Diabetic Emergencies
Lecturer: Bader Alyahya
1. Hypoglycemia
Definition:
- Triad: Glucose less than + Signs/symptoms + Response to Glucose.
- More common in Type 1 than Type 2 diabetes.
- It is the most common cause of coma associated with diabetes.
- Associated with significant morbidity and mortality.

Causes
- Type 1: Taking insulin with missing meal.
- Type 2: High dose of oral hypoglycemic.

Other potential causes:
- Overaggressive insulin therapy.
- Longer history of diabetes.
- Autonomic neuropathy.
- Decreased epinephrine secretion or sensitivity.
Clinical Picture
Signs and symptoms are caused by excessive secretion of catecholamines and CNS dysfunction:
- Adrenergic: Sweating, Tremors, Nervousness, Tachycardia, Hunger.
- Neuroglycopenic: Neurologic symptoms ranging from bizarre behavior and confusion to seizure and coma.
Hypoglycemia Unawareness:
- Hypoglycemia without warning symptoms.
- Even a single hypoglycemic episode can reduce neurohumoral counter-regulatory responses to subsequent episodes.

Management & Disposition
Treatment:
- D50% 1-2 vials (IV - IO - Central).
- If no line: Glucagon 1-2 mg IM.
- Note: If profound hypoglycemia give octreotide (somatostatin).


Disposition:
- Insulin induced hypoglycemia: Can be discharged except for Lantus insulin (long acting).
- Oral hypoglycemic induced: Needs admission for 24h (due to half life of drug).
2. Diabetic Ketoacidosis (DKA)
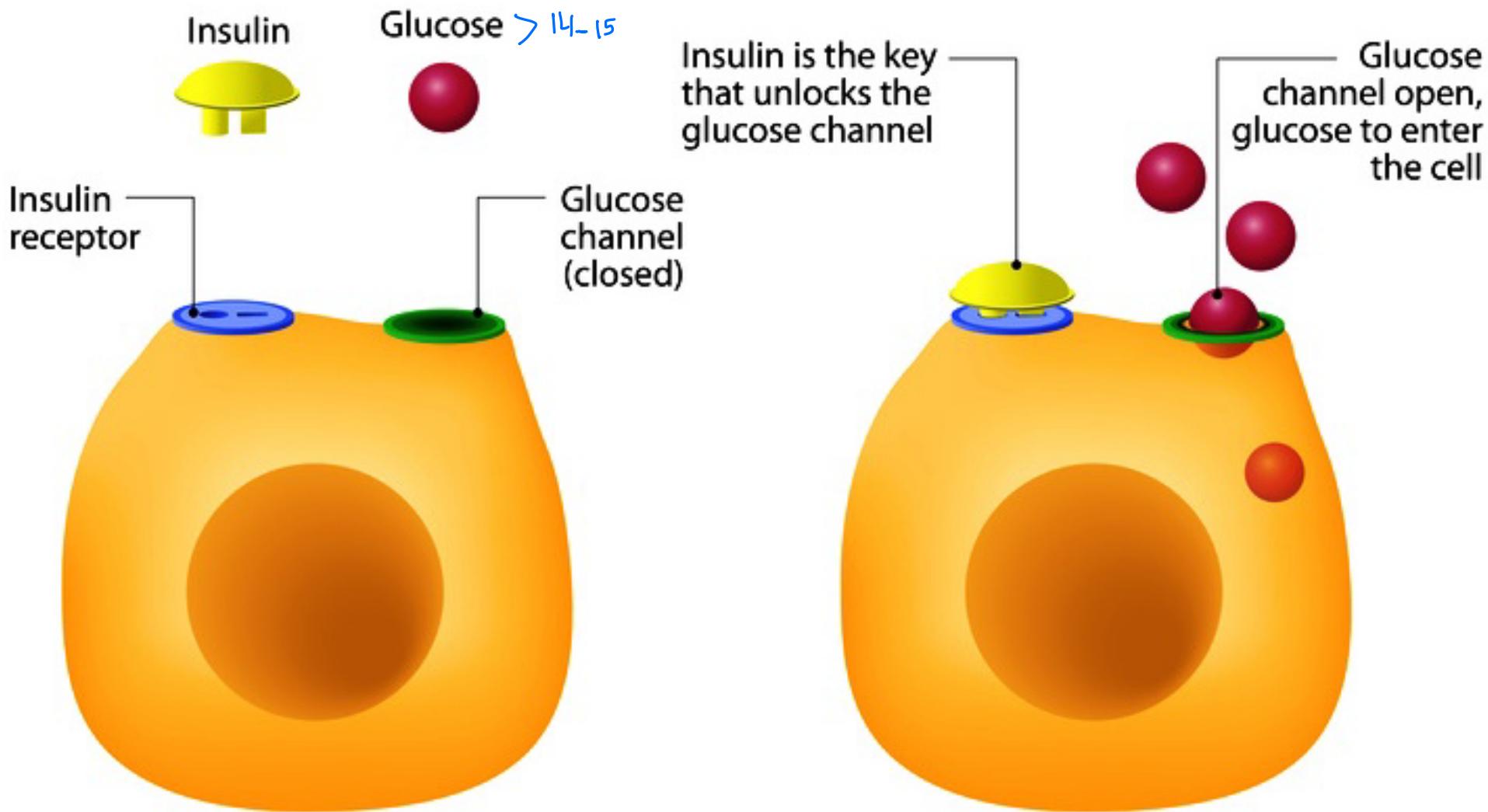
Insulin Function & Physiology
Mechanism of Insulin Action: Diagram Description:
- Basal State: Insulin and Glucose are separate; Glucose channel is closed.
- Insulin Action: Insulin inserts into the receptor unlocks glucose channel Glucose enters cell.
- Concept: Insulin is the key that unlocks the glucose channel.
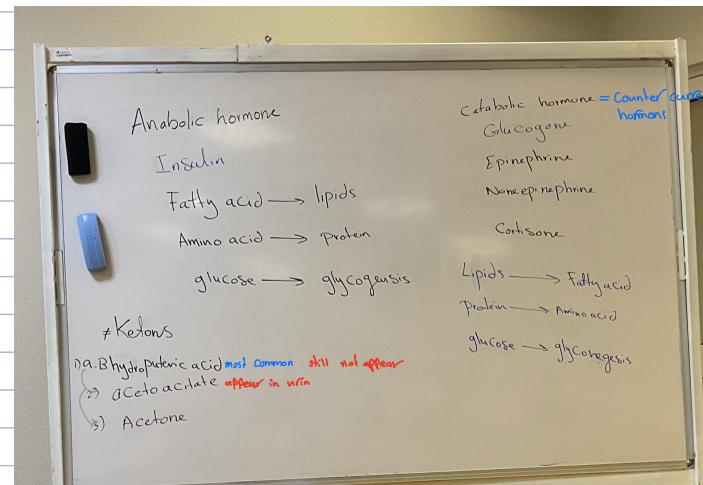
Hormonal Balance (Whiteboard Notes):
- Anabolic hormones (Insulin):
- Fatty acid lipids
- Amino acid protein
- Glucose glycogenesis
- Catabolic hormones (Glucagon, Epinephrine, Norepinephrine, Cortisone):
- Lipids Fatty acid
- Protein Amino acid
- Glucose glycogenolysis
General Principles
- 5% of Type 2 DM has overlap or may have DKA.
- MODY Type 3 DM: DM Type 1 in old age or DM Type 2 in young age.
- Euglycemic DKA: 10% of DKA patients have normal Blood glucose (e.g., took insulin dose before ER).
- Diagnosis: Complete certainty depends on Anion Gap.
- Normal anion gap = 100% DKA excluded.
- Absence of Ketones in urine doesn’t exclude DKA (early presentation involves -hydroxybutyric acid which does not appear in standard urine ketone tests).
- pH may be normal in mixed Metabolic acidosis and alkalosis.
Ketones:
- -hydroxybutyric acid (Most common, does not appear in urine tests).
- -ketoacetate (Appears in urine).
- Acetone (Fruity smell).
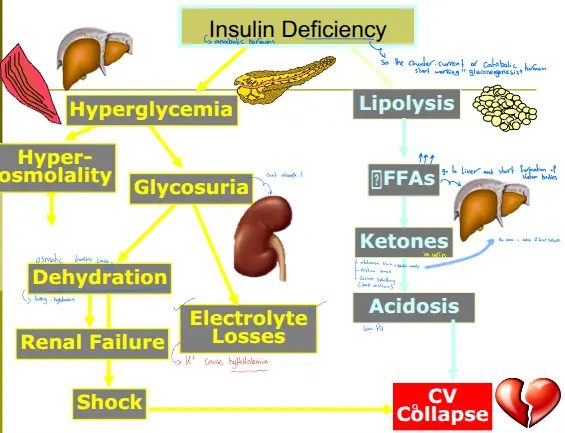
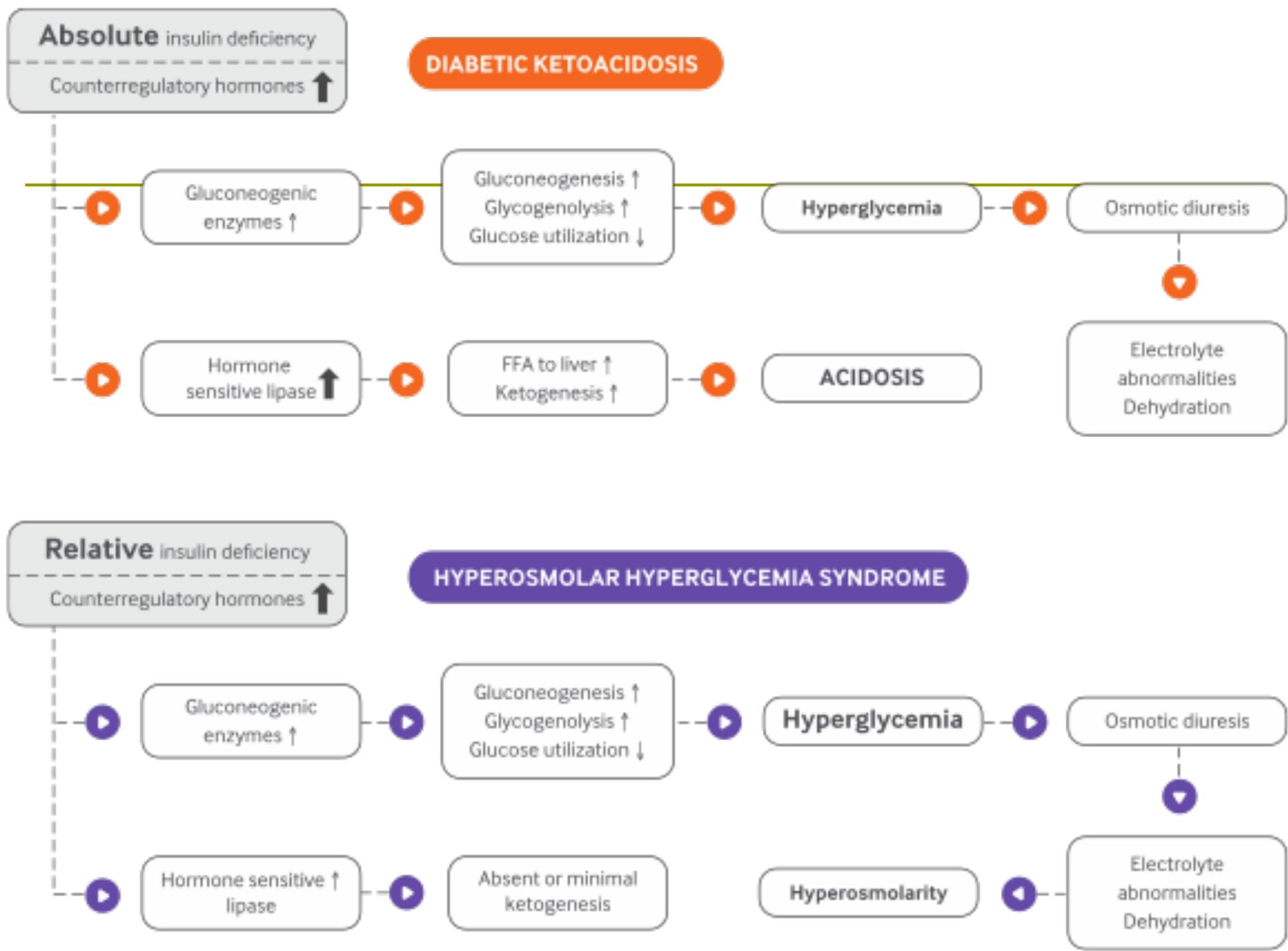
Pathophysiology
Complete or relative absence of Insulin and excess Counter-regulatory hormones result in:
- Hyperglycemia (Gluconeogenesis)
- Ketone formation (Lipolysis FFAs Liver)
- Wide anion gap metabolic acidosis
Sequence of Events:
- Insulin Deficiency: Anabolic hormone lost Catabolic hormones take over (Gluconeogenesis).
- Hyperglycemia Glycosuria Osmotic diuresis Dehydration (Tachycardia, Hypotension) & Electrolyte Losses ().
- Dehydration Renal Failure / Shock / CV Collapse.
- Ketosis Acidosis (Low pH) Kussmaul breathing, Acetone smell, Abdominal pain (stretch of liver capsule).
Diagnostic Criteria
Suspect DKA if:
- pH
- Bicarbonate
- Anion gap
- Formula: Serum Na – (chloride + bicarbonate)
- Ketones: Positive serum or urine ketones (Urine/Serum).
- Plasma glucose () (but may be lower).
- Precipitating factor present.
Precipitating Causes & treat cause
- Omission of insulin injection (MOST COMMON CAUSE).
- Dislodged or obstructed insulin pump.
- Infection / Sepsis (Primary reason for failure to respond).
- Pregnancy.
- Medication.
- CVA.
- GI Hemorrhage.
- Pancreatitis.
- Myocardial infarction (Small troponin rise may occur without ischemia; ECG changes may reflect hyperkalemia).
- Thyrotoxicosis.
- New diagnosis of diabetes.
- Idiopathic (approx. 15%).

Investigations
- VBG, electrolytes, serum/urine ketones, Renal profile.
- Note: Urine test can only detect AcAc.
- High anion-gap can be the only clue to presence of metabolic acidosis.
- Sodium Correction: Add to reported Na for every of glucose over .
- WBC: Increased due to stress & hemoconcentration (absolute bands predict infection).
Management
Pillars of Treatment: Fluids, Potassium, Acidosis.
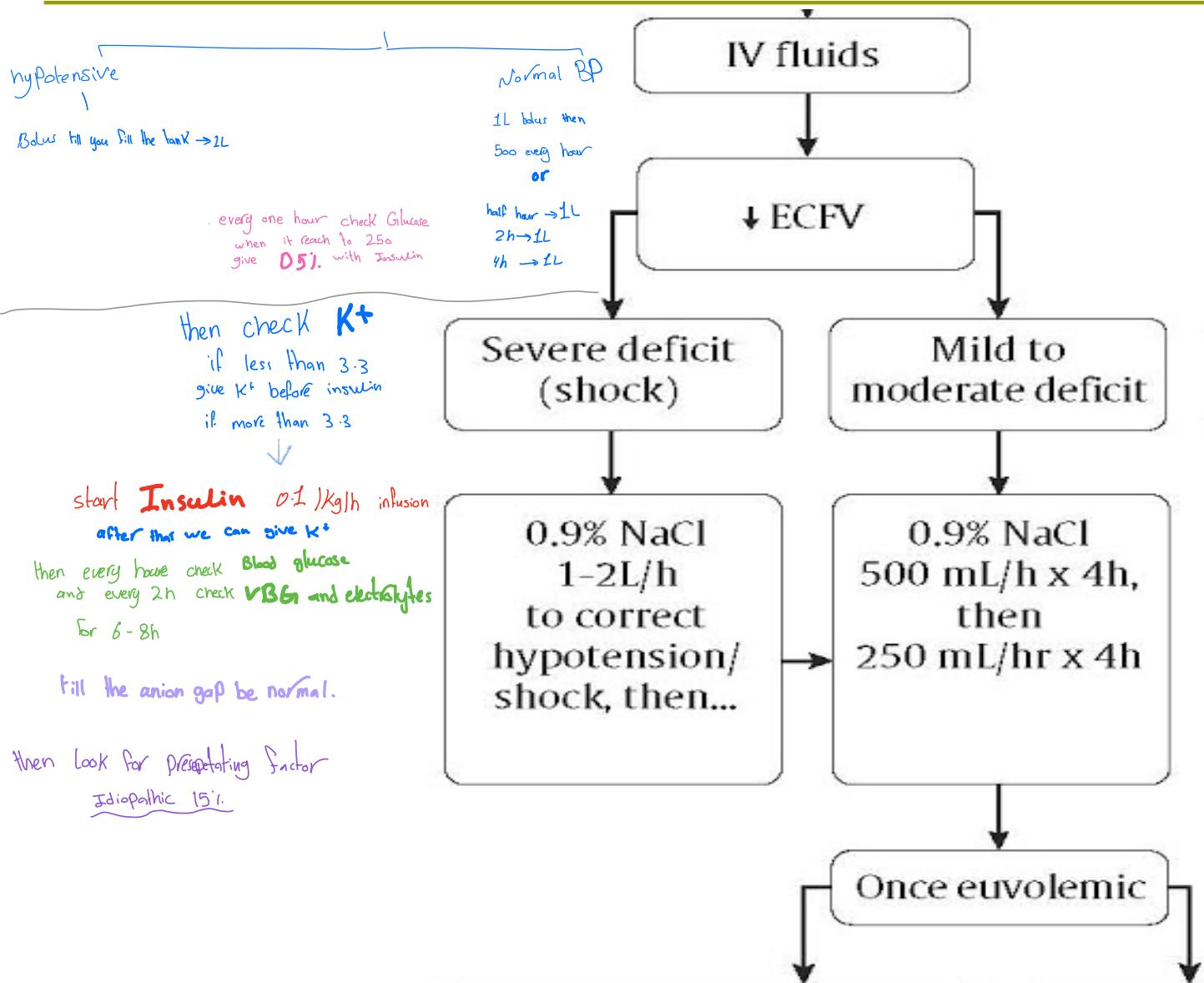
1. Fluids (Resuscitation)
- Goal: Replace Fluids with IV 0.9% NaCl until Euvolemic.
- Loss of water is typically 4-6L in DKA.
- Hypotensive: Bolus “fill the tank” 2L.
- Normal BP: 1L bolus 500ml/hr (4h) 250 ml/hr (4h).
- Check Glucose hourly. When glucose reaches () switch to D5% with Insulin.
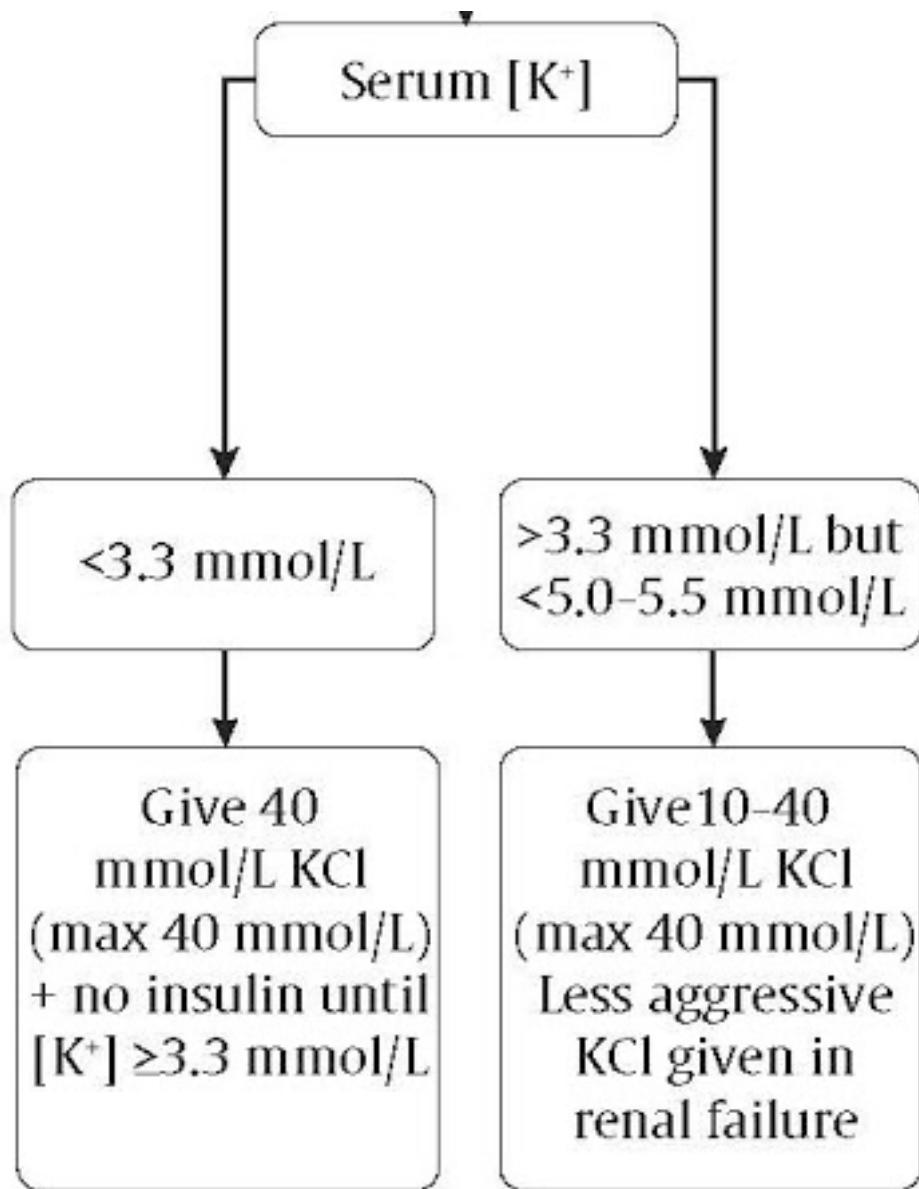
2. Potassium ()
- Hypokalemia is the most life-threatening electrolyte abnormality.
- Physiology: Acidosis shifts OUT of cells (Pseudohyperkalemia). Treating acidosis shifts back IN (risk of severe hypokalemia).
- Rule: Correct FIRST, then start insulin.
- : Give 40 mmol KCl + NO Insulin until .
- : Give 10-40 mmol KCl (Less aggressive in renal failure).
- : No KCl, monitor.
- Other electrolytes: No IV Phosphate used in ED.
3. Acidosis (Insulin)
- Start Infusion: .
- Goal: used Treat the acidosis (normalize Anion Gap), NOT just the glucose.
- Note: ~25% of glucose decrease is driven by fluids alone.
- Maintain insulin until anion gap normalizes.
- Monitor: Glucose every 1h; VBG and Electrolytes every 2h for 6-8h.
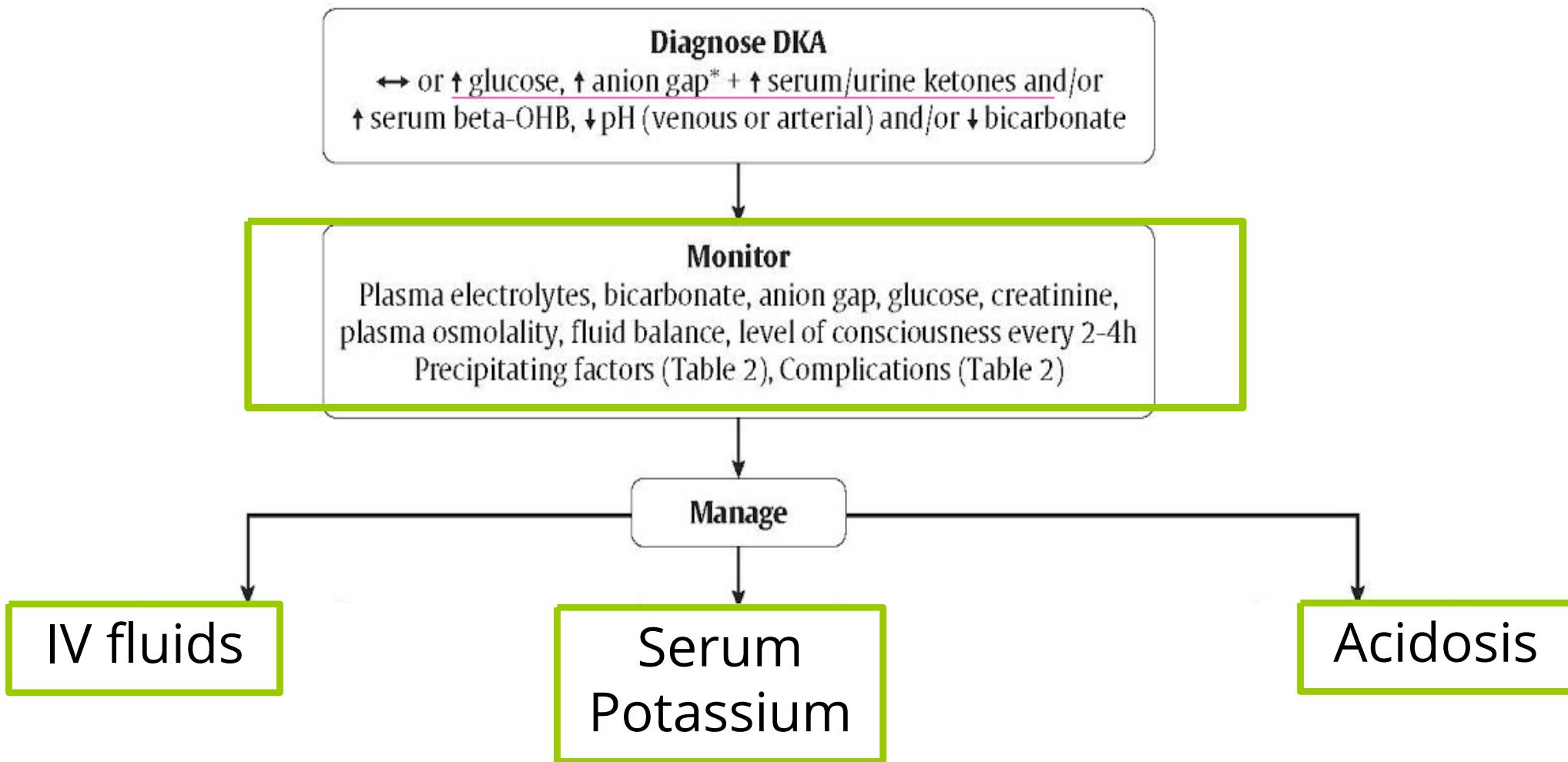
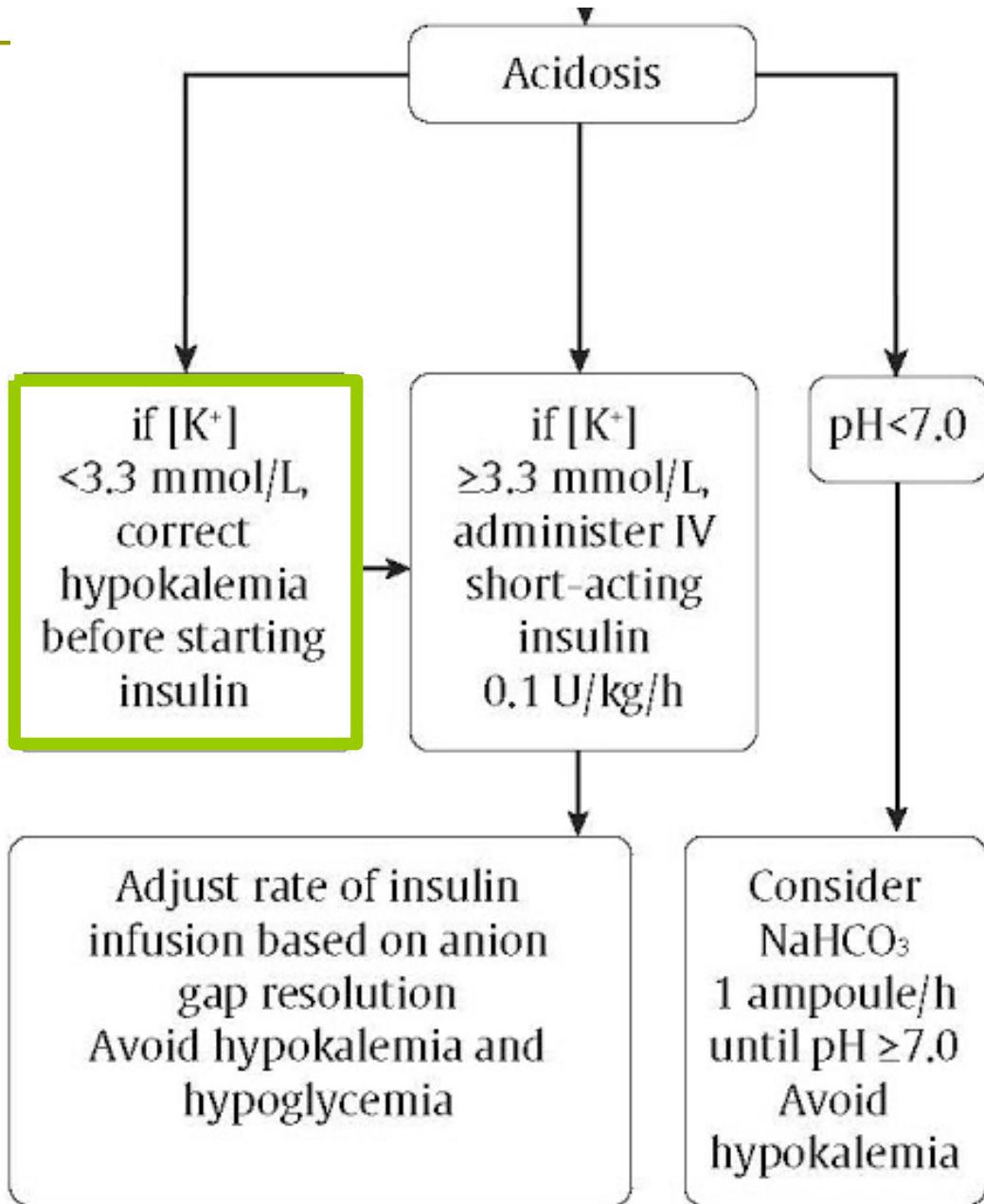
4. Bicarbonate ()
- Not routinely used. Only if pH .
- Give 1 ampoule/h until pH .
- Complications of :
- Hypokalemia.
- Paradoxical CNS acidosis.
- Worsening intracellular acidosis.
- Impaired O2 curve to left.
- Hypertonicity / Na overload.
- Delayed recovery from alkalosis.
- Elevation of lactate.
- Cerebral edema.
Mortality Factors:
- Low (), Infection/AMI, Old age, Severe hypotension/coma.
- Increased Osmolality, BUN, and Blood Glucose.
- Cerebral Edema: (Risk in young/new-onset). If neurologic change occurs Mannitol before CT.
- Note: Vascular thrombosis can occur (CNS).
- Underlying renal and CVS dis. Prolong and severe coma.

3. Hyperosmolar Hyperglycemic State (HHS)
Also known as: Non-Ketotic Hyperosmolar Coma.
Overview & Pathogenesis
- Represents an extreme of the disease process (DKA vs HHS).
- Mechanism: Relative insulin deficiency (enough to prevent ketosis, not enough to prevent hyperglycemia).
- HHS vs DKA:
- Severe Hyperglycemia () & Hyperosmolality ().
- Absence of ketogenesis.
- Profound dehydration (8-12L water loss).
- Higher Mortality (40-60%) due to older age and comorbidities. versus DKA (5-15%)
- Hypokalemia, Sodium variable, Azotemia, Metabolic acidosis (lactic or uremic)
Biochemical Pathway differences:
- DKA: Increased Hormone Sensitive Lipase FFA to liver Ketogenesis Acidosis.
- HHS: Increased Gluconeogenic enzymes Hyperglycemia; but Hormone Sensitive Lipase activity prevents/limits ketogenesis Hyperosmolarity.
Precipitating Causes
70-80% have an identifiable cause:
- Infections: Pneumonia, UTI, Sepsis.
- Events: Stroke, MI.
- Medications: diuresis, phenytoin, diazoxide, steroids, mannitol, cimetidine, immunosuppressive agents, etc.
Recognition
- Onset: Insidious (Days to Weeks).
- Clinical: Confusion, Seizure, Coma + Marked Shock/Dehydration.
- Labs: High Glucose, High Osmolality, No Ketones, Variable Sodium, Azotemia.
Management
Strategy similar to DKA:
-
Fluids: Initiate aggressive rehydration to treat hypovolemia, as patients typically lose 20–25% of their total body water.
- Goal: Replace ½ of the fluid deficit within the first 12 hours and restore urine output to 50 ml/hour.
- Fluid Selection:
- Unstable: Normal Saline.
- Stable: ½ NS or NS (requires close monitoring of fluid status).
-
Insulin: Note that patients are generally less resistant to insulin compared to DKA cases.
-
Dextrose: Add to regimen when blood glucose approaches 300 mg/dl.
-
Electrolytes:
- Potassium: Replace once urine output is established.
- Phosphate: Replace as needed.
- Treat precipitating causes
- Monitor intake and output
- Evaluate for other causes of coma
Comparison: DKA vs HHS
| Feature | Diabetic Ketoacidosis (DKA) | Hyperglycemic Hyperosmolar State (HHS) |
|---|---|---|
| Patient Profile | Younger, Type 1 Diabetes (mostly) | Older, Type 2 Diabetes (typically) |
| Onset | Acute (Hours to 1-2 days) | Insidious (Days to weeks) |
| Insulin Status | Absolute Deficiency | Relative Deficiency |
| Pathophysiology | Ketosis & Acidosis | Hyperosmolarity & Dehydration (No Ketosis) |
| Glucose | (Profound) | |
| pH (Arterial) | ||
| Bicarbonate | ||
| Ketones | Moderate/Severe | Minimal/Absent |
| Osmolality | No hyperosmolality (typically) | |
| Gap | Anion Gap | No Anion Gap |
| Volume Loss | 4-6 Liters | 8-12 Liters (Severe) |
| Mortality | 5-15% | 40-60% |
| Source: AACE (American Association of Clinical Endocrinologists) |
Key Messages
- A normal or mildly elevated blood glucose does not rule out DKA (e.g., in pregnancy or SGLT2 inhibitor use).
- DKA Treatment: IV Insulin () + Fluids + Potassium.
- Bicarbonate: Only for extreme acidosis ().