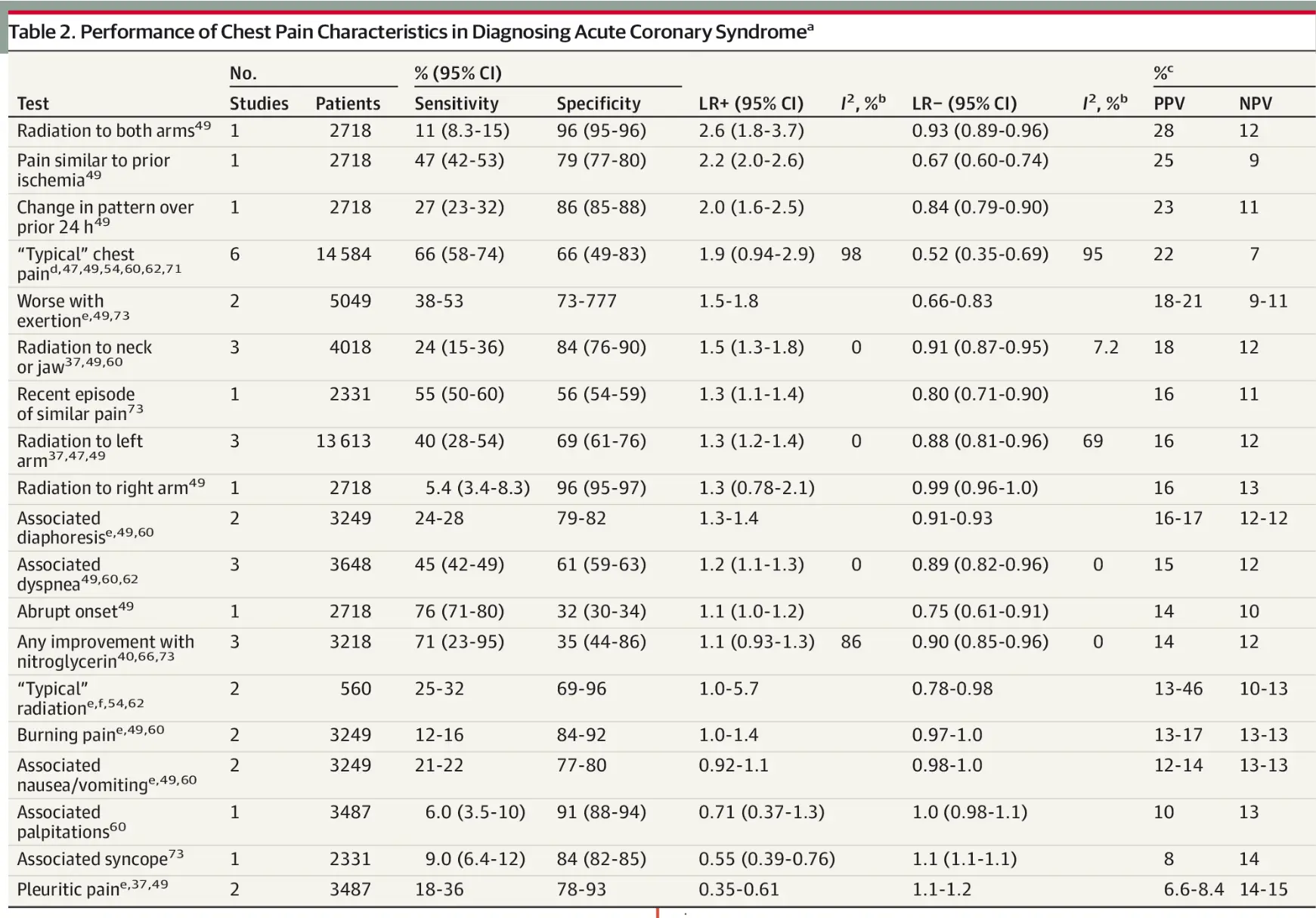
The Rational Clinical Examination Systematic Review
- Key Effect: Perform ECG every 10-20 min (4 times total). If normal, it will not change after that.
- Source: JAMA. 2015;314(18):1955-1965.
Table 2: Performance of Chest Pain Characteristics (ACS)
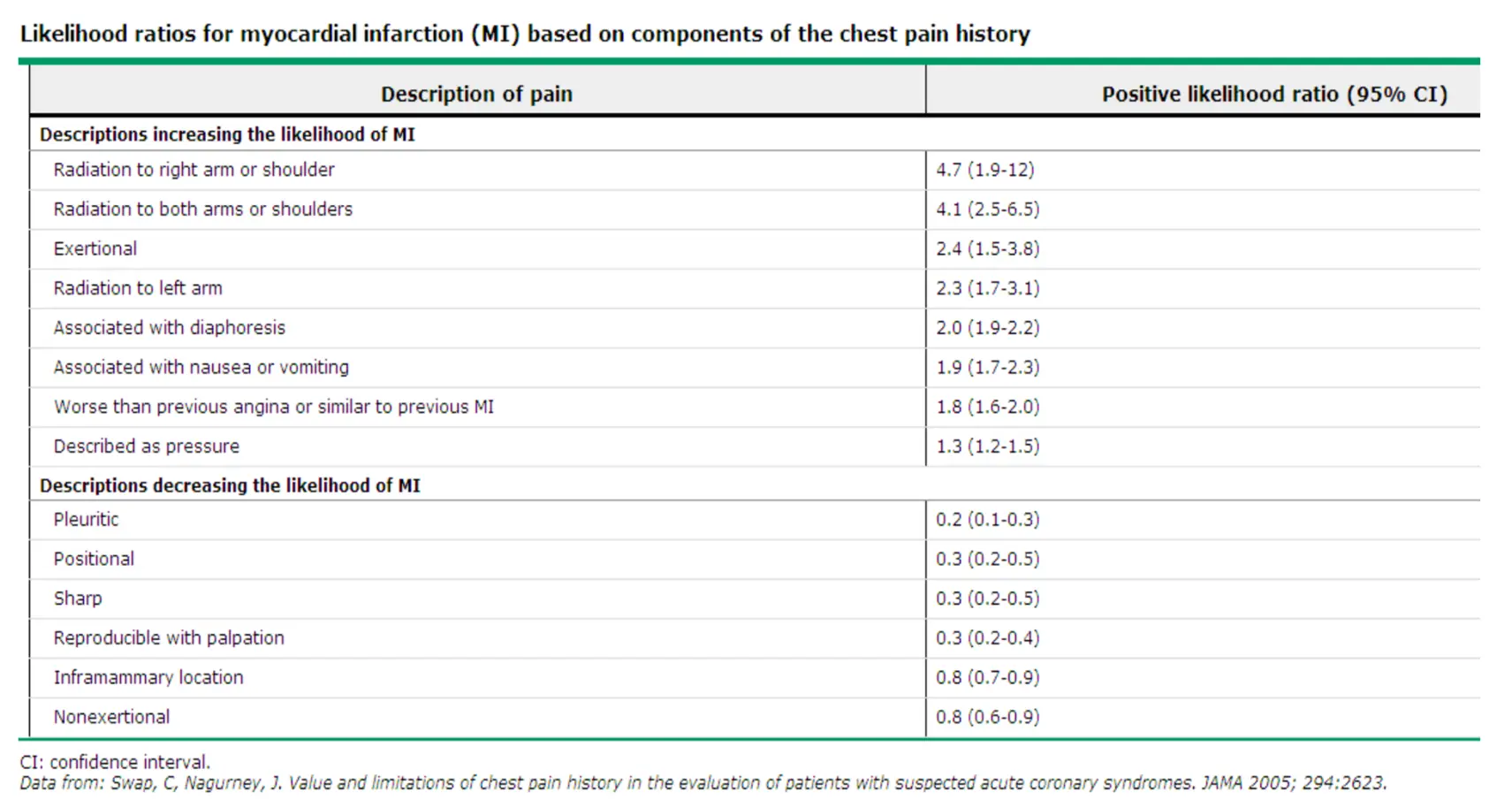
Likelihood Ratios (MI) Summary (UpToDate 2012)
Evaluation & Management Workflow
Scenario 1: The Intern’s Call
- Setting: 2:00 AM. Mr. S, 67M with CAD and AKI, has chest pain after walking from the bathroom.
- Immediate Action:
- Ask nurse for current vital signs.
- Request an EKG and admission EKG for comparison.
- Go see the patient!
- Assessment:
- Determine stability.
- Interpret EKG vs. baseline.
- If unstable or concerning EKG, call senior resident.
- Stable Patient Protocol:
- Focused History (CAD risk, typical/atypical, prior MI similarity).
- Focused Physical:
- Vitals (Tachycardia, BP shifts, Hypoxia).
- HEENT (JVD, carotid bruits).
- Chest (Rales, wheezes).
- CVS (Murmurs, reproducible pain, S3 gallop).
- Abd (Tenderness, pulsatile mass).
- Ext/Skin (Edema, pulses, rash).
- Diagnostics/Disposition:
- CXR, Cardiac biomarkers, ABG?
- Telemetry/ICU.
- Write a clinical event note!
Supplemental Clinical Findings
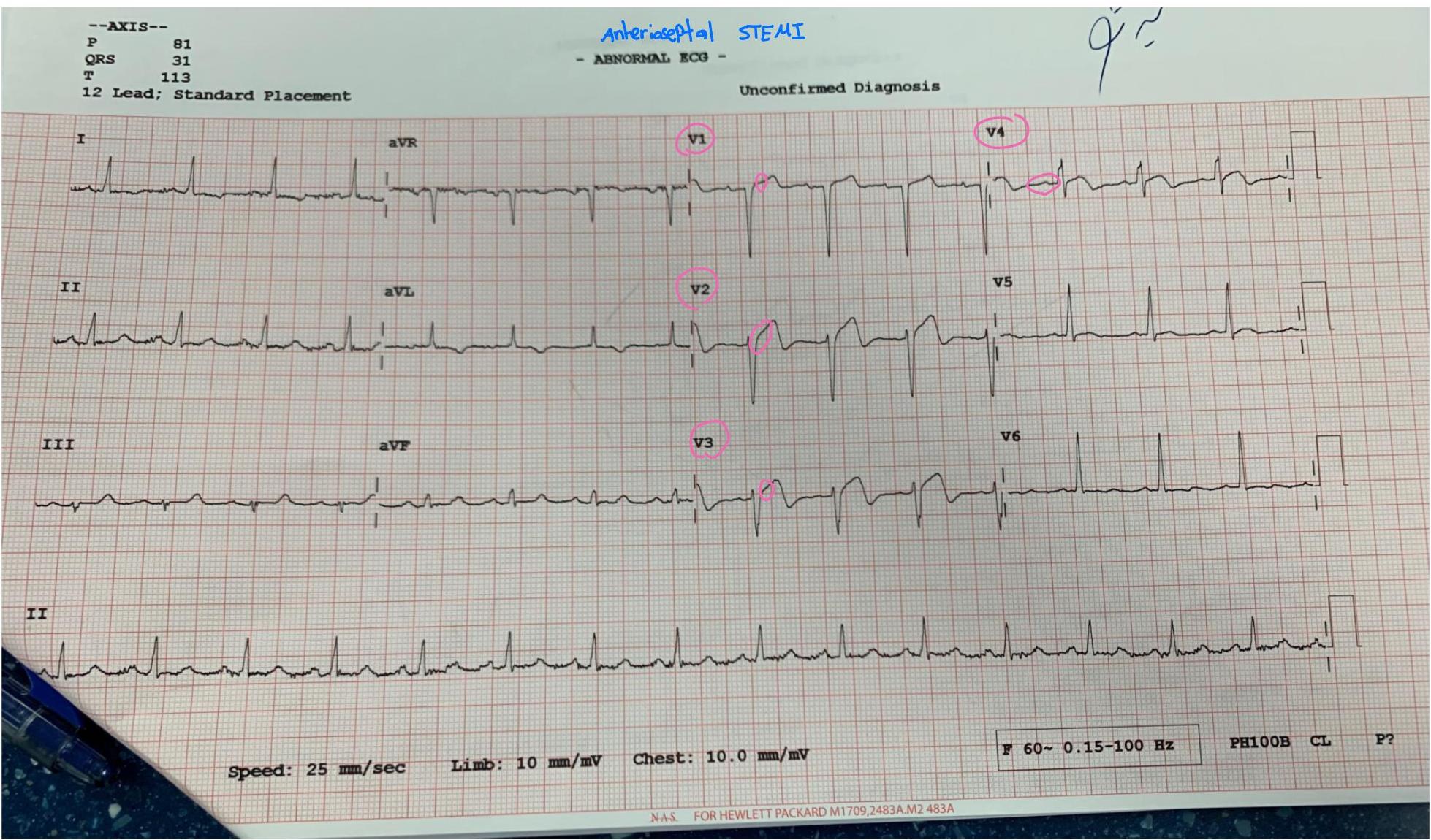
Case Note: 60M with CP 2 days ago (No active pain)
- ECG Findings: Axis (P 81, QRS 31, T 113). Anteroseptal STEMI (unconfirmed).
Case Note: 70M with radiation to both shoulders
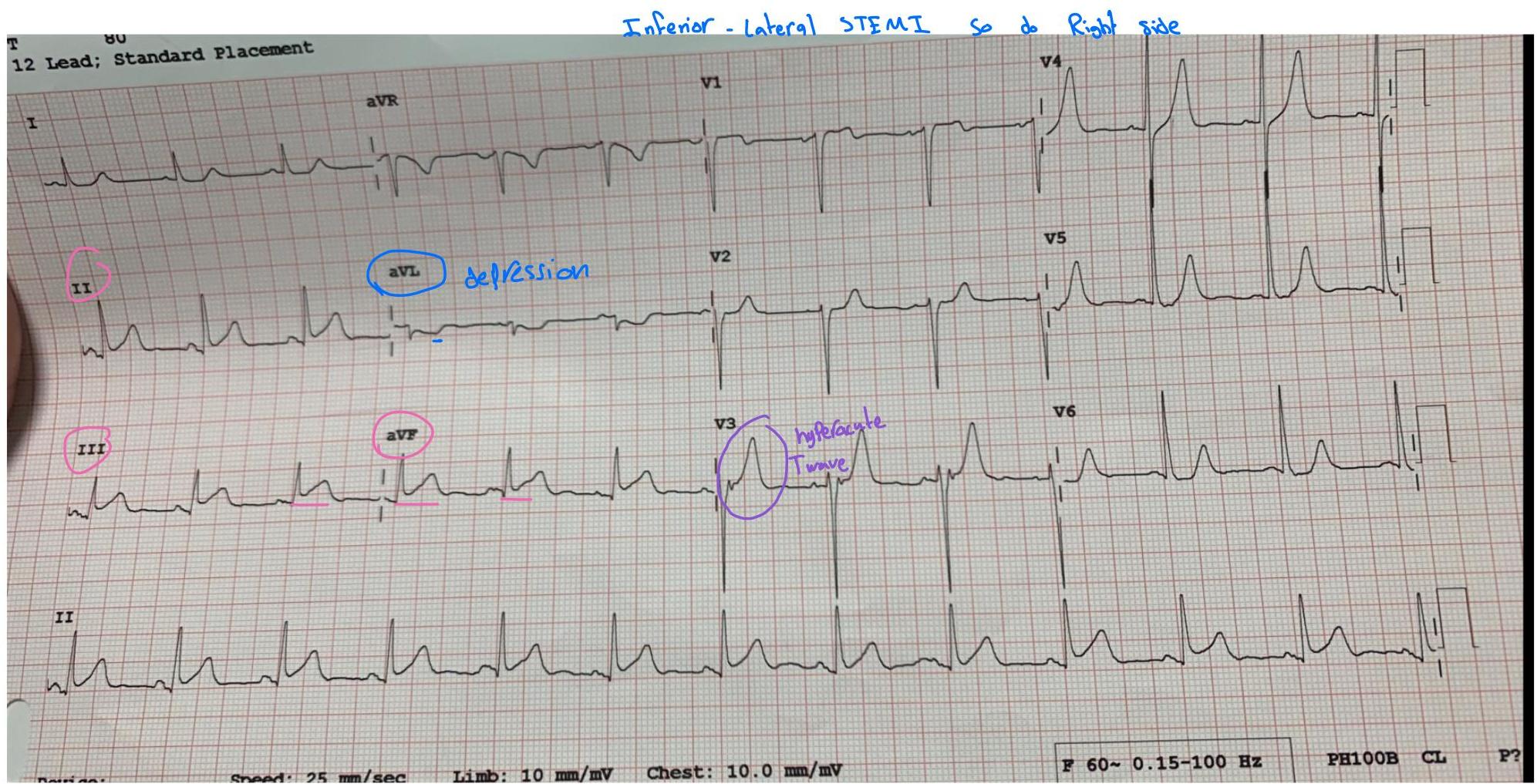
Clinical Pearl: Inferior or Posterior MI
- Next Step: Check Right Ventricular involvement.
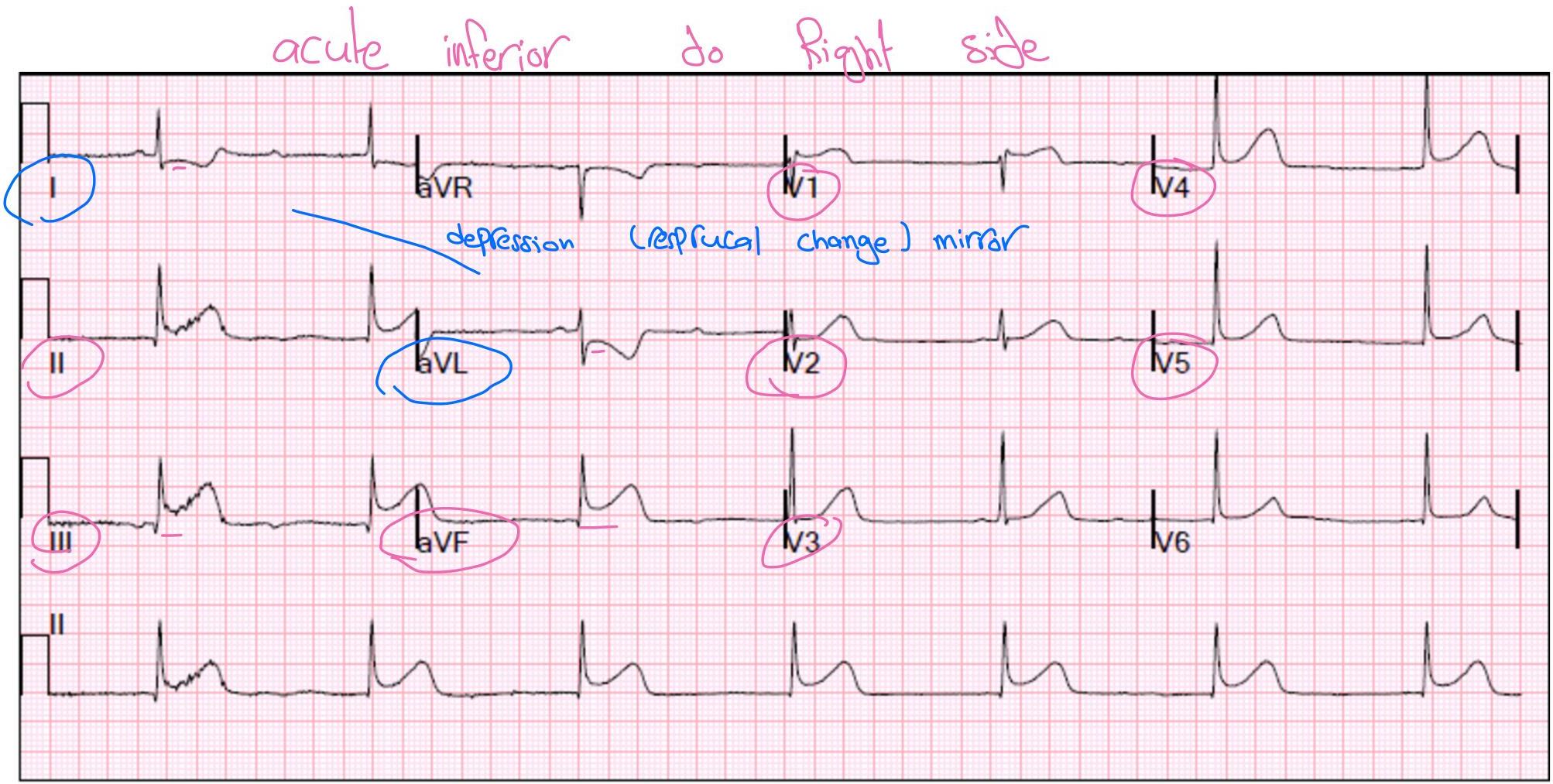
Clinical Pearl: Posterior MI
- Usually not isolated.
- Perform extended ECG (2 leads): one below scapula, one between scapula and vertebra.
- 20% have RV involvement or fracture leading to hypotension → Treat with fluids.
Clinical Cases
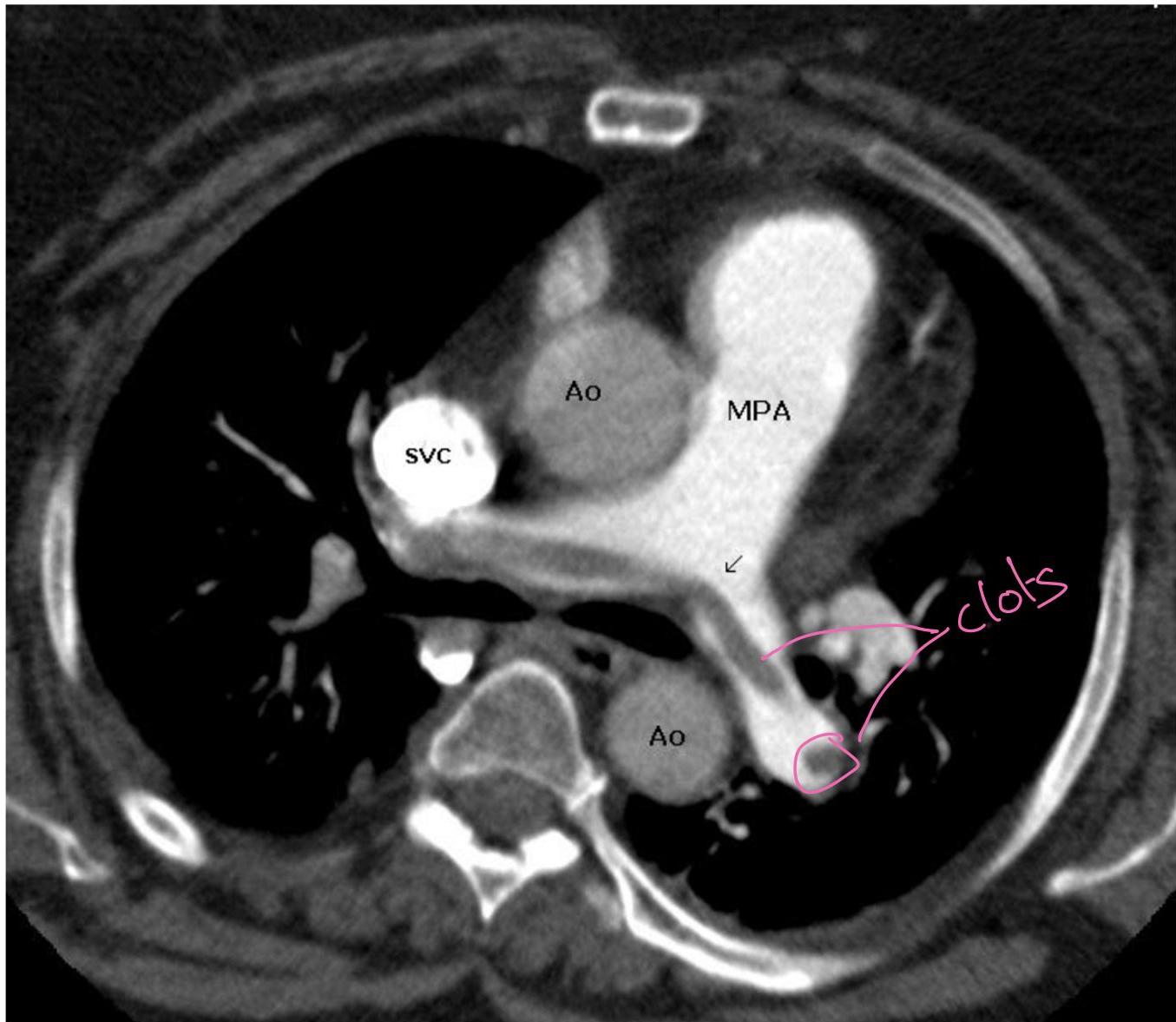
Case 1: Pulmonary Embolism (PE)
- Presentation: 62F, 3 weeks post-right THA, admitted for COPD exacerbation. Sudden onset L-sided chest pain (8/10), pleuritic, O2 sat drop (94% → 88% on 2L NC).
- Initial management: Give aspirin. Repeat ECG 4 times if no change (unstable vs non-STEMI).
- Vitals: Afebrile, HR 120, BP 110/70, RR 28.
- Exam: Accessory muscle use, EAE, loud S2.
- Labs: Positive D-dimer, Troponin 0.12 (Normal < 0.04), BNP 520.
- Clinical Notes: “Plastic chest Pain” [sic]. “To send to CT, increase the sum Five five.”
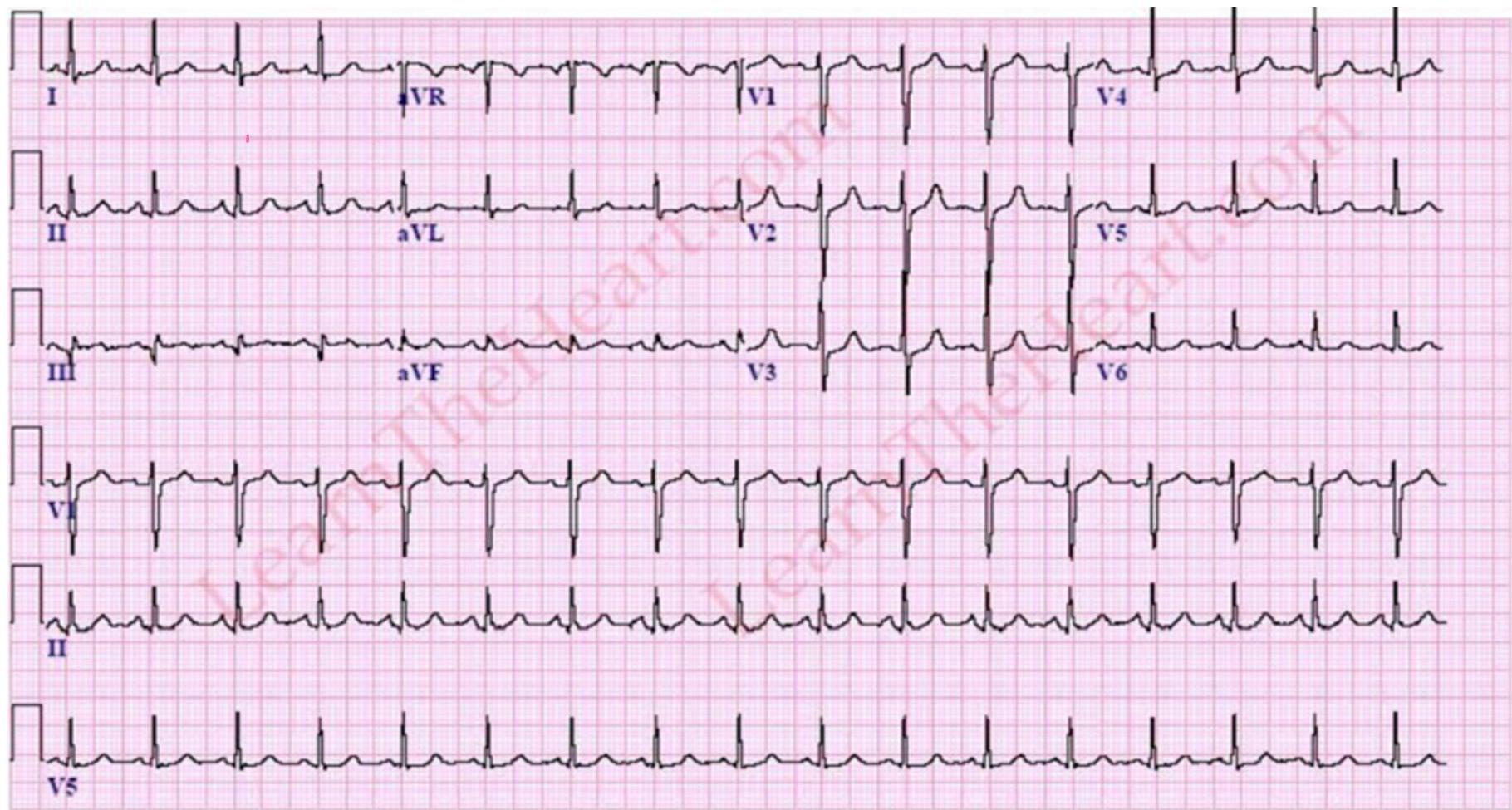
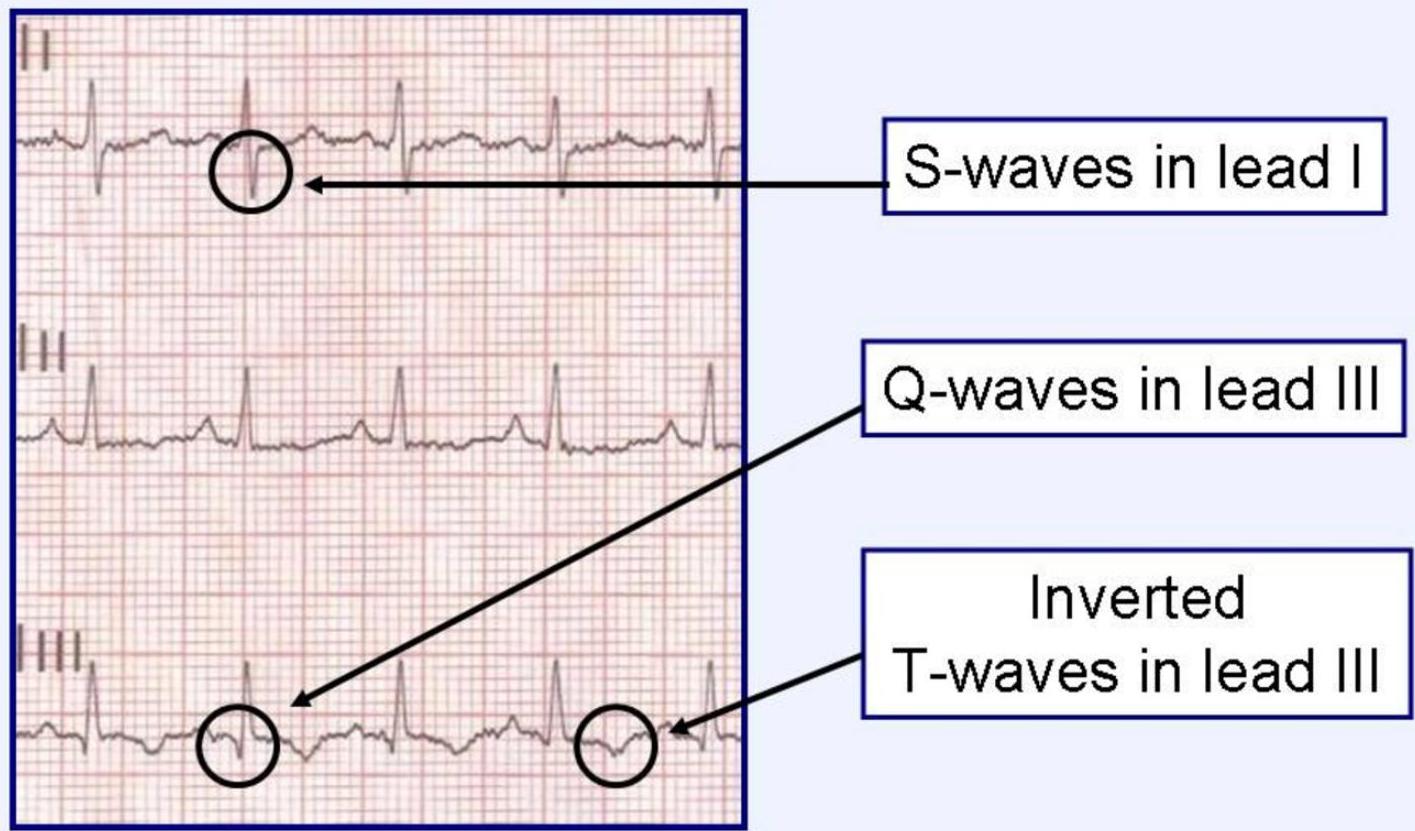
PE
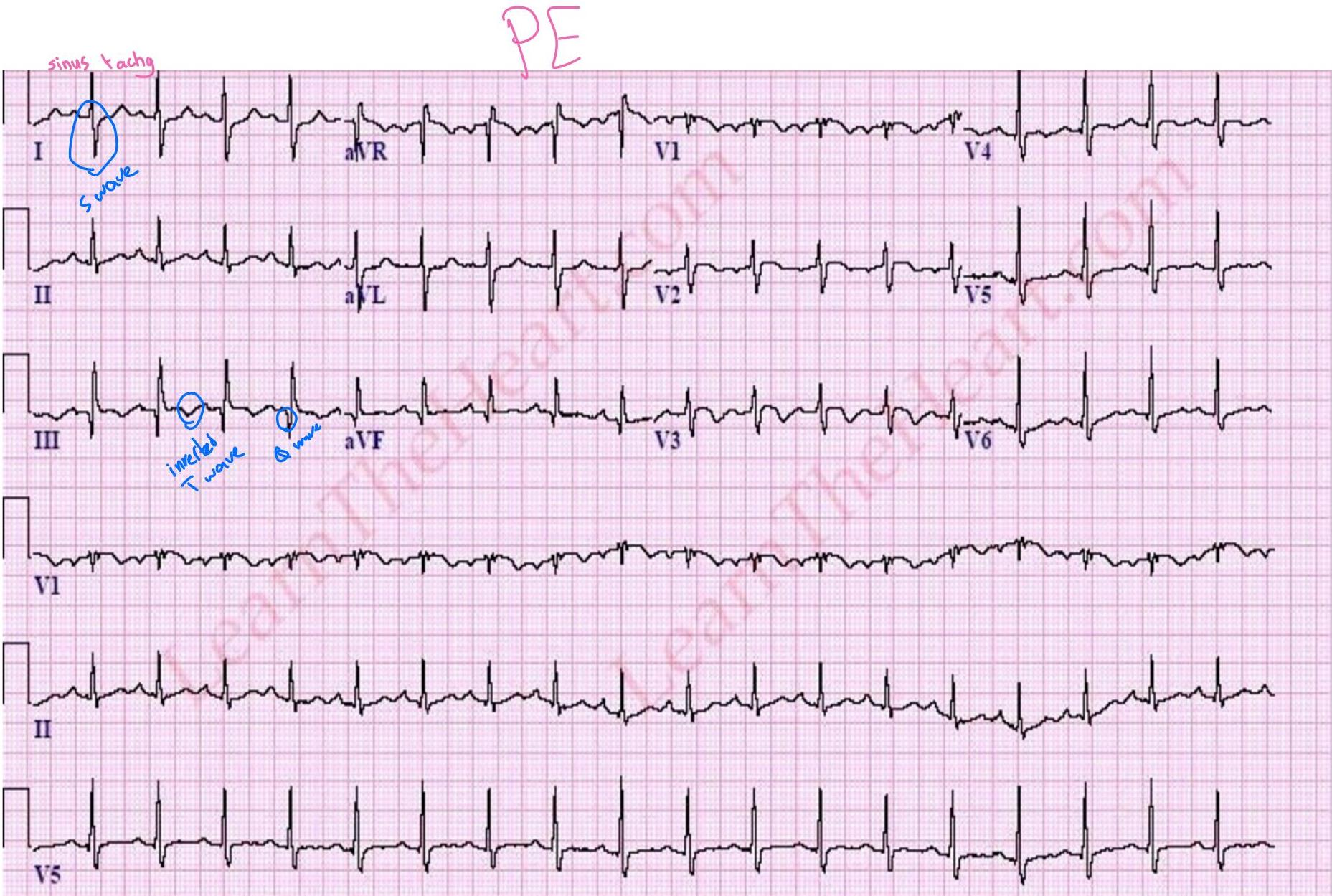
- S1Q3T3: Present in only 20% of PE.

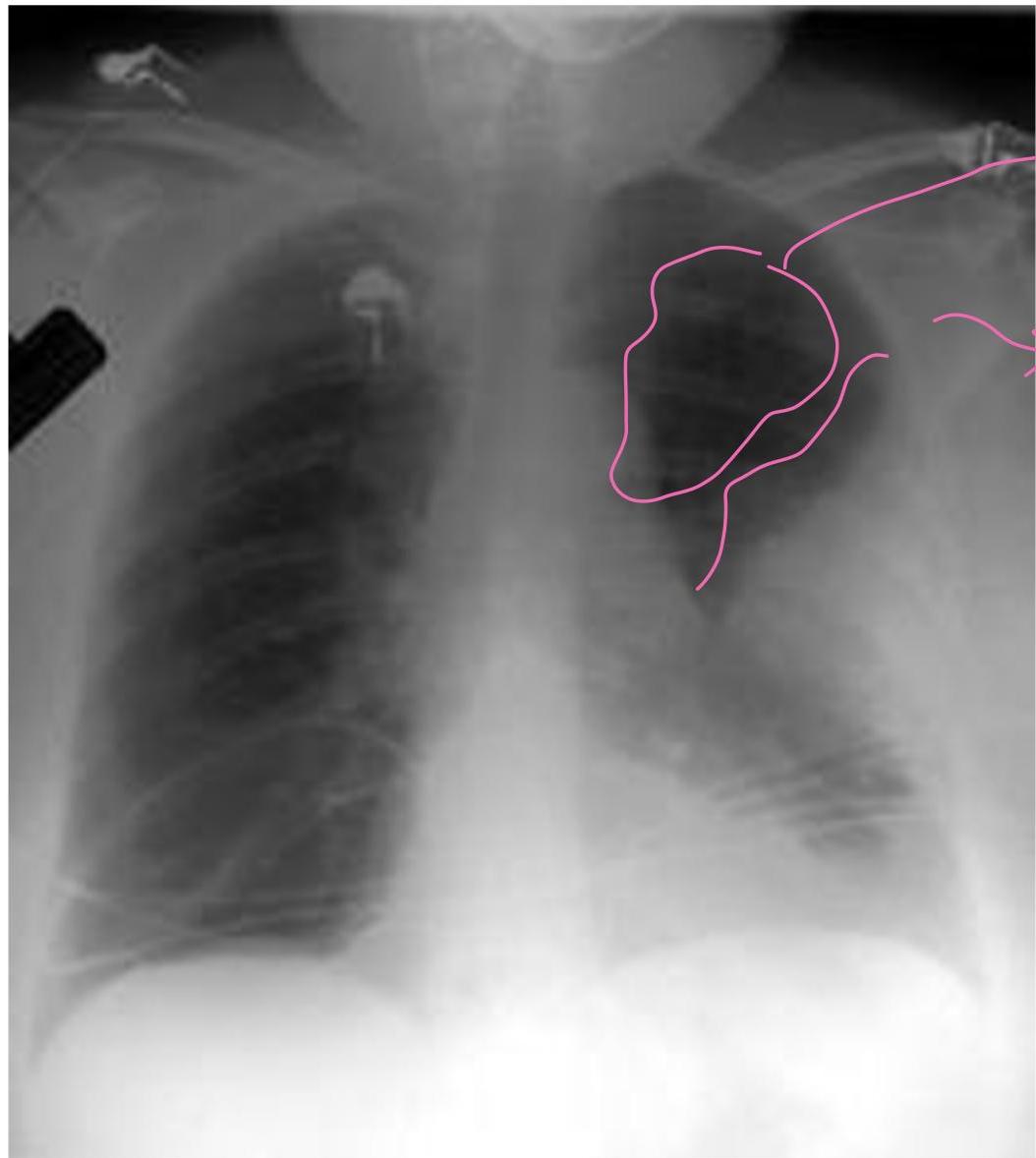
- CXR Findings:
- Westermark sign: Clarified area (hyperlucency) secondary to oligemia.
- Hampton sign: “Dome stuffed” (hump).

- Management Plan: Give heparin (“heforin” [sic]) and send to CT.
Wells Score & PE Management
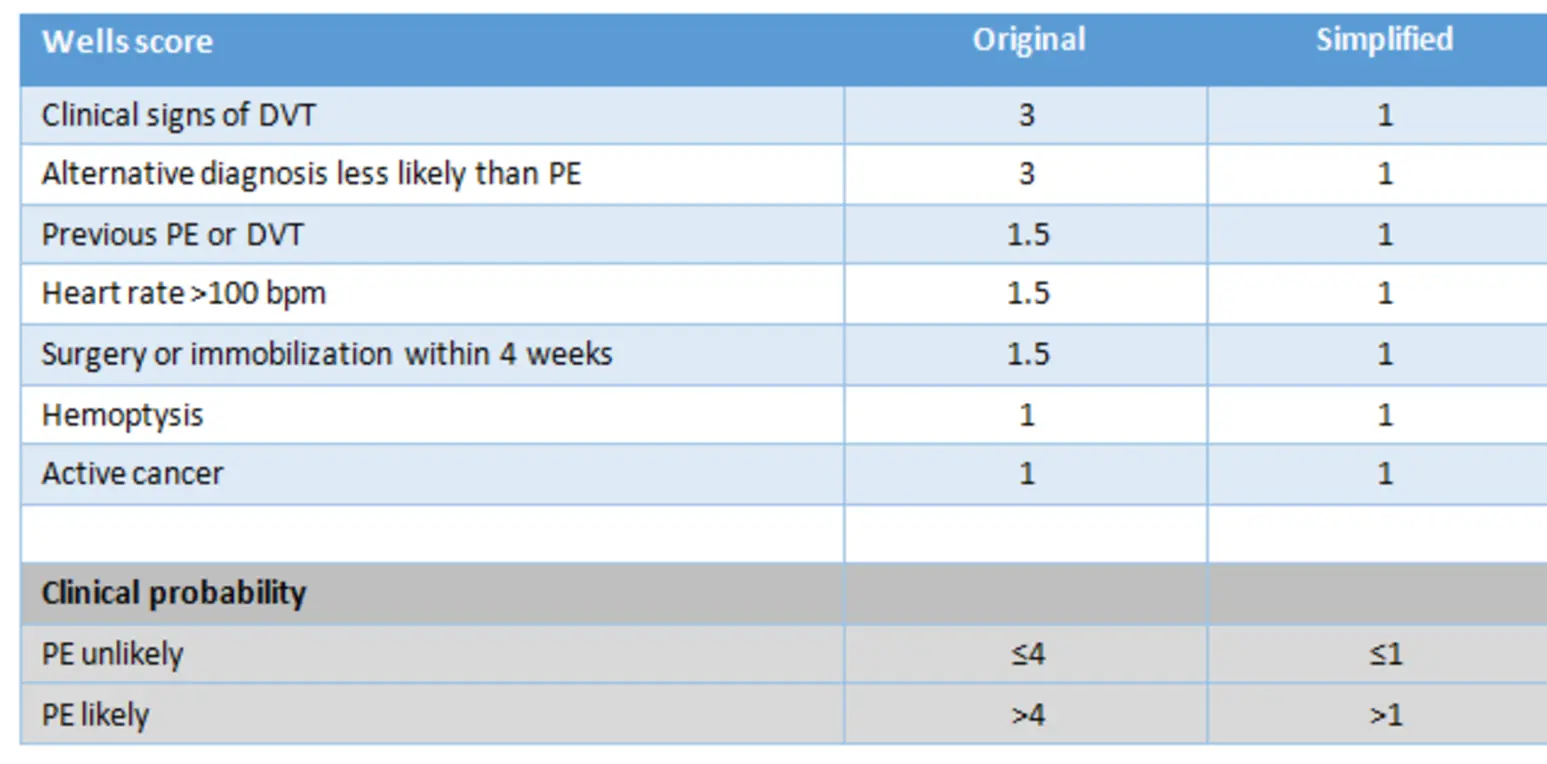
- PERC Score first; if high, do Wells.
- If negative D-dimer helps exclude in low/mod probability.
- Wells Criteria: Clinical signs of DVT (3), Alt diagnosis less likely (3), Heart rate > 100 (1.5), Immobilization (1.5), Previous VTE (1.5), Hemoptysis (1), Cancer (1).
- Likely PE (>4) → do CT. Unlikely (≤4) → do D-dimer.
- Treatment: Anticoagulation (Heparin/LMWH). Thrombolytics in hypotensive/massive PE. IVC filter if bleeding risk.
Diagnostic testing
- Pulmonary angiography (Gold standard)
- Spiral CT (CT-PE protocol)
- V/Q scan (helpful for detecting chronic VTE)
- D-dimer (<500ng/ml helps exclude PE in patient with low/moderate pre-test probability)
Treatment of PE
-
Anticoagulant therapy is primary therapy for PE2
- Unfractionated heparin3
- LMWH4
-
For unstable patients, catheter embolectomy or surgical embolectomy are options5
-
For patients at risk for bleeding, IVC filter is an alternative6
-
thrombolytic or fibrinolytic (Streptokinase) in Hypotensive
-
if massive with normal BP only heparin
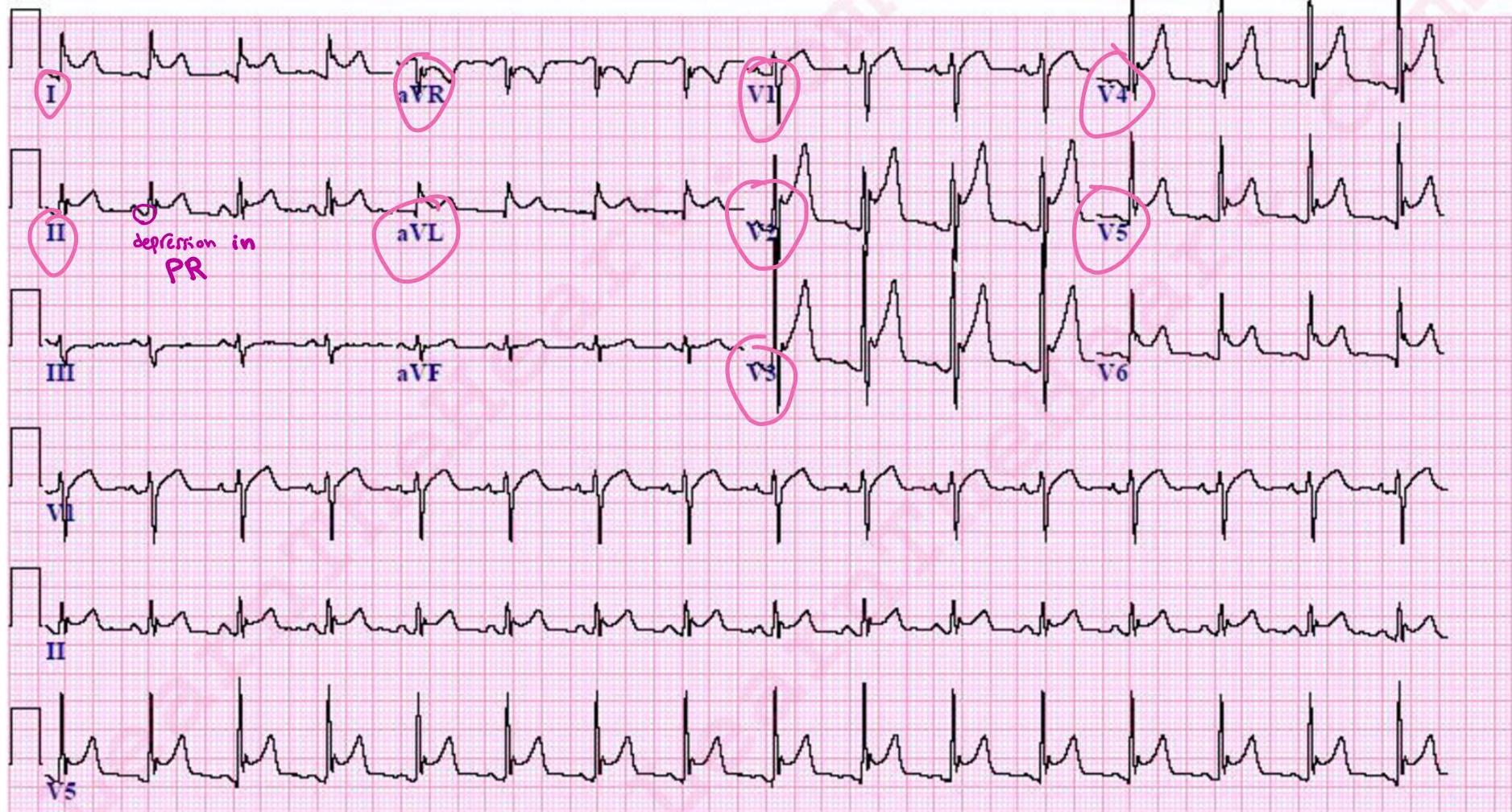
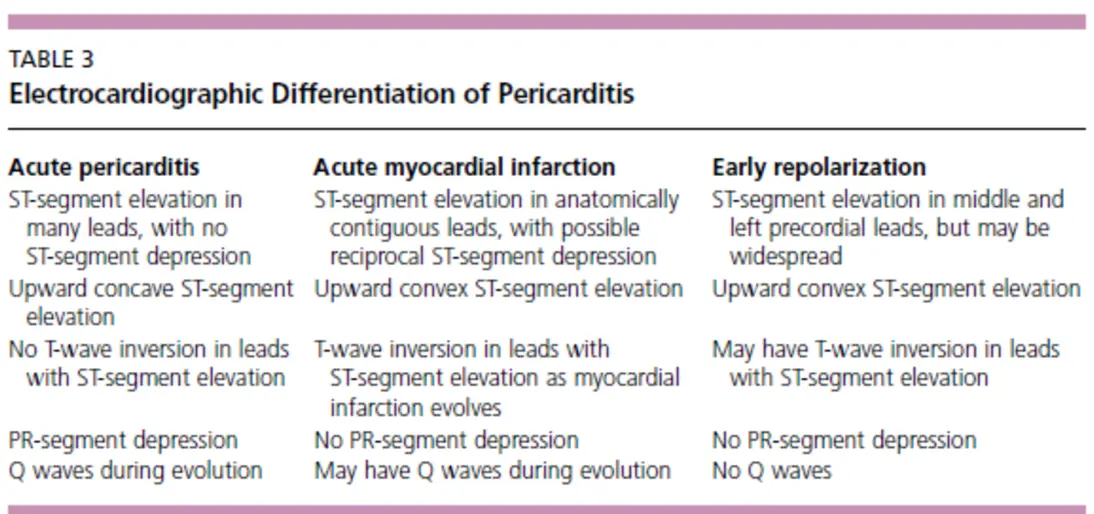
Case 2: Pericarditis
-
Presentation: 24M with PMHx of SLE/Asthma. Sharp, pleuritic pain (2 days), worse lying supine, better leaning forward. Recent viral URI.
-
Vitals: T 38.1, HR 104.
-
Exam: Leaning forward, WBC 14.
-
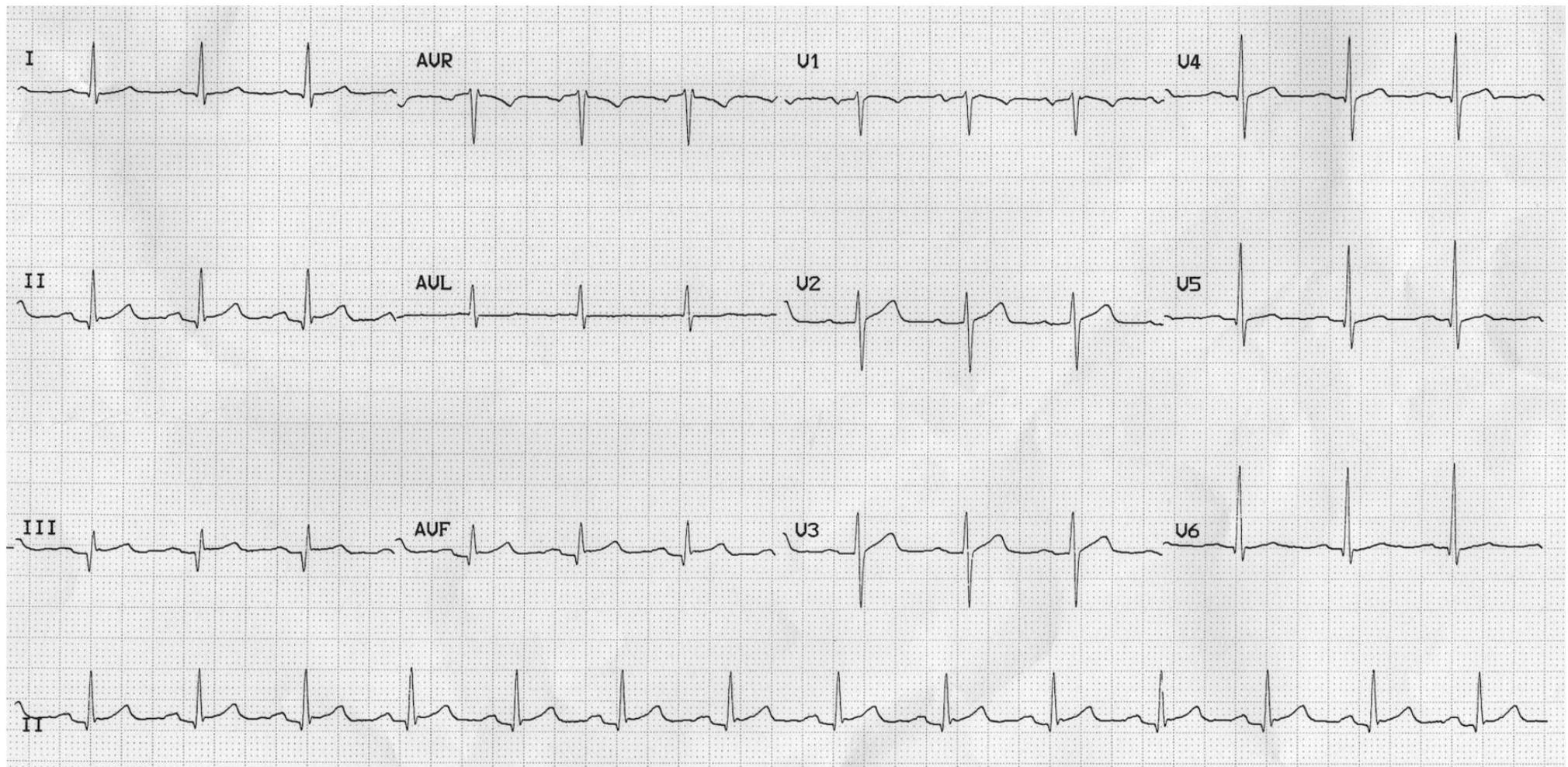
ECG Findings: Diffuse ST elevation and PR depression (elevated in aVR).
-
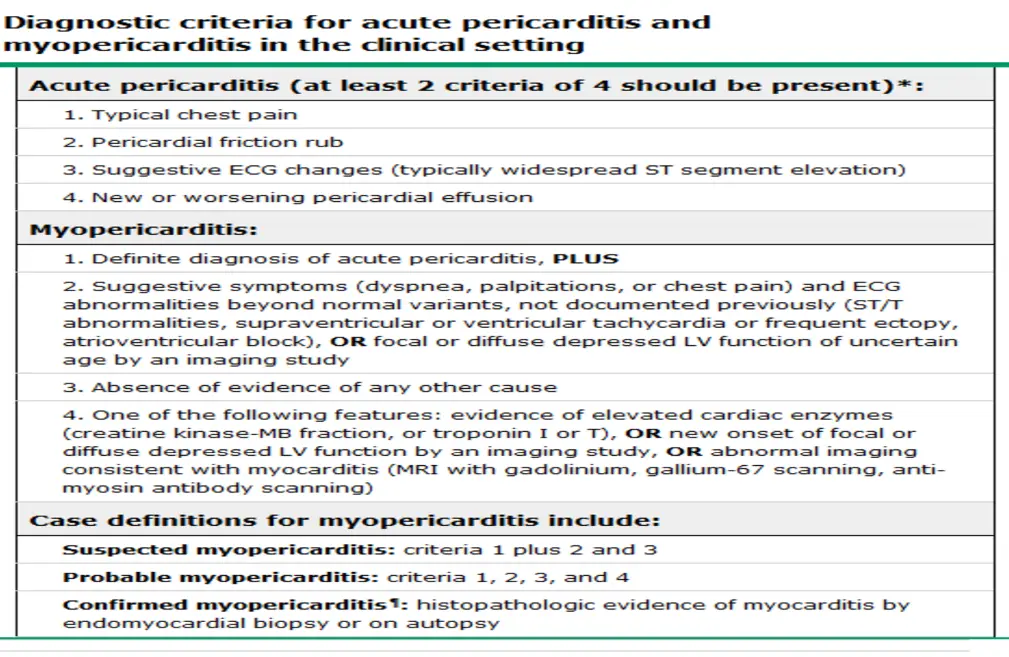
Diagnosis Criteria: Requires 2 of 4 (Typical pain, Friction rub, ECG changes, Effusion).
-
Management: Echo, Aspirin, NSAIDs/Colchicine (“Nidwage” [sic]).
-
EKG Findings:
- PR depression (elevated avR)
- Diffused ST elevation*
-
Diagnostic Steps & Management:
- Order troponin
- If troponin is positive, the diagnosis is Myopericarditis (they may develop HF)
- With troponin -ve: do echo, give aspirin/NSAIDs, and discharge
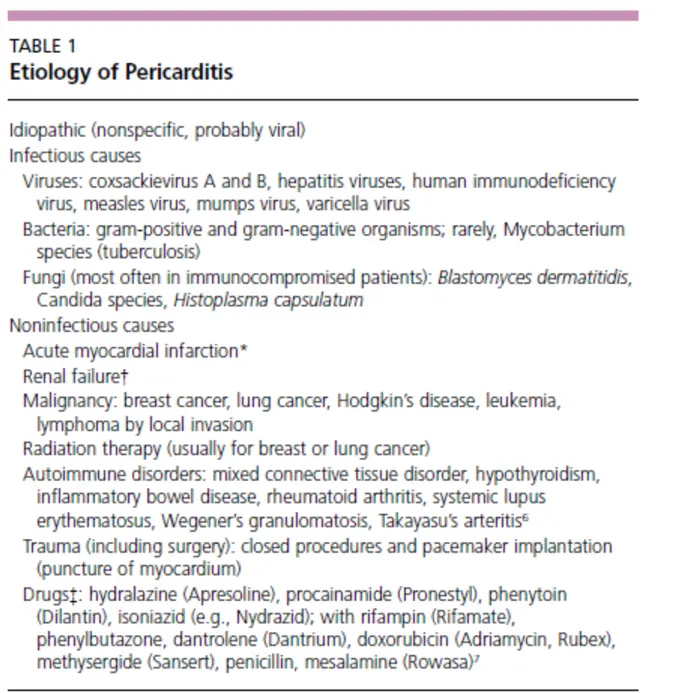 pericarditis:
pericarditis:
- Refers to inflammation of pericardial sac
- Preceded by viral prodrome, i.e. flu-like symptoms
- Typically, patients have sharp, pleuritic chest pain relieved by sitting up or leaning forward
Case 3: NSTEMI vs Aortic Dissection both normal ecg
- Presentation: 67M with DM/CAD. Retrosternal pain (7/10), nausea, diaphoresis, jaw radiation. Similar to prior MI.
- Vitals: HR 108, BP 105/60, Sat 93%.
- Exam: Rales at bilateral bases. tachycardic, nl s1/s2 no murmurs or rub
- Labs: Troponin + 3.2. ckmb = 9 ck = 345
- Clinical Notes: “Sever between scapula pain” [sic].
Management of UA/NSTEMI
-
Aspirin,
- inhibit platelet aggregation
-
Statin,
-
Nitroglycerin (SL).
- use if patient having active chest pain
- Caution: Do NOT use Nitroglycerin if RV infarct concern.
-
HR control (Beta-blocker, goal to titrate ~60 bmr ).
-
Plavix
- P2Y12 receptor blocker
- Inhibits platelet aggregation
-
Anticoagulation
- Heparin/LMWH
- Inhibits thrombus formation
- Heparin/LMWH
-
Oxygen
- For O₂ sat < 90%
-
Morphine
- For refractory chest pain, unrelieved by NTG SL
Pit for cath or CABG depend on his case
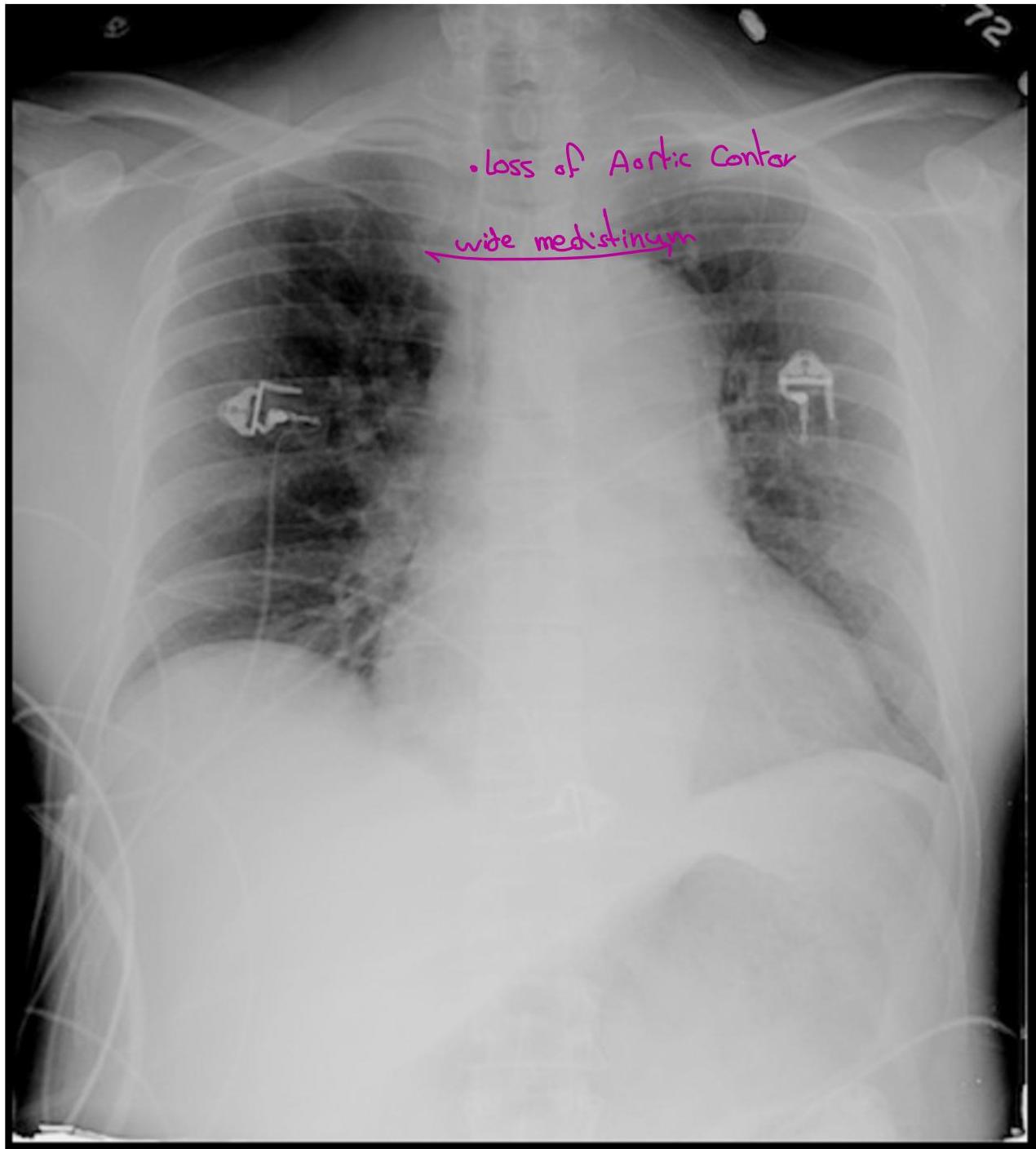
Case 4: Aortic Dissection
- Presentation: Crushing chest pain radiating to the back.
- Key Finding: BP discrepancy (R: 193/112, L: 160/99).
- Classification: Type A (Ascending - Surgical), Type B (any other part of aorta).
- Diagnostics: CXR, CT chest with contrast, MRI chest, TEE
Management of Aortic Dissection
- Type A dissection – Surgical
- Type B dissection – Medical
- Mainstay of medical therapy
- Pain control
- HR and BP control
- Goal HR = 60 beats/min, goal SBP = 100-120 mmHg
- Use IV beta-blockers (i.e. Labetalol, Esmolol)
- Can also use Nitroprusside for BP control
- AVOID Hydralazine
Case 5: Pneumothorax
- Presentation: 45M post-thoracentesis (1.5L removed). Develops sudden R-sided chest pain.

- Management:
- Stable < 3cm: Supplemental O2 and observation.
- Stable > 3cm: Needle aspiration.
- Failure or Unstable: Chest tube. if >3cm or failed aspiration or unstable patient
Summary
- Chest pain is a very common complaint that has a broad differential
- Always try to rule out the life-threatening causes of chest pain
- It is important to remember that troponin elevation DOES NOT always mean ACS
- Use the history, physical exam, labs, EKG and imaging to reach a diagnosis (Good H is the most important)
- Whenever you are stuck, ask for help. Your seniors are there to help you!!