Fever in infants without source
Dr Tariq Al thobaiti ,MBBS
The Febrile Infant - Who Has SBI?
Serious bacterial Infection
all of them are normal








Background
neonate up to one month
Infant up to one year
-
Fever is the most common presenting chief complaint in pediatric patients presenting to the emergency department (ED).
-
Accounting for up to 20% of ED visits.
-
Most cases of fever are viral in origin, benign in course, and resolve spontaneously.
-
Because of the young infants and specially neonates bacterial infection can be missed easily.
-
Before the era of vaccination
Definition
Fever
- Acute fever is fever for <7 days.
- The febrile young infant is defined as an infant < 90 days of age with a rectal temperature .
- In infants and children 3 to 36 months old, the threshold is ( ).
Serious bacterial illness (SBI) is typically defined as the presence of pathogenic bacteria in a previously sterile site and include:
-
Urinary tract infection (UTI),
-
Bacteremia,
-
Meningitis,
-
Osteomyelitis,
-
Bacterial gastroenteritis,
-
Bacterial pneumonia,
-
Cellulitis
-
Septic arthritis
Incidence/Prevalence:
-
The incidence of serious bacterial infection (SBI) in febrile young infants (< 90 days of age) is 8% to 12.5%
-
Higher in neonates (0 through 28 days of age), in whom the SBI rate is nearly 20%.
= one month
Etiology And Pathophysiology
-
The febrile young infant is susceptible to both perinatally acquired and community-acquired infections including group B streptococcus (GBS), Escherichia coli and other gram-negative infections, Streptococcus pneumoniae, and Staphylococcus aureus.
-
The cause of fever varies depending on the age of the child
-
The vast majority of pediatric fever is due to infections
-
the vast majority of infections are attributable to a viral source
-
Bacterial disease is also an important cause of fever in children
-
In all children less than 3 months of age, the urinary tract is the most common site of infection, followed by bacteremia and meningitis.
-
Why Fever tends to be of a higher clinical importance in younger children?
- Infants <3 months of age, and especially neonates, are relatively immunosuppressed
- Incompletely vaccinated.
- Lack of effective communication, neonates and young infants may demonstrate few, if any, clinical clues to an underlying illness. crying only, decrease activity or feeding
- Fever may be the only presenting symptom
- ED management varies dramatically depending on the age due to unique spectrum of age specific pathogens.
- Neonates and young infants demonstrate decreased macrophage and neutrophil function, and bone marrow exhaustion.
- Infants and children demonstrate a poor immunoglobulin G antibody response to encapsulated bacteria until 24 months of age.
- Therefore, the age of the patient and the virulence of the bacteria are considerations for the evaluation of fever in children and the identification of SBI.
Table 165-1 Etiology of Fever in Children
| AGE | BACTERIAL CAUSES | VIRAL CAUSES | OTHER |
|---|---|---|---|
| 0–28 days of age | Group B Streptococcus Listeria monocytogenes Escherichia coli Chlamydia trachomatis Neisseria gonorrhoeae | Herpes simplex virus Varicella Enteroviruses Respiratory syncytial virus Influenza | Bundling Environmental |
| 1–3 months of age | Haemophilus influenzae Streptococcus pneumoniae Neisseria meningitidis E. coli | Varicella Enteroviruses Respiratory syncytial virus Influenza | Bundling Environmental |
| 3–36 months of age | S. pneumoniae N. meningitidis E. coli | Varicella Enteroviruses Respiratory syncytial virus Influenza Mononucleosis Roseola Adenovirus Norwalk virus Coxsackievirus | Leukemia Lymphoma Neuroblastoma Wilms’ tumor |
| 3 years to adulthood | S. pneumoniae N. meningitidis E. coli Group A Streptococcus | Varicella Enteroviruses Respiratory syncytial virus Influenza Mononucleosis Roseola Adenovirus Norwalk virus | Leukemia Lymphoma Neuroblastoma Wilms’ tumor Juvenile rheumatoid arthritis |
Differential Diagnosis
Infectious causes: Bacterial or viral
- Infection is most common cause of fever without source in infants
Noninfectious causes
- Noninfectious causes less common in fever without source in infants and young children
- Recent immunizations
- Malignancy
- Medications associated with fever
- Immunological
- Kawasaki disease
- Immunodeficiency
Protocols & Guidelines
To say this child is well or ill we have to look for 5:
- Tone Ill: Floppy - flat or well moving
- Interactive - interactive with others or not
- Consolable calm down with caregiver (well) — if not or irritable = Ill
- Special cry high pitched cry → well or low pitched cry → ill
- Look and gaze following moving object → well or Fixed gaze → ill
Do we really need them?
-
Studies have been conducted in an effort to identify patients who are low risk for bacterial infections and can be managed safely as outpatients with or without empiric antibiotic treatment.
-
These studies established that certain infants can be managed safely as outpatients and can avoid unnecessary hospitalization.
-
The incidence of SBI among infants categorized as low-risk after appropriate evaluation ranged from 0.5%-1.1% in studies that utilized or excluded the lumbar puncture as part of the initial evaluation, respectively.
-
The Boston, Rochester, and Philadelphia criteria were established from some of the largest and most applicable studies.
| Boston Criteria | Philadelphia Criteria | Rochester Criteria | |
|---|---|---|---|
| Target group and fever definition | |||
| Age range | 28-89 days | 29-60 days | ≤ 60 days |
| Fever defined as | ≥ 38 degrees C (100.4 degrees F) | ≥ 38.2 degrees C (100.8 degrees F) | ≥ 38 degrees C (100.4 degrees F) |
| Criteria for identification as low-risk | |||
| Peripheral WBC count | < 20,000/mm 3 | *≤ 15,000/mm 3 *more than high risk | 5,000-15,000/mm 3 |
| Peripheral band cell count | NA | NA | ≤ 1,500/mm 3 |
| Band/neutrophil ratio | NA | ≤ 0.2 | NA |
| Urinalysis | < 10 WBC/hpf or dipstick negative for leukocyte esterase activity | < 10 WBC/hpf and few or no bacteria on spun specimens | Normal |
| Cerebrospinal fluid | < 10 WBC/mm 3 | < 8 WBC/mm 3 in nonbloody specimen, negative Gram stain microscopic | NA |
| Chest x-ray | No infiltrate (if chest x-ray done) | No evidence of discrete infiltrate | NA |
| Stool smear | NA | Negative for blood with few or no WBC | < 25 WBC/hpf |
| Appearance | Well-appearing | Well-appearing | Well-appearing |
| History | No history of
| No recognizable immunodeficiency syndrome | Previously healthy with no history of
|
| Physical exam | No evidence of soft tissue, bone, or ear infection; no dehydration | No evidence of any bacterial infection | No evidence of skin, soft tissue, bone, joint, or ear infection |
| Reference for derivation | J Pediatr 1992 Jan;120(1):22 | N Engl J Med 1993 Nov 11;329(20):1437full-text | J Pediatr 1985 Dec;107(6):855, J Pediatr 1988 Mar;112(3):355 |
Diagnostic Performance for Identifying Serious Bacterial Infection in Validation Studies:
| Philadelphia Criteria | Rochester Criteria | |
|---|---|---|
| Sample size | Reference for validation | 931 well-appearing febrile infants ≤ 60 days old |
| Number (%) meeting low-risk criteria | 101 (24%) | 437 (46.9%) |
| Number (%) with serious bacterial infection | 43 (10.2%) | 66 (7.1%) |
| Sensitivity | 100% | 92% |
| Specificity | 26.6% | 50% |
| Positive predictive value (high-risk group) | 13.4% | 12.3% |
| Negative predictive value (low-risk group) | 100% | 98.9% |
| Reference for validation | Pediatrics 1999 Mar;103(3):627 | Pediatrics 1994 Sep;94(3):390 |
Which one to choose?
Limitations
-
These studies varied in their patient population, inclusion/exclusion criteria, and uniformity in workup and management.
-
This had led to a lack of consensus and debate concerning the best approach to care for the febrile infant.
-
Despite the established guidelines, variability in application exists among many practitioners.
-
Infants <28 days have found an increased number of missed SBI in this age group and higher prevalence of SBI when compared to their older counterparts.
-
The patient population in the Boston and Philadelphia studies excluded infants under 1 month of age.
-
A retrospective study that applied these low-risk criteria to febrile infants 1-18 days of age revealed a negative predictive value of 97% for both protocols.
-
The Philadelphia and Rochester protocols also were reevaluated a prospective study that enrolled infants 56 days or younger. The authors here found the negative predictive value for the Philadelphia and Rochester criteria to be 97.1% and 97.3%, respectively, compared to the original report of 99.7% and 98.9%, respectively.
History and Physical for young infants <90 days
full history full exam from head to toe
History & Physical
- Used to identify possible causes and assess risk for serious illness
- If the physical examination does not identify a source of infection causing fever, decision making is based first upon age and then by height of fever.
- There are no absolute rules in the evaluation and management of fever
History
- Ask how temperature was taken (accuracy of temperature reading depends on measurement method)
- Bundling may increase skin but not rectal temperature.
Medication history
- Ask about recent or regular medication use or possible accidental ingestion, including
- antipyretics
- acetaminophen
- ibuprofen
- aspirin
- antibiotics which may
- affect evaluation by partially treating infection or confounding culture results
- be associated with fever due to drug hypersensitivity
- antipyretics
- If infant is breastfeeding, ask about mother’s medications
- may partially treat infection
- may confound cultures
- may be associated with fever or drug reactions
Past medical history (PMH):
- ask about prior febrile illnesses
- immunization status
- as potential cause of fever
- to determine susceptibility to pathogens
- chronic illness
- seizures
- prematurity
- presence of indwelling medical devices
- periodic fever syndromes and autoinflammatory syndromes associated with recurrent fevers in children
Social history (SH):
- ask about
- exposure to illness in family members, caretakers, friends, or others
- daycare
- travel history, including
- list of exposures and risk factors
- information about pre-travel immunizations or chemoprophylaxis during travel
- description of accommodations
- Reference - Am Fam Physician 2003 Oct 1;68(7):1343
Review of systems (ROS):
to identify possible etiology for fever consider asking about
- lethargy
- irritability
- apnea
- shaking
- sweating
- decreased appetite or feeding difficulties
- congestion
- cough
- eye redness or discharge
- batting at ear
- trouble swallowing
- tachypnea
- dyspnea
- wheezing
- vomiting
- diarrhea
- rash
- cyanosis
- jaundice
- seizures
- joint swelling
Physical
General appearance
Pediatric Assessment Triangle
- The pediatric assessment triangle (PAT) offers a sensible, orderly approach that can be used to assess children of all ages, identify abnormal cardiopulmonary physiology, and define the urgency and need for lifesaving interventions. Before touching the patient, one should observe the child from a distance for visual and auditory clues.
Temperature measurement
- GO for Rectal
Consider Fever if or more
3 weeks baby: Fever
- good tone
- Interactive
- high pitch cry
- Consolable
- temp
Skin
- look for
- specific rash
- blistering or ulcerating lesions
- petechiae
- cyanosis or pallor
- capillary refill time 3 seconds
- evaluate skin turgor (hydration status)
HEENT
- look for bulging or sunken fontanelle
- red tympanic membrane
- nasal flaring
- nasal discharge
- red throat or gums
- ulcerations
- dry mucous membranes
Neck:
- evaluate for nuchal rigidity
Cardiac:
- listen for cardiac murmur
Lungs:
- evaluate inspiration and expiration
- listen for wheezing, rales
Abdomen:
- evaluate for tenderness, distention, mass
Workup For Alternative Sources Of Infection
-
Controversy exists as to the extent of testing that should be performed in febrile young infants with alternative sources of fever, such as viruses.
-
does the febrile infant aged < 90 days with bronchiolitis require the full sepsis workup, or can the fever be attributed to a viral source?
-
concomitant bacterial and viral infections can occur, but viral infection may suggest lower risk of bacterial infection in febrile infants
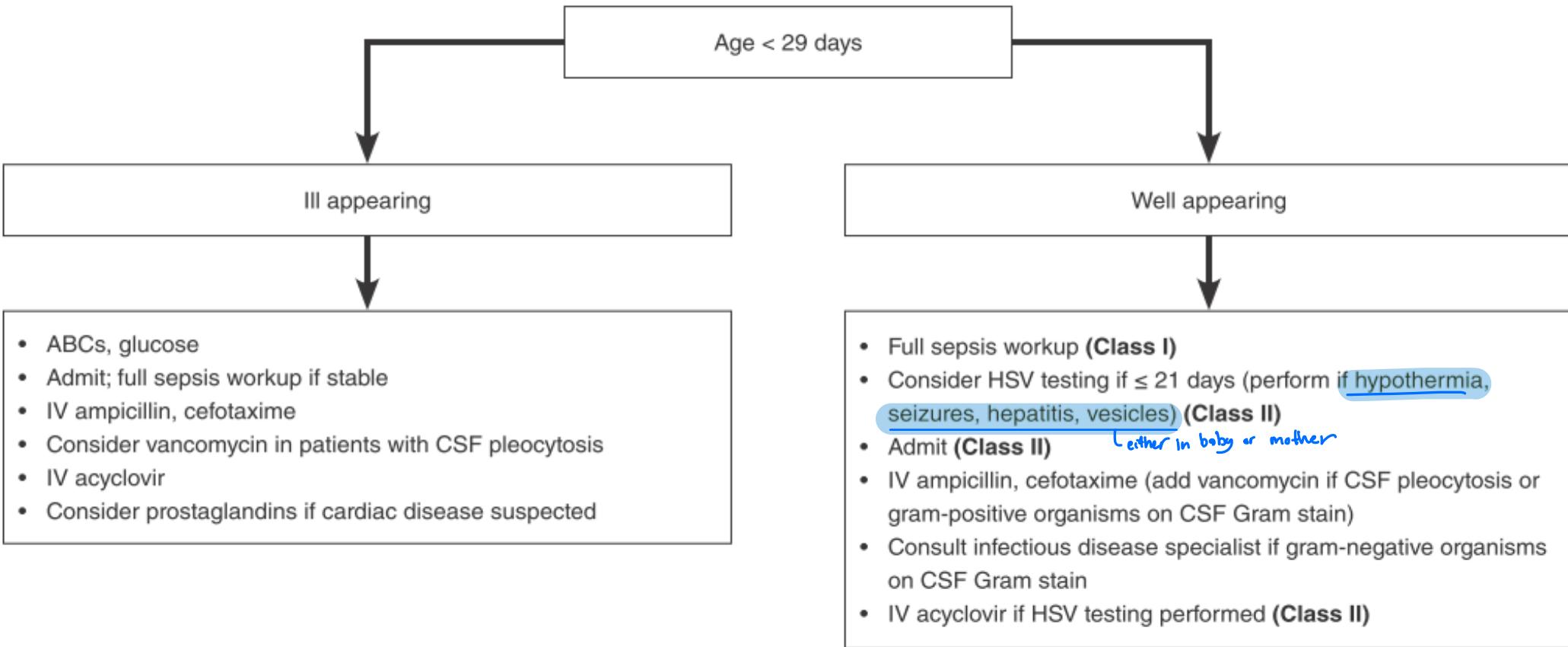
Birth-28 days old
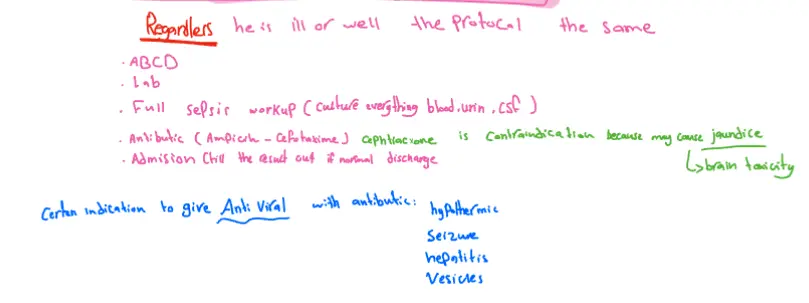
Regardless he is ill or well the protocol the same
- ABCD
- Lab
- Full sepsis workup (culture everything blood, urine, CSF)
- Antibiotic (Ampicillin - Cefotaxime) cephtriaxone is contraindication because may cause jaundice
- Admission till the result out if normal discharge
→ brain toxicity Certain indication to give Anti Viral with antibiotic:
- hypothermic
- Seizure
- hepatitis
- Vesicles
 ~ lina serhan
~ lina serhan
Clinical Pathway For Evaluation Of Febrile Young Infants (< 29 Days Old) <1M
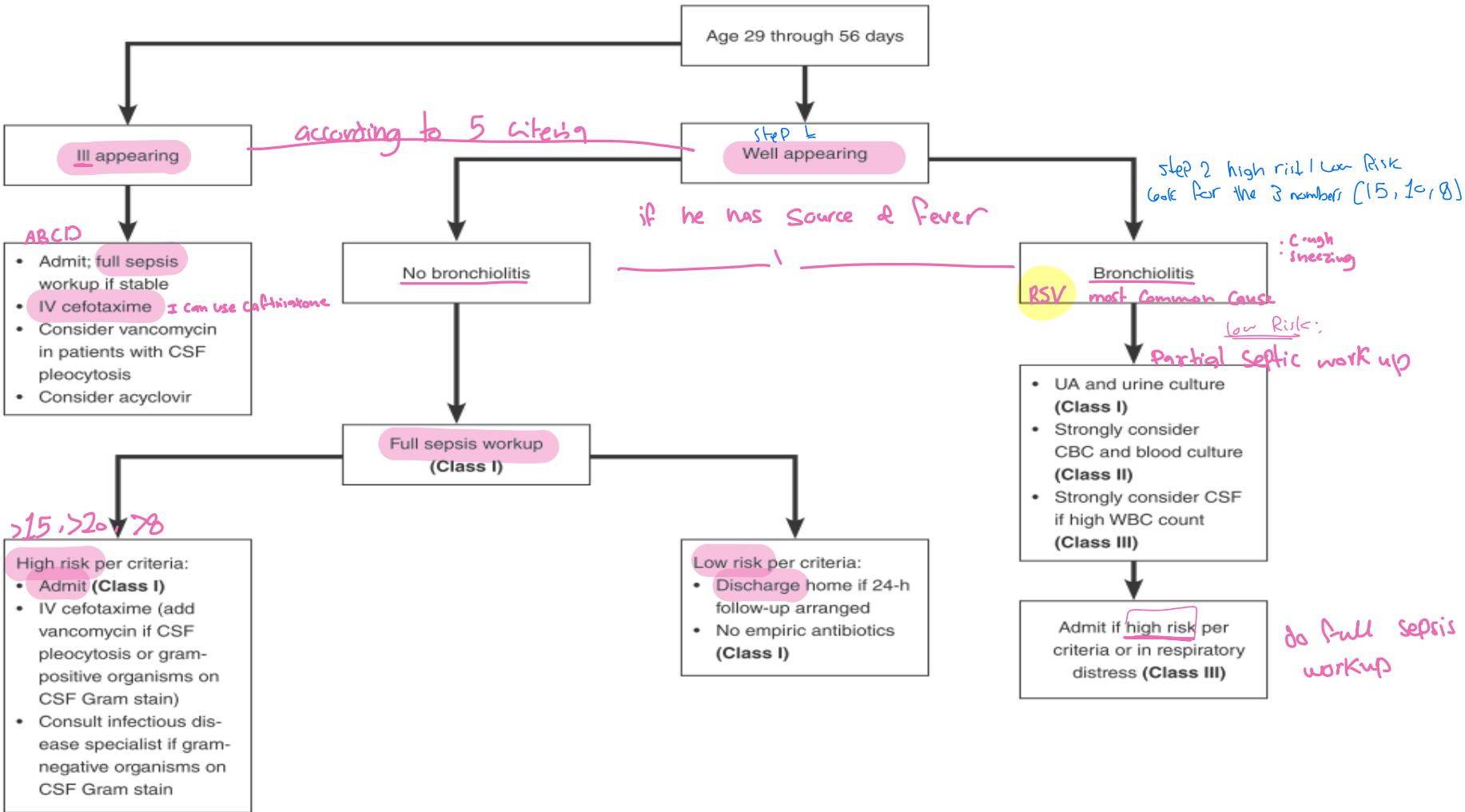
Young infants 1-2 months
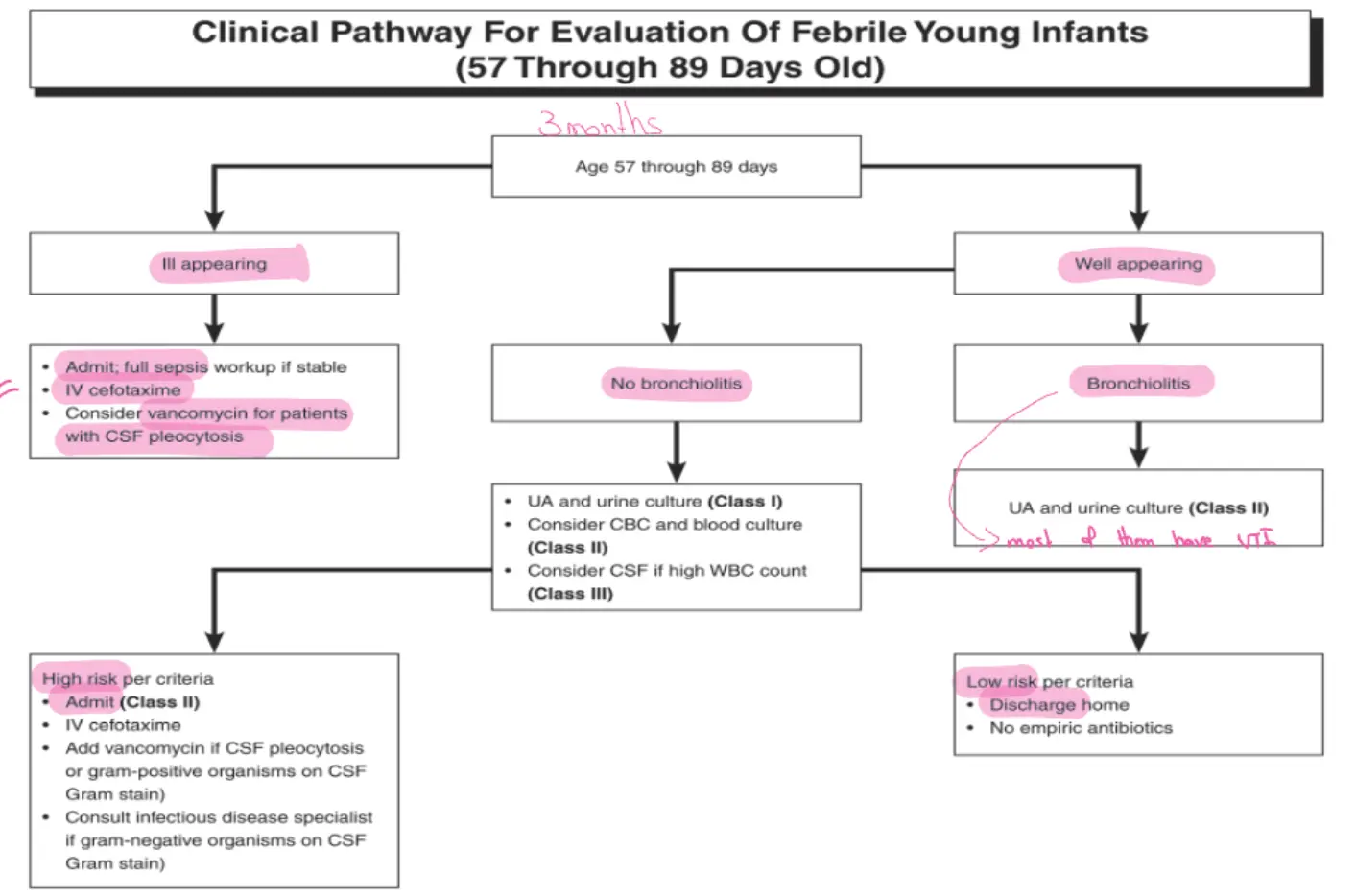
Clinical Pathway For Evaluation Of Febrile Young Infants (57 Through 89 Days Old) 2-3 m
Laboratory & Diagnostic Studies
Which one better?
Can we really exclude SBI?
- Blood culture
- Complete blood count with differential (CBCD)
- IT Ratio (immature-to-total neutrophil)
- UA & Urine culture
- LP – CSF analysis
- CXR
- Stool
- CRP
- ESR
- Procalcitonin