Mohammed Alageel
Goals
-
Discuss the definition and burden of disease
-
Brief overview of the pathophysiology of heart failure
-
Review the diagnostic and therapeutic approach to heart failure
-
Review evidence‑based algorithm in the treatment of acute heart failure
Definition
-
Heart failure may be defined as the pathophysiologic state in which the heart is incapable of pumping a sufficient supply of blood to meet the metabolic requirements of the body or requires elevated ventricular filling pressures to accomplish this goal.
-
It is an “AHA” complex syndrome that results from a structural or functional cardiac disorder that impairs the ability of ventricles to fill or eject blood.
Burden of Disease
- Incidence of HF approaches 10 per 1 000 population after age 65.
- 1–2 % at age 45‑50 years.
- >10 % at age > 75 years.
- At age 40 years, lifetime risk for HF is 21 % for men and 20.3 % for women.
- 80 % of admissions for HF occur in people > 65 years.
- HF carries approximately 50 % mortality at 5 years after symptom onset; one‑third of patients with the most severe disease die within the first year after diagnosis.
Cost of hospitalization for heart failure is twice that for all forms of cancer and myocardial infarction combined (USA data).
NYHA Classification
Class I – No limitation of physical activity. Ordinary activity does not cause undue fatigue, palpitation, or dyspnoea.
Class II – Slight limitation of physical activity. Comfortable at rest but ordinary activity results in fatigue, palpitation, or dyspnoea.
Class III – Marked limitation of physical activity. Comfortable at rest but less than ordinary activity results in fatigue, palpitation, or dyspnoea.
Class IV – Unable to carry out any physical activity without discomfort. Symptoms at rest; any activity increases discomfort.
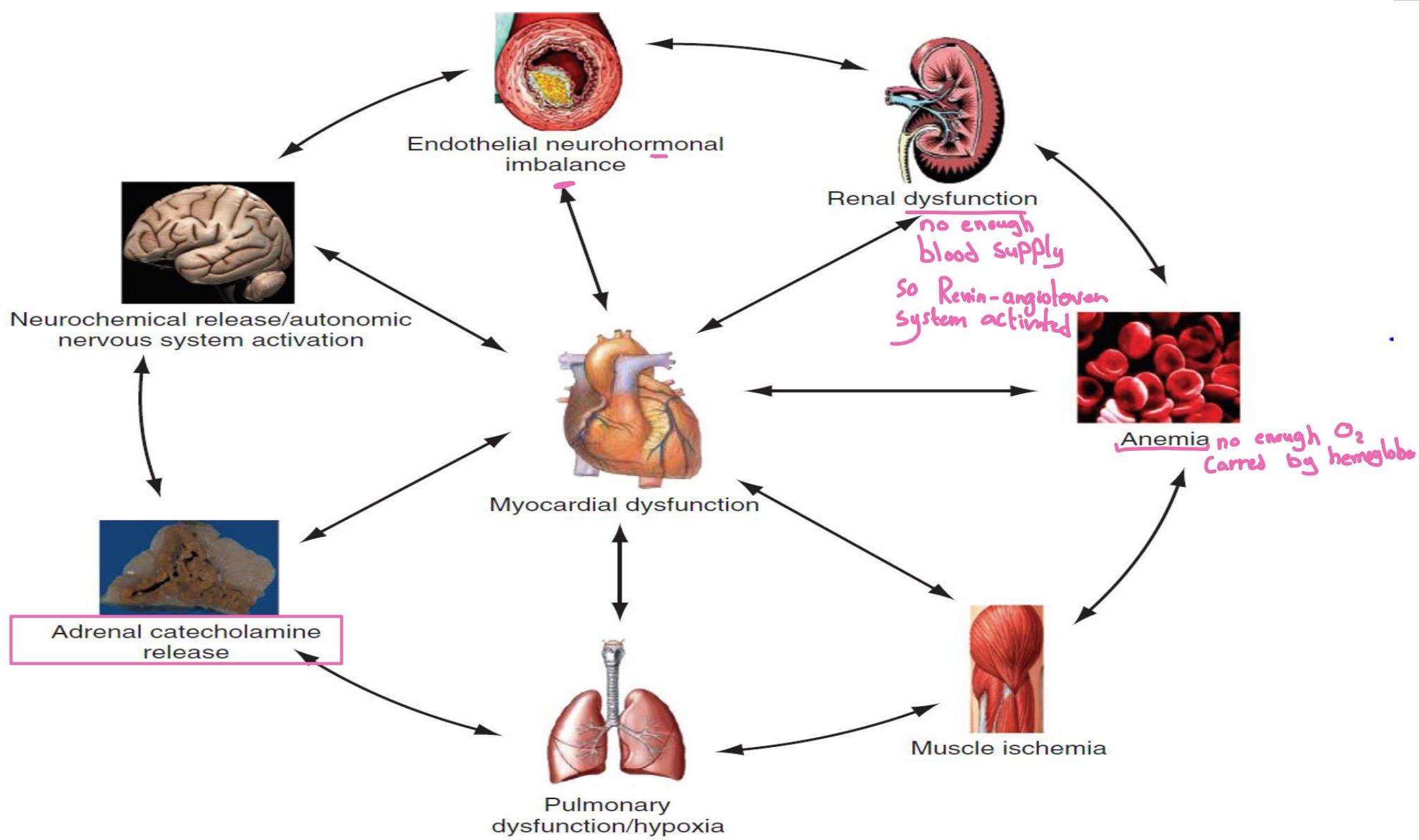
Pathophysiology
- Dysfunction of the heart or any component of the cardiopulmonary system initiates adaptive neurohormonal activation (sympathetic nervous system, RAAS, natriuretic peptides, endothelin, vasopressin, etc.) → ↑BP, ↑fluid retention.
- Feedback loops mediated through vasoactive substances secreted by the heart, autonomic nervous system, kidneys, adrenals, lungs, and vascular endothelium are crucial; perturbations in any organ affect the others.
Causes of Heart Failure
Coronary Artery Disease
- In developed countries, atherosclerotic coronary artery disease remains the leading cause of HF, present in almost 70 % of patients in multicenter HF trials.
- Chronic coronary insufficiency leads to diffuse myocardial fibrosis termed ischemic cardiomyopathy.
Cardiomyopathy and Myocarditis
- Mostly idiopathic forms—dilated, hypertrophic, or restrictive—often related to substance use.
Valvular Heart Disease
- The third leading cause of HF after ischemic heart disease and dilated cardiomyopathy.
Pericardial Diseases
- Significantly affect ventricular function, decreasing CO and increasing intracardiac pressures.
Pulmonary Disease
- COPD prevalence is 20–30 % in HF; it may obscure HF recognition.
- Natriuretic peptide (BNP) levels are only slightly elevated in primary pulmonary disease compared with much higher levels in LV failure.
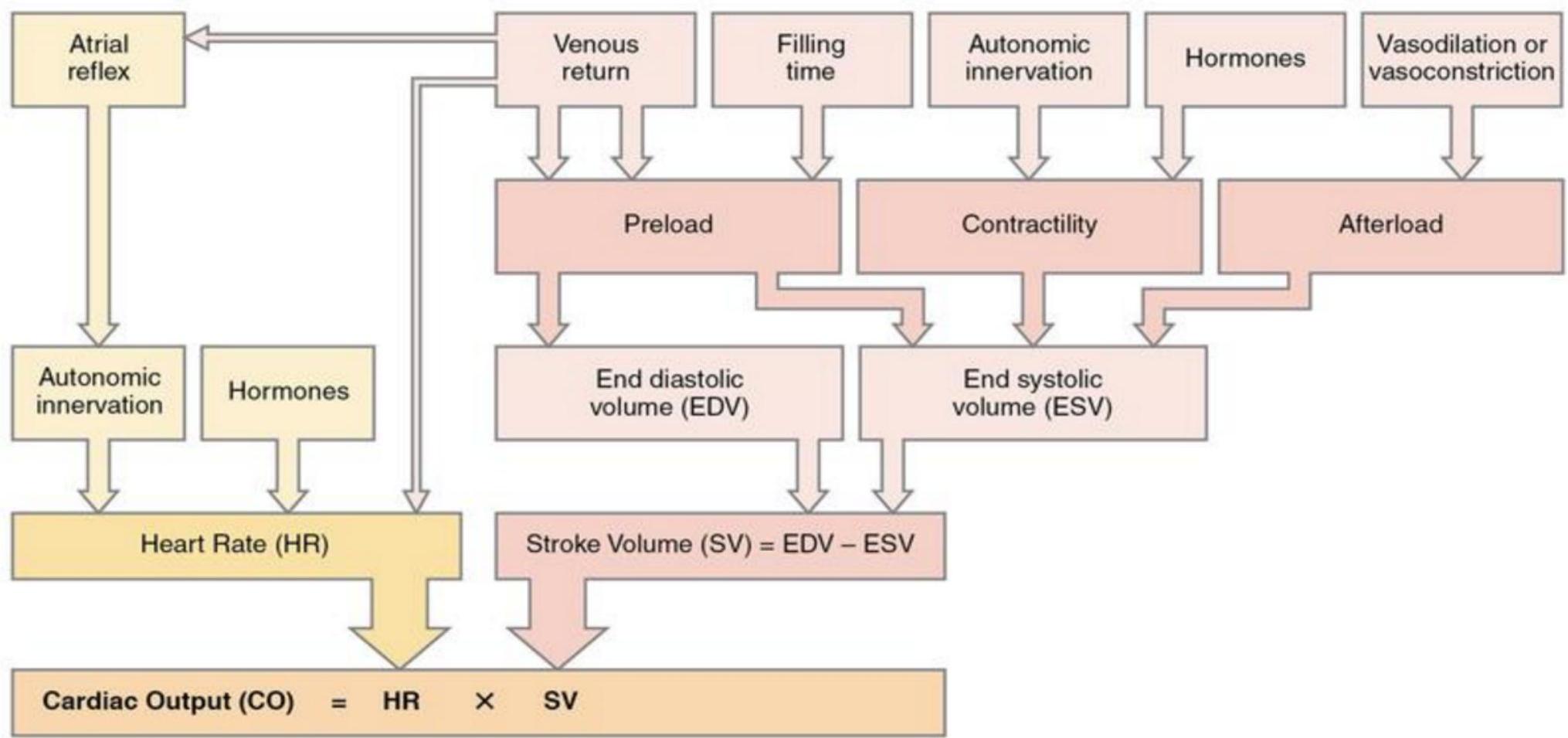
Factors Affecting Heart Rate (HR) and Stroke Volume (SV)
Physiologic Mechanisms for Compensation
-
Increase in stroke volume → more blood ejected.
-
Increased systemic vascular resistance → systemic hypertension.
-
Development of cardiac hypertrophy.
Classification
-
Multiple: Forward vs. backward; right‑ vs. left‑sided HF; acute vs. chronic; low vs. high output.
-
Systolic (HFrEF) vs. Diastolic (HFpEF) – About 50 % of patients with congestive symptoms have normal EFs and experience diastolic dysfunction.
Precipitating Causes & Exacerbating Factors
-
Sodium and volume excess
-
Systemic hypertension
-
Myocardial infarction or ischemia (stop the drugs)
-
Systemic infection
-
Dysrhythmias
-
Acute hypoxia or respiratory problems
-
Anemia
-
Pregnancy
-
Thyroid disorders
-
Acute myocarditis
-
Acute valvular dysfunction
-
Pulmonary embolus
-
Excess exertion or trauma
-
Pharmacologic complications
Assessment
History
- Chronic symptoms; inquire about dyspnoea, chest pain, prior heart disease, cardiac catheterization, surgery, current medications (and adherence), and possible intercurrent illness.
- Paroxysmal nocturnal dyspnoea, orthopnoea, lower‑limb oedema, exertional wheezing.
Physical Examination
- Hypertension often indicates a better prognostic sign; clammy, hypoperfused patients may have low EF HF.
- Wheezing or crackles are common.
- Jugular venous distention in ~50 % of cases; peripheral edema in one‑third.
- An S3 gallop may be present in up to 25 %.
Ultrasound Findings
-
LT side → Pulmonary edema (side‑specific)
-
Right‑side → lower‑limb edema - Elevated JVP
Laboratory and Imaging Testing
- Chest radiograph – helps distinguish cardiogenic pulmonary edema from other causes of dyspnea. An enlarged cardiac silhouette is seen in 70% of cases
- CBC – anemia detection.
- Basic metabolic panel – renal function.
- Cardiac biomarkers – detect ischemia.
- BNP – levels > 500 pg/mL highly associated with HF progression.
ECG Diagnostic
-
Arrhythmia recognition and management; identification of acute coronary syndrome.
Treatment
Goals
- Determine underlying cardiac pathology (baseline dysfunction).
- Identify the acute precipitant.
- Mitigate the acute decompensation.
Two Types of Acute Heart Failure
- Well‑perfused with normal or high BP.
- Poorly perfused with low BP.
Acute Heart Failure Management
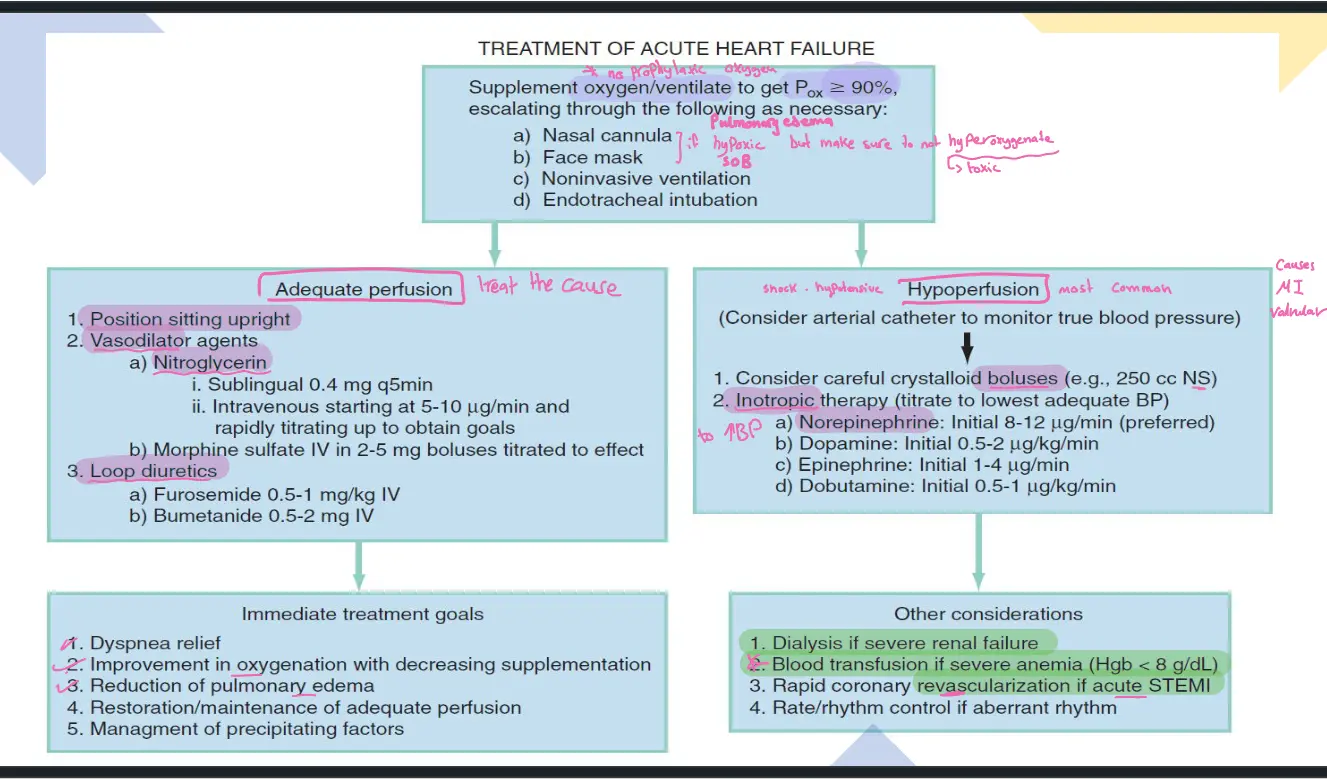
- Oxygen/ventilation to keep (nasal cannula → face mask → non‑invasive ventilation → endotracheal intubation).
Adequate Perfusion
-
Position patient upright.
-
Vasodilator agents
- Nitroglycerin – sublingual 0.4 mg q5 min; IV start 5–10 µg/min, titrate to goal.
- Morphine sulfate IV 2–5 mg boluses titrated to effect.
-
Loop diuretics
- Furosemide 0.5–1 mg/kg IV
- Bumetanide 0.5–2 mg IV
Immediate Treatment Goals
- Relief of dyspnoea
- Improvement in oxygenation with decreasing supplemental O₂
- Reduction of pulmonary edema
- Restoration/maintenance of adequate perfusion
- Management of precipitating factors
Hypoperfusion (consider arterial catheter)
- Careful crystalloid boluses (e.g., 250 mL NS).
- Inotropic therapy (titrate to lowest adequate BP)
- Norepinephrine – initial 8–12 µg/min (preferred)
- Dopamine – initial 0.5–2 µg/kg/min
- Epinephrine – initial 1–4 µg/min
- Dobutamine – initial 0.5–1 µg/kg/min
Other Considerations
- Dialysis if severe renal failure.
- Blood transfusion if severe anemia (Hgb < 8 g/dL).
- Rapid coronary revascularization if acute STEMI.
- Rate/rhythm control for aberrant rhythms.
Pearls
- Neurohormonal mechanisms provide initial compensation but become deleterious; chronic therapy to block these effects is vital, even in asymptomatic myocardial dysfunction.
- Identifying a precipitating cause is key in treatment.
- Most acute HF can be managed with upright positioning, supplemental oxygen, vasodilators, and loop diuretics.
- In hypoperfusing patients who are adequately volume‑repleted (true cardiogenic shock), norepinephrine is the pressor of choice.