Diagnosis and Management of Shock
Dr. Hani Albrahim
1. Case Presentation: Initial Encounter
Patient: 20-year-old male History: Brought to ED by Red Crescent with history of chest tightness and shortness of breath (SOB). Physical Exam: Stab wound on the left side of the chest.
Vitals:
- BP: 80/40 mmHg (Hypotensive)
- HR: 120 bpm (Tachycardic)
- O2 Sat: 95%

Decision Point: Now what?
2. Objectives
- Identify the 4 main categories of shock.
- Discuss the goals of resuscitation in shock.
- Summarize the general principles of shock management.
- Describe the physiologic effects of vasopressors and inotropic agents.
3. Definition and Concept
Shock is a state of inadequate blood flow to the tissues of the body resulting from problems with the circulatory system. It is a syndrome of impaired tissue oxygenation and perfusion.
Clinical Pearls:
- “Clinically ill pit”: Patients look sick.
- Hypotension: Every shock state eventually leads to hypotension, though it may not be present initially.
- Risks: If left untreated, it leads to irreversible injury, organ dysfunction, and death.
- Fluid Resuscitation: Patients may not respond to normal saline, but it is given initially because it is fast and accessible while waiting for blood products.
- Surgical Need: Many cases (like trauma) need the Operating Room (OR), but stabilization (e.g., blood) starts immediately.

4. Classification of Shock
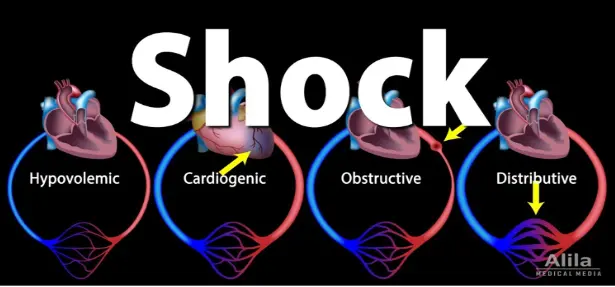
There are four primary classes of shock.
I. Hypovolemic Shock
Characterized by depleted intravascular volume relative to vascular capacity.
- Causes:
- Blood Loss (Hemorrhagic): Trauma, fracture, internal bleeding (e.g., AAA), external bleeding.
- Fluid Loss (Non-hemorrhagic): Vomiting, diarrhea, dehydration, burns.
- Management Focus: Volume replacement (Fluids/Blood). Vasopressors are secondary.
II. Cardiogenic Shock
Forward flow of blood is inadequate due to pump failure (loss of functional myocardium).
- Physiology: Often seen with low Ejection Fraction (EF). Normal is ~55%+.
- Causes:
- Ischemic (ACS/MI)
- Myopathy (e.g., alcohol-induced)
- Mechanical (valvular failure)
- Arrhythmia (e.g., V-tach)
- Management Focus: Antibiotics (if septic component), careful fluids, Inotropes.
III. Distributive Shock
Characterized by a loss of vascular tone (Vasodilation).
- Types:
- Septic Shock: Most common form.
- Anaphylactic Shock: High mortality risk due to airway involvement.
- Neurogenic Shock: Spinal injury.
- Adrenal crisis.
- Drug ingestions.
IV. Obstructive Shock
Physical obstruction to the outflow or impaired cardiac filling.
- Causes & Treatments:
- Cardiac Tamponade: Impairs diastolic filling. Rx: Pericardiocentesis.
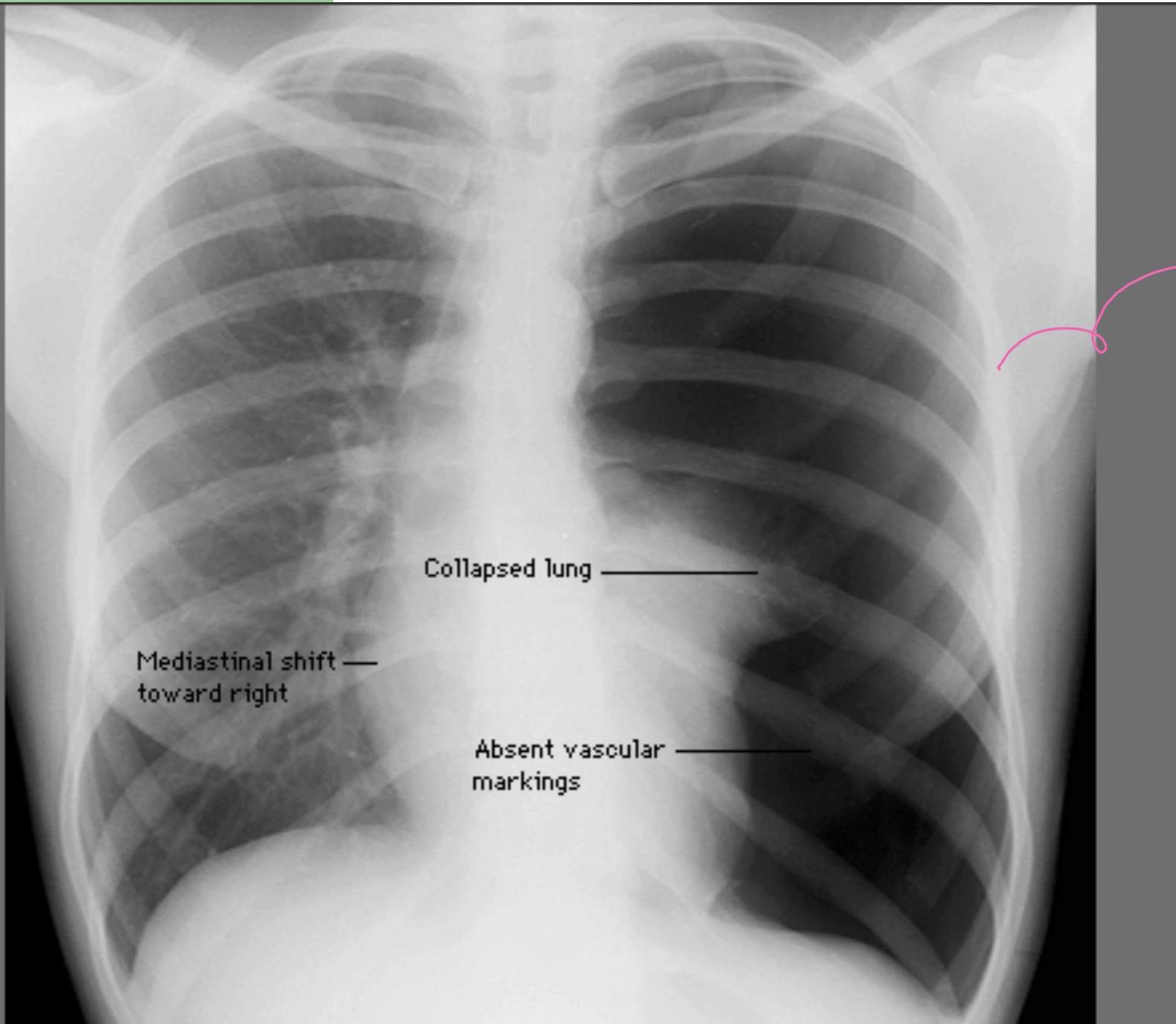
- Tension Pneumothorax: obstructs venous return. Rx: Needle decompression.
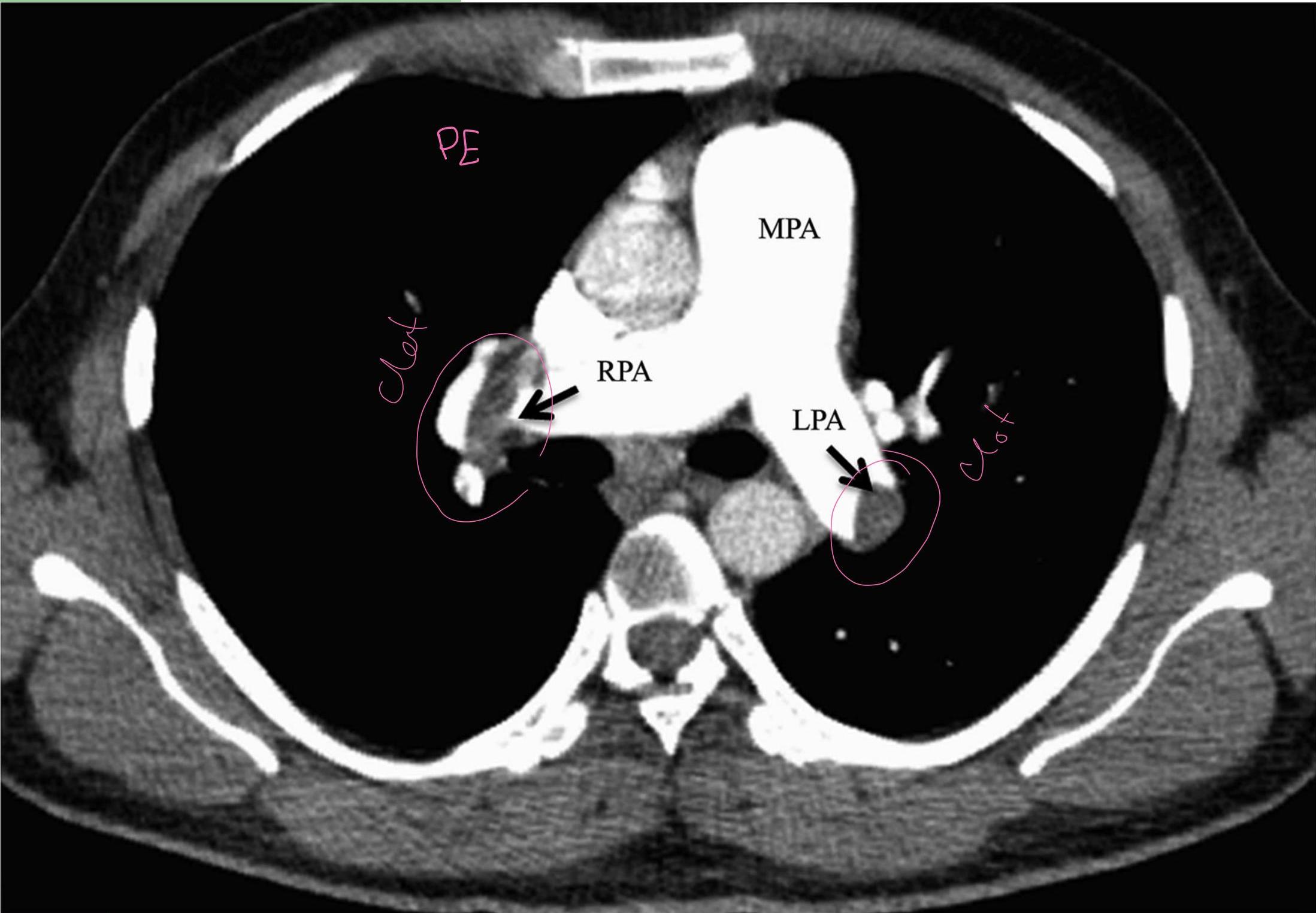
- Massive Pulmonary Embolism (PE): Increases RV afterload. Rx: Thrombolytics.
- Constrictive Pericarditis: Rx: Surgical intervention.
5. Septic Shock & SIRS
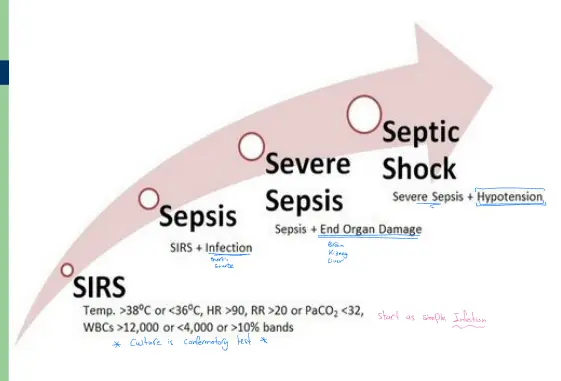
Sepsis Progression: Simple Infection Sepsis Septic Shock End Organ Damage.
Key Target Organs:
- Brain (Confusion)
- Kidney (AKI)
- Liver
SIRS Criteria (Systemic Inflammatory Response Syndrome)
Defining Sepsis typically involves infection + SIRS criteria:
- Temperature: or
- Heart Rate: bpm
- Respiratory Rate: bpm or
- WBC: , , or bands
Note: Culture is the confirmatory test.
6. Clinical Presentation & Diagnosis
Patients may present with a spectrum of signs:
- Subtle: Tachypnea, tachycardia.
- Identifiable: Hypotension, altered mental status (confusion).
Manifestations result from:
- Inadequate tissue perfusion and oxygenation.
- Compensatory responses (adrenergic surge).
- Specific etiology symptoms.
Diagnostic Imaging Examples:
Ischemia/Arrhythmia (V-Tach):


Echocardiography (EF reduced to 20%):


Tension Pneumothorax (Collapsed lung, Mediastinal shift, Absent lung markings):
Pulmonary Embolism (CT Angio):
Tamponade:

7. Management Principles
General Management (The ABCs)
The overall goal is to improve oxygen delivery to prevent cellular and organ injury. Effective therapy requires treatment of the underlying etiology. Interventions to restore mormal perfusion by achieving adequate B.P, increasing cardiac output and optimizing oxygen content of the blood
- Early Identification
- ABC: Airway, Breathing, Circulation.
- Early IV Antibiotics: If infection is suspected.
- Volume Replacement: IVF (Normal Saline) or Blood products.
- Treat the Underlying Cause.


Specific Management by Type
Hypovolemic Shock
- Goal: Restore volume lost (blood, GIT, Urinary, Dehydration).
- Action: IVF vs. Blood.
- Note: Vasopressors are only a temporary bridge to restore BP until fluid resuscitation takes place.
Distributive (Septic) Shock
- Goal: Restore intravascular volume. The most common form of distributive shock is septic shock
- Action:
- IVF resuscitation.
- Early appropriate antibiotics.
- Treat underlying source (e.g., infected diabetic foot).
- Inotropes/Vasopressors: Indicated if hypotension persists despite fluids.
Cardiogenic Shock
● Forward flow of blood is inadequate because of pump failure due to loss of functional myocardium ● The main goal is to improve myocardial function - It is the most severe form of heart failure and it is distinguished from chronic heart failure by the presence of hypotension,hypoperfusion and the need for different therapuetic inteventio
- Goal: Improve myocardial function.
- Action:
- Treat arrhythmias.
- PCI (Percutaneous Coronary Intervention) for ACS.
- Inotropes and vasopressors to support pump function.
Obstructive Shock
● Obstruction to the outflow due to impaired cardiac filling and excessive after load ● Cardiac tamponade and constrictive pericarditis impair diastolic filling of the right ventricle ● Tension pneumothorax limit right ventricular filing by obstruction of venous return ● Massive pulmonary embolism increase right ventricular afterloa - Treat the underlying cause Z
- Goal: Relieve the obstruction.
- Action:
- Tension Pneumothorax Needle Decompression.
- Tamponade Pericardiocentesis.
- Massive PE Thrombolytics.
8. Vasopressors & Inotropes
Definitions
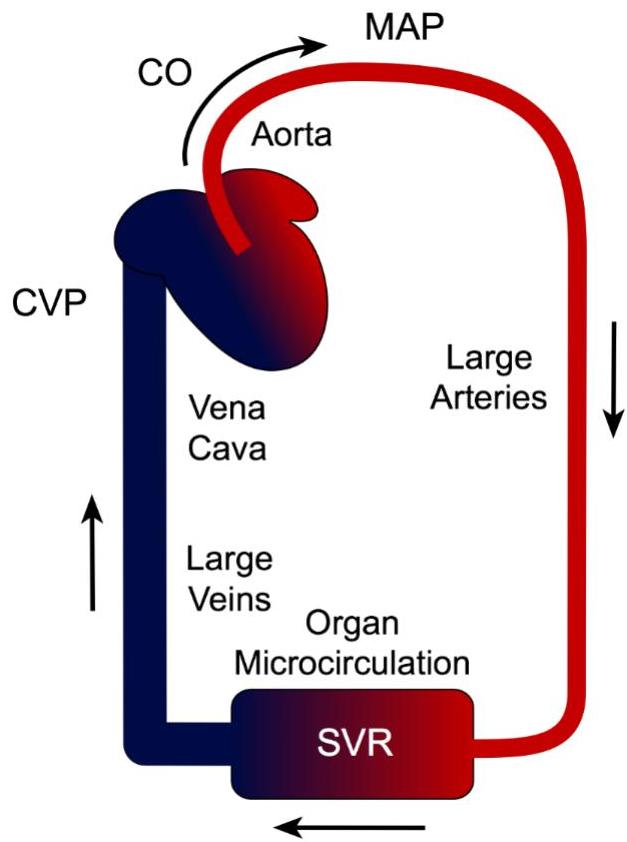
- Vasopressors: Drugs that elevate Mean Arterial Pressure (MAP) via vasoconstriction. Indicated if SBP drops from baseline or MAP .
- Inotropes: Drugs that increase cardiac contractility.
Many drugs have both vasopressor and inotropic effects. ▪ Vasopressors are indicated for a decrease of >30 mmHg from baseline systolic blood pressure or MAP <60 mmHg, when either condition results in end- organ dysfunction secondary to hypoperfusion.
Formula:

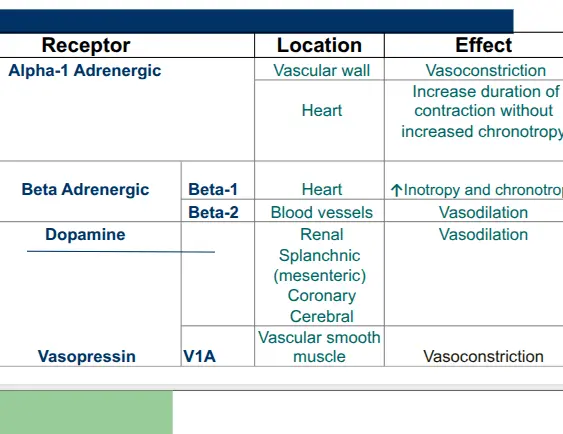
Receptor Physiology
- Alpha-1 Adrenergic: Vascular wall vasoconstriction; increases duration of heart contraction.
- Beta-1 Adrenergic: Heart; Increases Inotropy (contractility) and Chronotropy (rate).
- Beta-2 Adrenergic: Blood vessels; Vasodilation.
- Dopamine Receptors: Renal, Splanchnic, Coronary, and Cerebral vasodilation. (arrythmogenic - increasing mortality)
- Vasopressin (V1): Vascular smooth muscle vasoconstriction.
Comparison Tables
Table 1: Relative Receptor Potency
| Agent | Alpha-1 (VC) | Beta-1 (Inotropy) | Beta-2 (VD) | Dopamine | Vasopressin |
|---|---|---|---|---|---|
| Dobutamine | + | +++++ | +++ | 0 | 0 |
| Dopamine | +++ | ++++ | ++ | +++++ | 0 |
| Epinephrine (best in anaphylaxis) | +++++ | ++++ | +++ | 0 | 0 |
| Norepinephrine (any type of shock) | +++++ | +++ | ++ | 0 | 0 |
| Phenylephrine | +++++ | 0 | 0 | 0 | 0 |
| Vasopressin | 0 | 0 | 0 | 0 | +++++ |
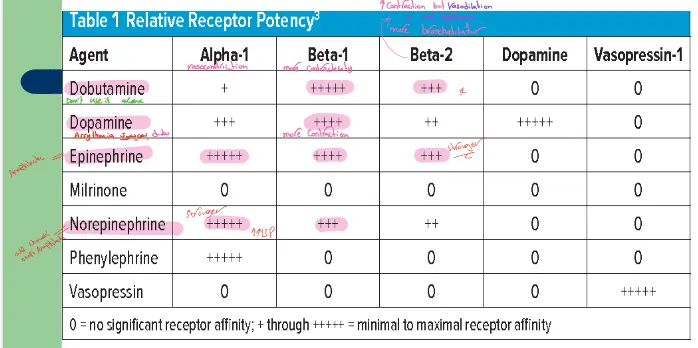 |
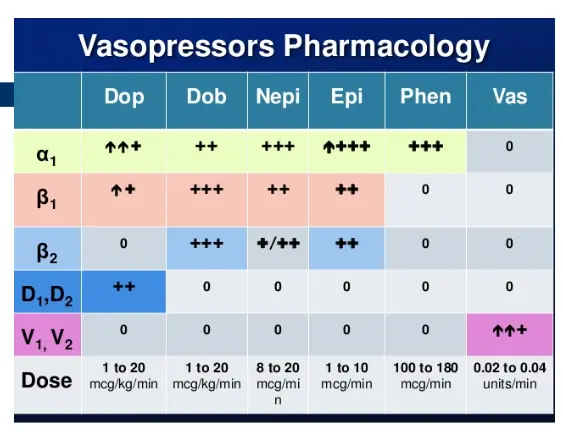
Table 2: Pharmacologic Dosing and Effects
| Receptor/Dose | Dopamine | Dobutamine | Norepi | Epi | Phenylephrine | Vasopressin |
|---|---|---|---|---|---|---|
| ↑↑↑ | ++ | +++ | ↑↑↑↑ | +++ | 0 | |
| ↑↑ | +++ | ++ | ++ | 0 | 0 | |
| 0 | +++ | ↓/↑↑ | ++ | 0 | 0 | |
| Dose | 1-20 mcg/kg/m | 1-20 mcg/kg/m | 8-20 mcg/m | 1-10 mcg/m | 100-180 mcg/m | 0.02-0.04 u/m |
 | ||||||
 |
9. Clinical Scenarios
Scenario I: Septic Shock
- Patient: 72yo F, DM, HTN, altered mental status.
- Vitals: Temp 39°C, BP 70/45 (improves to 80/45 post-IVF), HR 140, Turbid urine (UTI).
- Question: What is the most appropriate 1st line vasopressor?
- A. Epinephrine
- B. Dobutamine
- C. Norepinephrine (First line for Septic Shock)
- D. Dopamine
Scenario II: Cardiogenic Shock
- Patient: 64yo M, CAD, Cardiomyopathy (EF 20%), SOB, Orthopnea, Edema.
- Vitals: Temp 37°C, BP 75/48, hypoxic. CXR: Pleural effusion.
- Question: What is the most appropriate 1st line agent?
- A. Epinephrine
- B. Dobutamine???? - then we add it
- C. Norepinephrine
- D. Dopamine
Scenario III: Anaphylactic Shock
- Patient: 16yo M, Bee sting, SOB.
- Vitals: BP 80/50, HR 140, O2 sat 80%.
- Question: What is the most appropriate 1st line agent?
- A. Epinephrine (IM/IV - First line for Anaphylaxis)
- B. Dobutamine
- C. Norepinephrine
- D. Dopamine
Scenario IV: Septic Shock / CAP
- Patient: 56yo M, Obese, COPD, with Community Acquired Pneumonia (CAP).
- Vitals: BP 80/50, HR 120, Temp 39.5°C, O2 sat 60%.
- Question: What is the most appropriate 1st line vasopressor?
- A. Epinephrine
- B. Dobutamine
- C. Norepinephrine (First line for Septic Shock)
- D. Dopamine