GASTROENTERITIS
Dr Tariq Al thobaiti ,MBBS
-
Diarrheal diseases are the second leading cause of death worldwide in children.
-
Rotavirus is the most common pathogen in areas without a vaccination program.
-
in areas with widespread rotavirus vaccination, norovirus is the most common pathogen.
CLINICAL FEATURES
-
Diarrhea associated with acute viral gastroenteritis typically lasts <7 days and not longer than 14 days, and it may be accompanied by vomiting or fever.
-
Isolated vomiting should not be diagnosed as acute gastroenteritis.
-
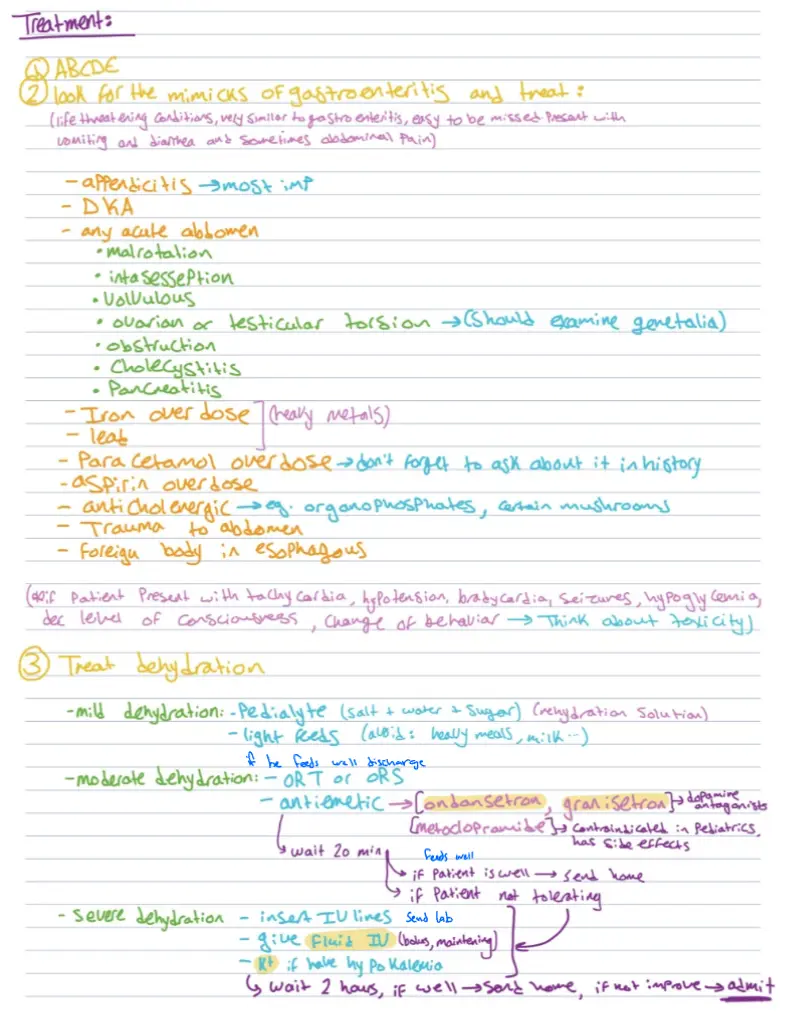
Although appendicitis typically manifests with abdominal pain followed by vomiting associated with constipation,
-
it may also cause diarrhea, particularly once the appendix has perforated. This is presumed to occur because the inflammation irritates the colon, resulting in diarrhea
LABORATORY TESTING
- Obtain a CBC only if the child is ill appearing or has bloody diarrhea.
- (mainly to identify bacterial enterocolitis or hemolytic-uremic syndrome).
- The WBC count and C-reactive protein are not reliable for distinguishing viral from bacterial gastroenteritis.
hypoglycemia, hypokalemia, acidosis, leukocytosis
LABORATORY TESTING
-
Given that the reported prevalence of hypoglycemia may be as high as 9% in pediatric gastroenteritis.
-
measuring serum glucose in infants and young children is essential.
-
Obtain serum electrolytes only in specific circumstances.
LABORATORY TESTING
- BUN is elevated in severe dehydration.
- it does not identify lesser degrees of dehydration very well.
- Serum bicarbonate>15 mEq/L makes dehydration unlikely.
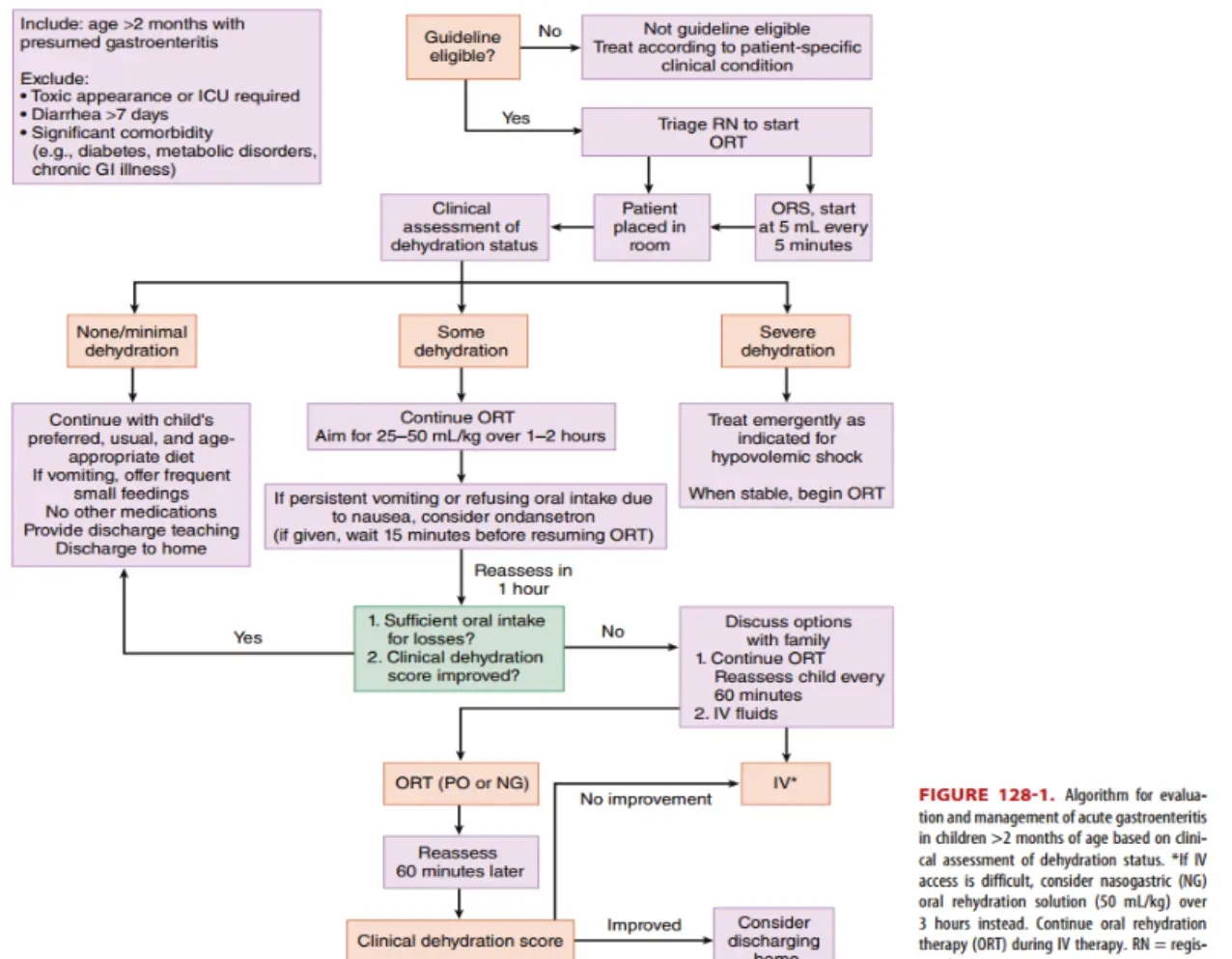
TABLE 129-2 Clinical Guidelines for Assessing Dehydration in Children
| None to Minimal Dehydration ( loss of body weight) | Some (mild to moderate) Dehydration ( to loss of body weight) | Severe Dehydration ( loss of body weight) | |
|---|---|---|---|
| Mental status | Well, alert | Fatigued, restless, irritable | Apathetic, lethargic, unconscious |
| Thirst | Normal, slight increase, or refusing fluids | Increased, eager to drink | Very thirsty or too lethargic to indicate |
| Heart rate | Normal | Normal to increased | Tachycardic with brady- cardia in severe cases |
| Blood pressure | Normal | Normal | Normal to reduced |
| Pulse quality | Normal | Normal to reduced | Weak, thready |
| Breathing | Normal | Normal to tachypneic | Deep |
| Eyes | Normal | Slightly sunken orbits | Deeply sunken orbits |
| Tears | Present | Decreased | Absent |
| Mucous membranes | Moist | Dry | Parched |
| Anterior fontanelle | Normal | Sunken | Sunken |
| Skin turgor | Instant recoil | Recoil in s | Recoil in s |
| Capillary refill | Normal | Prolonged 1–2 s | Prolonged s |
| Extremities | Warm | Cool | Cold, mottled, cyanotic |
| Urine output | Normal to decreased | Decreased ( mL/ kg/h) | Minimal ( mL/ kg/h) |
| Organism | Typical Clinical Features | Risk Factors | Complications | Antimicrobial Therapy |
|---|---|---|---|---|
| Shigella | Ranges from watery stools without constitutional symptoms to fever, abdominal pain, tenesmus, mucoid stools, hematochezia; Shigella dysenteriae serotype 1 causes more severe symptoms | Contact with infected host or fomite, poor sanitation, crowded living conditions, day care | Pseudomembranous colitis, toxic megacolon, intestinal perforation, bacteremia, Reiter’s syndrome, hemolytic-uremic syndrome, encephalopathy, seizures, hemolysis | Typically self-limited Treat if: immunocompromised, severe disease, dysentery or systemic symptoms If susceptibility unknown: azithromycin, ceftriaxone, ciprofloxacin; if susceptible, ampicillin or trimethoprim-sulfamethoxazole |
| Salmonella | Nontyphoidal: May be asymptomatic or cause watery diarrhea, mild fever, abdominal cramps Enterica serotypes: “enteric fever” may include high fever, constitutional symptoms, headache, abdominal pain, dactylitis, hepatosplenomegaly, rose spots, altered mental status | Direct contact with animals: poultry, livestock, reptiles, pets; consuming food contaminated by human carrier: beef, poultry, eggs, dairy, water | Meningitis, brain abscess, osteomyelitis, bacteremia, dehydration, endocarditis, enteric (typhoid or paratyphoid) fever | Typically self-limited Treat if: <3 mo of age, hemoglobinopathy, immunodeficiency, chronic GI tract disease, malignancy, severe colitis, bacteremia, sepsis Options: ampicillin, amoxicillin, trimethoprim-sulfamethoxazole; if resistant, azithromycin, fluoroquinolone Invasive disease: cefotaxime, ceftriaxone |
| Campylobacter | Diarrhea, hematochezia, abdominal pain, fever, malaise | Contamination from poultry feces or undercooked poultry, untreated water, unpasteurized milk, pets (dogs, cats, hamsters, birds); person-to-person transmission possible | Acute: dehydration, bacteremia, focal infections, febrile seizures Convalescence: reactive arthritis, Reiter’s syndrome, erythema nodosum, acute idiopathic polyneuritis, Miller Fisher syndrome, myocarditis, pericarditis | Often self-limited; 20% have relapse or prolonged symptoms Treat if: moderate-severe symptoms, relapse, immunocompromised, day care and institutions Options: erythromycin, azithromycin, ciprofloxacin |
| Escherichia coli -Shiga toxin producing | Initially nonbloody diarrhea, often becoming bloody; severe abdominal pain | Food or water contaminated with human or cattle feces, undercooked beef, unpasteur- | Hemorrhagic colitis, hemolytic-uremic syndrome | None indicated; debated risk of increased incidence of hemolytic-uremic syndrome with treatment |
| Escherichia coli –Shiga toxin producing | Initially nonbloody diarrhea, often becoming bloody; severe abdominal pain | Food or water contaminated with human or cattle feces, undercooked beef, unpasteurized milk | Hemorrhagic colitis, hemolytic-uremic syndrome | None indicated; debated risk of increased incidence of hemolytic-uremic syndrome with treatment |
|---|---|---|---|---|
| E. coli –enteropathogenic | Severe watery diarrhea, usually children <2 years in resource-limited countries | Food or water contaminated with feces | Dehydration | Treat if severe Options: trimethoprim-sulfamethoxazole, azithromycin, ciprofloxacin |
| E. coli –enterotoxigenic | Moderate watery diarrhea, abdominal cramps; traveler’s diarrhea | Food or water contaminated with feces | Dehydration | Treat if severe Options: trimethoprim-sulfamethoxazole, azithromycin, ciprofloxacin |
| E. coli –enteroinvasive | Fever, bloody or nonbloody diarrhea, dysentery | Food or water contaminated with feces | Dehydration | Treat if severe Options: trimethoprim-sulfamethoxazole, azithromycin, ciprofloxacin |
| E. coli –enteroaggregative | Watery diarrhea, may be prolonged | Food or water contaminated with feces | Dehydration | Treat if severe Options: trimethoprim-sulfamethoxazole, azithromycin, ciprofloxacin |
| Yersinia | Bloody diarrhea with mucus, fever, abdominal pain; pseudoappendicitis syndrome: fever, right lower quadrant pain, leukocytosis; Yersinia pseudotuberculosis causes fever, scarlatiniform rash, abdominal pain | Contaminated food: improperly cooked pork, unpasteurized milk, untreated water; contact with animals (ungulates, rodents, rabbits, birds) | Acute: bacteremia, pharyngitis, meningitis, osteomyelitis, pyomyositis, conjunctivitis, pneumonia, empyema, endocarditis, acute peritonitis, liver/spleen abscess; convalescence: erythema nodosum, glomerulonephritis, reactive arthritis | Typically self-limited; if severe, treat with trimethoprim-sulfamethoxazole, aminoglycosides, cefotaxime, fluoroquinolones, tetracycline, doxycycline, chloramphenicol |
| Vibrio cholerae | Voluminous watery diarrhea, usually without cramps or fever, classically described as “rice water” stools | Travel to affected areas, consumption of contaminated water or food (particularly undercooked seafood) | May rapidly lead to hypovolemic shock, hypoglycemia, hypokalemia, metabolic acidosis, seizures | Treat if moderate or severe: azithromycin, doxycycline; ciprofloxacin or trimethoprim-sulfamethoxazole if resistant |
By lina serhan