Mohammed Alageel
Headache
Goals
- Describe the categorization of headaches
- Describe characteristics and disease burden of each type
- Emphasize the importance of screening for secondary causes of headaches
- Overview of most common primary headache types regarding causes, triggers and treatment
Burden of disease
- 3 million visits to the emergency department (ED) per year in the United States.
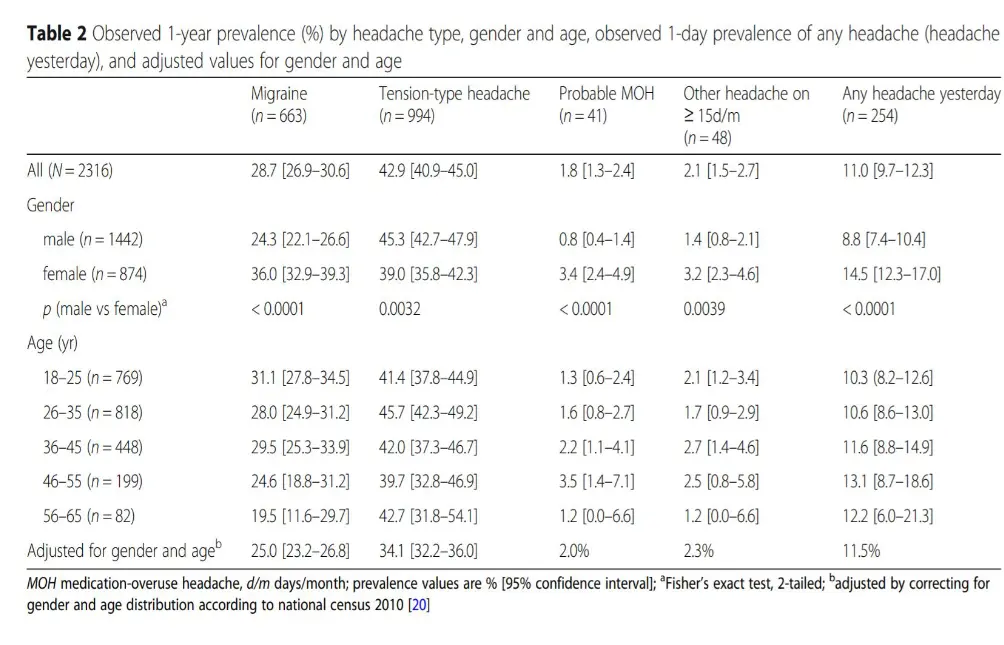
Saudi prevalence
Introduction
- Headache also known as cephalalgia, is the symptom of pain anywhere in the region of the head or upper neck
- Headache is among the most common pain problems encountered in primary practice.
- The brain itself is not sensitive to pain, because it lacks pain receptors. The pain originates from the tissues and structures that surround the skull or the brain.
- These include the extracranial and intracranial arteries, sinuses, cranial nerves and spinal the meninges, the eyes ears teeth and lining of the mouth
Classification
1- Primary headaches (benign, recurrent, not caused underlying disease or structural problems). So not dangerous
get better with time
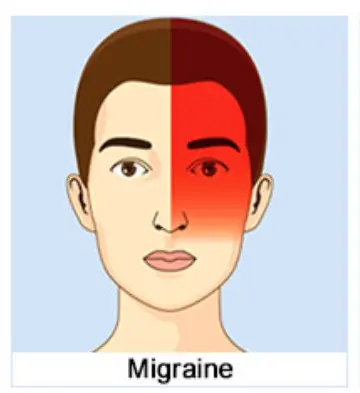
- Migraine
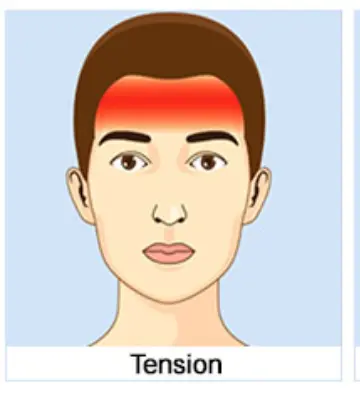
- Tension-type headache (most common) → Muscle contraction - vasodilation
- Cluster headache
2- Secondary headaches ( caused by underlying organic diseases or following an injury) suggest
this what will kill you “Dangerous”
3- cranial neuralgias, facial pain, and other headaches. abnormal signals
Primary headache
- 90% of all headaches are primary headaches
- Peak age between 20 and 40 years old
- The most common types of primary headaches are migraines, tension-type headaches and cluster headaches
Other less common types of primary headaches include—
-
Hemicrania continua: continuous unilateral pain with episodes of severe pain and a/w autonomic symptoms. It can be relieved by the medication indomethacin.
-
Primary sex headache: dull, bilateral headache that starts during sexual activity and becomes much worse during orgasm. Treated by advising the person to abstain. Medications such as propranolol and diltiazem can also be helpful
-
Primary thunderclap headache: Sudden onset of severe headache may occur in the absence of any known provocation—requires dangerous diagnoses to be ruled out includes SAH, sentinel bleed of an intracranial aneurysm, cervicocephalic arterial dissection and cerebral venous thrombosis
-
Hypnic headache: moderate-severe headache that starts a few hours after falling asleep and lasts 15–30 minutes. The headache may recur several times during night. Hypnic headaches are usually in older women. They may be treated with lithium.
-
Primary stabbing headache: recurrent episodes of stabbing “ice pick pain” or “jabs and jolts” for 1 second to several minutes without autonomic symptoms (tearing, red eye, nasal congestion). These headaches can be treated with indomethacin.
-
Primary cough headache: generalized, starts suddenly and lasts for several minutes after coughing, sneezing or straining –Rx- indomethacin
-
Primary exertional headache: B/L, throbbing, pulsatile pain which starts during or after exercising, lasting for 5 minutes to 24 hours. It can be treated with medications such as indomethacin
-
New daily-persistent headache (NDPH) -Headache that is daily and unremitting from very soon after onset (within 3 days at most). Headache is present daily, and is unremitting, for > 3 months
-The pain is typically bilateral, pressing or tightening in quality and of mild to moderate intensity. There may be photophobia, phonophobia or mild nausea.
Secondary headache
Secondary headaches are those due to an underlying organic cause or occur following a trauma
1- headaches associated with head trauma
2- Headaches associated with vascular disorders
•SAH
- Acute ischemic cerebrovascular disorder
- Unruptured vascular malformation
- Arteritis (e.g. temporal arteritis)
- Arterial HTN → this is contraversial ‘headach it self increase the BP’ and most of HTN fit are asymptomatic so we don’t know the headach because of high BP or the opposite
3- headache associated with nonvascular intracranial disorder
- benign intra cranial HTN (pseudotumor cerebri) –intracranial infection
- Low CSF pressure (post LP, spontaneous)
4-Headache associated with substance abuse or
-
even because of caffeine
-
withdrawal, excess use of medications used to treat headache (rebound headache)
5-Headache associated with noncephalic infection
- (viral infection, bacterial infection)
6-Headache associated with metabolic disorder
- (hypoxia, hypercapnia, hypoglycemia, dialysis)
7-Headache or facial pain
-
associated with disorder of cranium, neck, eyes, ears, nose, sinuses, teeth or mouth
-
—cervicogenic headache
8-Headache attributed to psychiatric disorder
- Anxiety
cranial neuralgias, facial pain, and other types
- Cranial neuralgia describes inflammation of one of the 12 cranial nerves coming from the brain that control the muscles and carry sensory signals (such as pain) to and from the head and neck.
- most common example is trigeminal neuralgia, which affects cranial nerve V (the trigeminal nerve), the sensory nerve that supplies the face and can cause intense facial pain when irritated or inflamed
Approach to headache
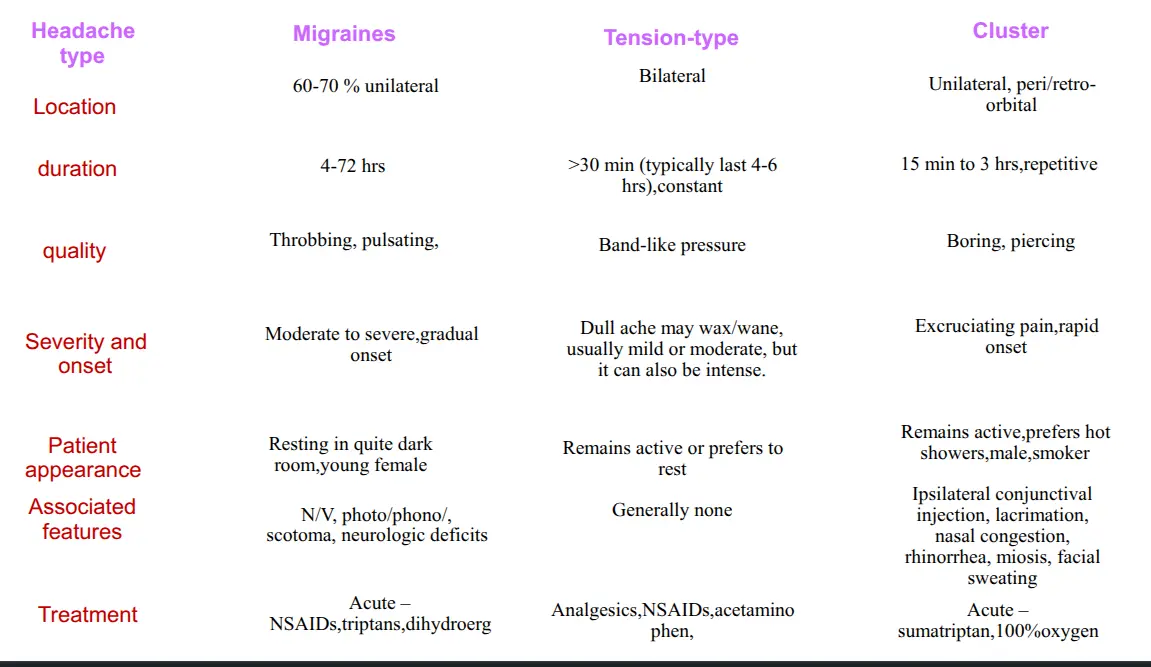
Migraine
Tension Headache
Cluster Headache
Headache type
Pearls
- The most reassuring fact is chronicity of symptoms
- Patients being assessed for headaches whether new or old need to be questioned regarding red fags
- Rapidly progressive headaches always warrants a thorough assessment
- Cluster headaches are always associated with autonomic dysfunction
- Patients with migraine headaches should be asked to keep migraine diaries to help identify triggers to help avoid them