Low Back Pain: Approach To The Patient In The E.D.
Bader Alyahya, MD, FRCPC (EM, CPT), ABEM
ER Consultant
Epidemiology
- 2.3% of all physician visits
- 84% of the adult population have experienced low back pain in their lifetime
- Costs $100 billion per year in the US
- 95% of clinically significant herniation occur at the L4-5 and L5-S1, causing radicular pain in the L5 and S1 dermatomes
Reference: Rosen’s 8th edition
© Mayfield Clinic
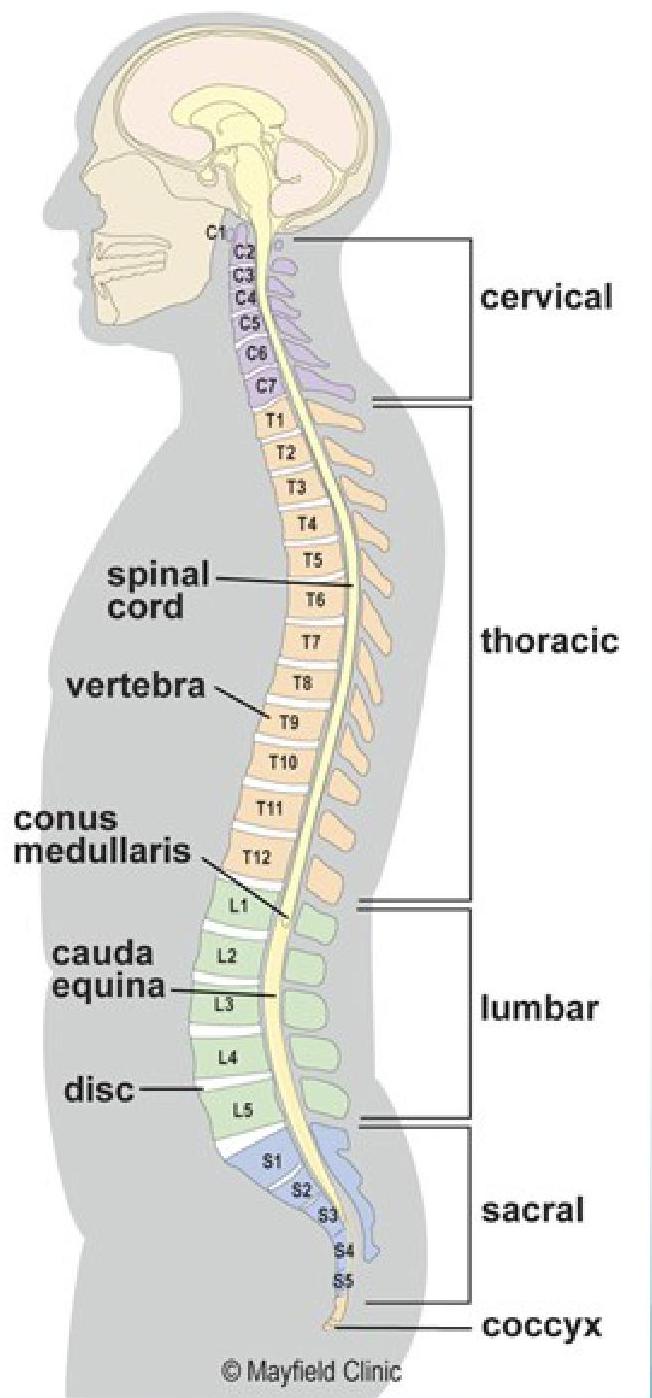
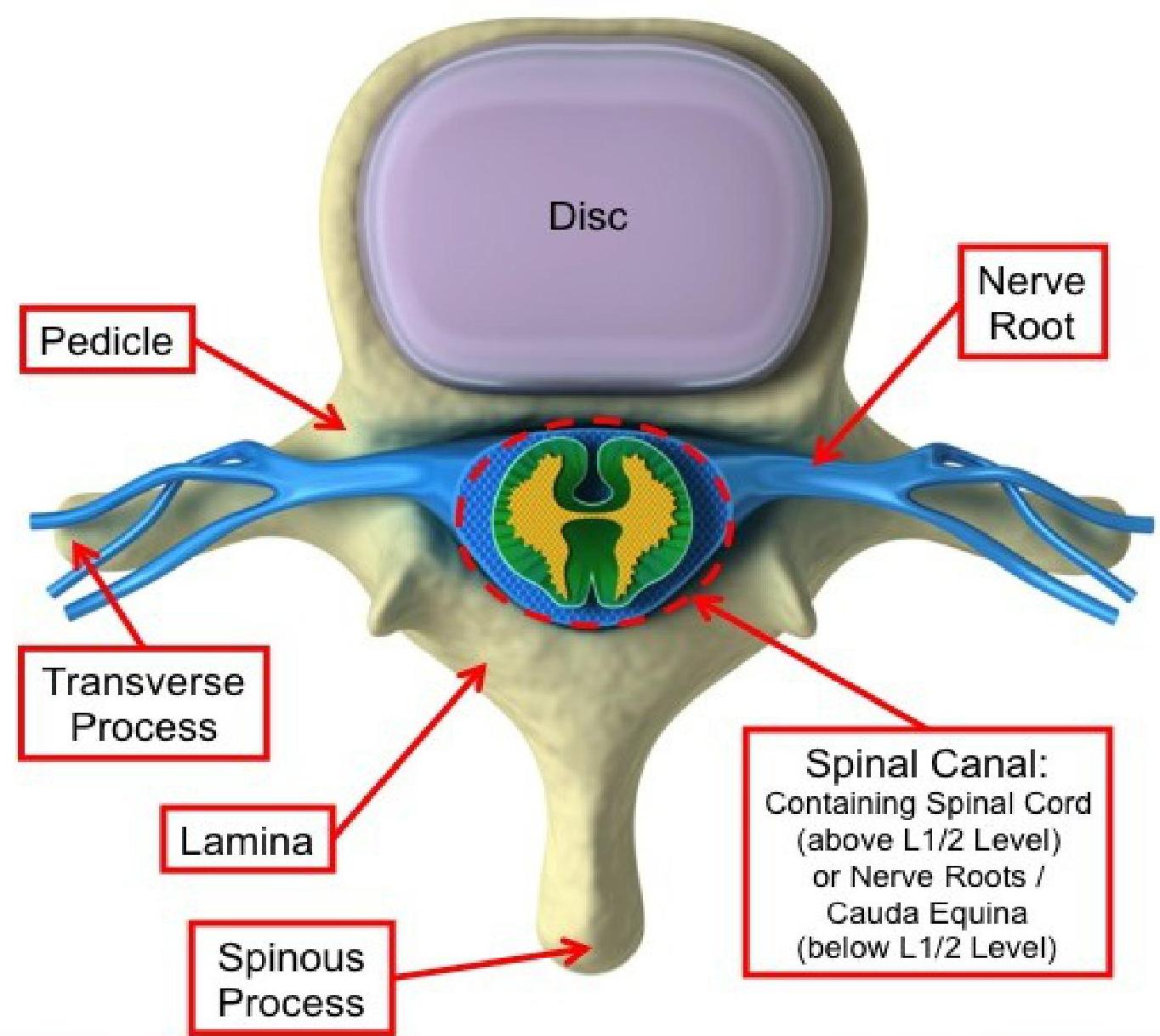
Anatomy and Terminology
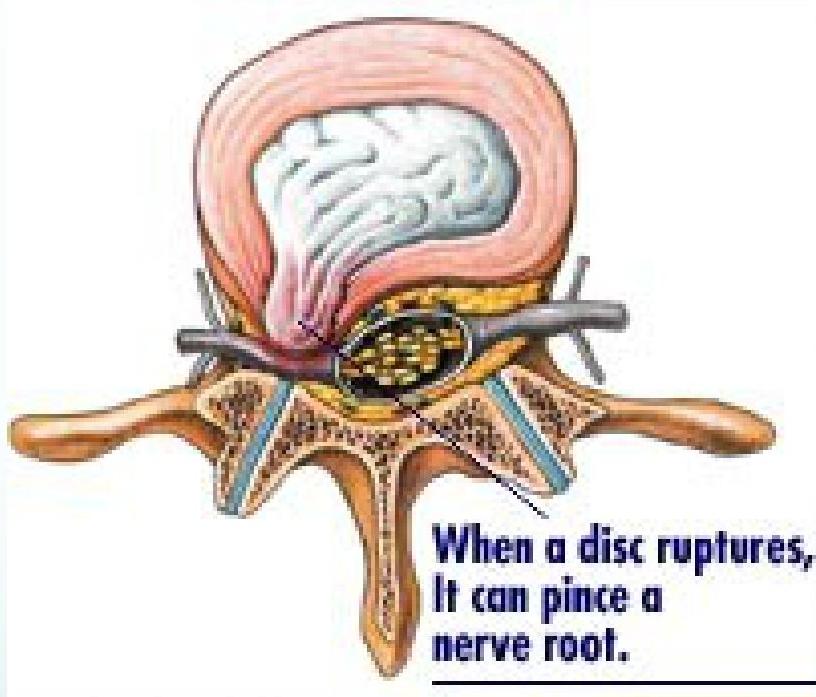
The Normal Spine in Cross Section
Terminology Used in Back Pain
Spondylosis
Arthritis of the spine. Seen radiographically as disc space narrowing and arthritic changes of the facet joint.
Spondylolisthesis
Anterior displacement of a vertebra on the one beneath it. A radiologist determines the degree of slippage upon reviewing spinal radiographs. Slippage is graded I through IV:
- Grade I: 1 to 25% slip
- Grade II: 26 to 50% slip
- Grade III: 51 to 75% slip
- Grade IV: 76 to 100% slip
Generally, Grade I and Grade II slips do not require surgical treatment and are treated medically. However, Grade III and Grade IV slips, and some milder grade slips, may benefit from surgery if persistent and disabling symptoms are present.
Spondylolysis
A fracture in the pars interarticularis where the vertebral body and the posterior elements protecting the nerves are joined. In a small percent of the adult population, there is a developmental crack in one of the vertebrae, usually at L5.
Spinal Stenosis
Local, segmental, or generalized narrowing of the central spinal canal by bone or soft tissue elements, usually bony hypertrophic changes in the facet joints and by thickening of the ligamentum flavum.
Radiculopathy
Impairment of a nerve root, usually causing radiating pain, numbness, tingling, or muscle weakness that corresponds to a specific nerve root.
Sciatica
Pain, numbness, tingling in the distribution of the sciatic nerve, radiating down the posterior or lateral aspect of the leg, usually to the foot or ankle.
Cauda Equina Syndrome
Loss of bowel and bladder control and numbness in the groin and saddle area of the perineum, associated with weakness of the lower extremities. This condition can be caused by abnormal pressure on the bottom-most portion of the spinal canal and spinal nerve roots, related to either bony stenosis or a large herniated disc.
Lordosis, Kyphosis, Scoliosis
- Kyphotic curves refer to the outward curve of the thoracic spine (at the level of the ribs).
- Lordotic curves refer to the inward curve of the lumbar spine (just above the buttocks).
- Scoliotic curving is a sideways curvature of the spine and is always abnormal.
A small degree of both kyphotic and lordotic curvature is normal. Too much kyphotic curving causes round shoulders or hunched shoulders (Scheuermann’s disease). Too much lordotic curving is called swayback (lordosis). Lordosis tends to make the buttocks appear more prominent.
Reference: UpToDate
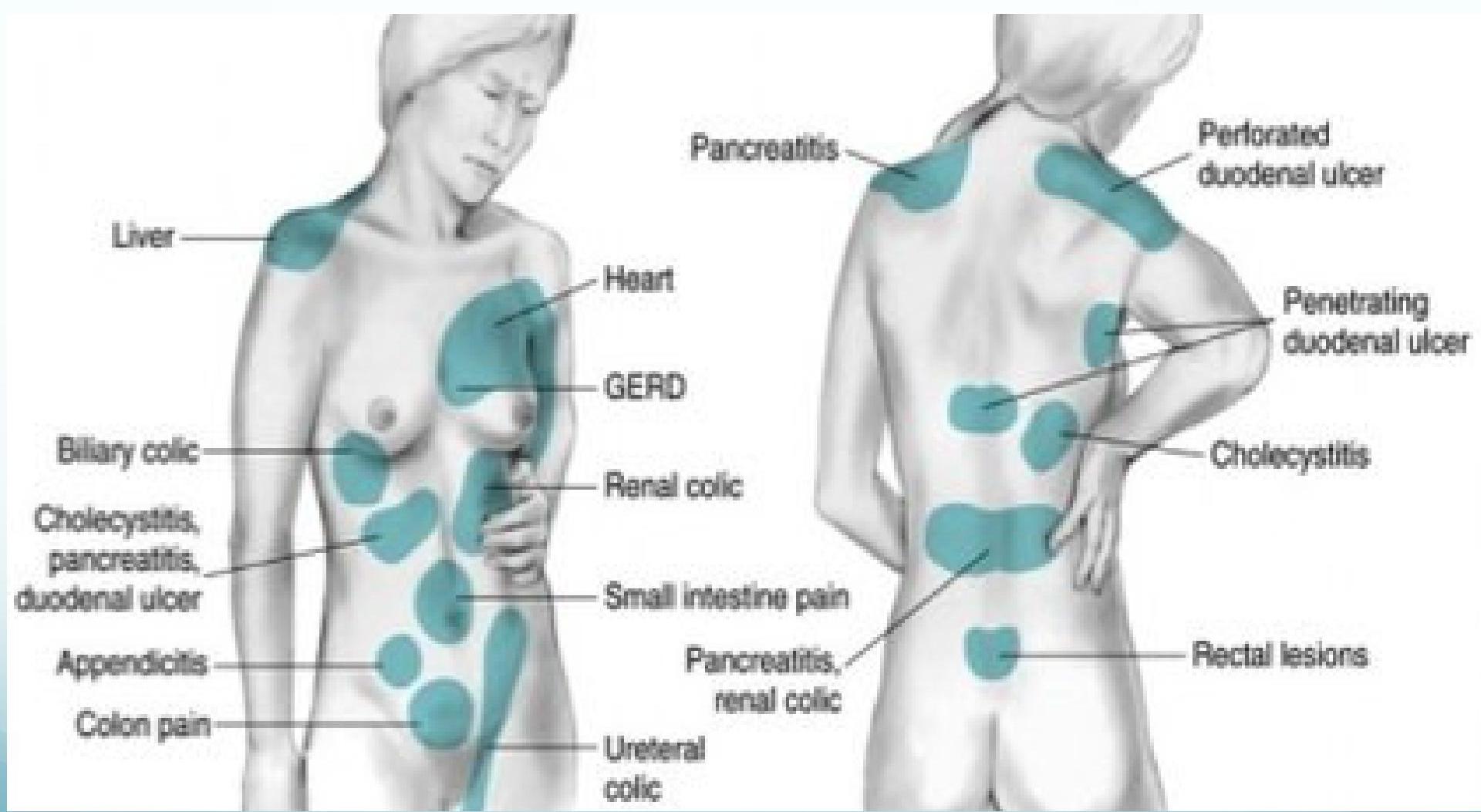
Differential Diagnosis
| Mechanical Low Back Pain | Nonmechanical Spine Disease | Visceral Disease |
|---|---|---|
| Lumbar strain | Neoplasia • Multiple myeloma • Metastatic carcinoma • Lymphoma and leukemia • Spinal cord tumors • Retroperitoneal tumors | Pelvic organs • Prostatitis • Endometriosis • Chronic pelvic inflammatory disease |
| Degenerative disease • Discs (spondylosis) • Facet joints (osteoarthritis) | Infection • Osteomyelitis • Septic discitis • Paraspinous abscess • Epidural abscess • Bacterial endocarditis | Renal disease • Nephrolithiasis • Pyelonephritis • Perinephric abscess |
| Spondylolisthesis | Inflammatory arthritis (often HLA-B27 associated) • Ankylosing spondylitis • Psoriatic spondylitis • Reiter syndrome • Inflammatory bowel disease | Aortic aneurysm |
| Herniated disc | Scheuermann disease (osteochondrosis) | Gastrointestinal disease • Pancreatitis • Cholecystitis • Penetrating ulcer |
| Spinal stenosis | Paget disease | Fat herniation of lumbar space |
| Osteoporosis | ||
| Fractures | ||
| Congenital disease • Severe kyphosis • Severe scoliosis • Possible type II or type IV transitional vertebrae | ||
| Possible spondylolysis | ||
| Possible facet joint asymmetry |
Red Flags

Clinical Clues (Table 1)
| Red Flags | Possible Cause |
|---|---|
| Duration > 6 wk | Tumor, infection, rheumatologic disorder |
| Age < 18 y | Congenital defect, tumor, infection, spondylolysis, spondylolisthesis |
| Age > 50 y | Tumor, intra-abdominal processes (such as an abdominal aortic aneurysm), infection |
| Major trauma, or minor trauma in elderly | Fracture |
| Cancer | Tumor |
| Fever, chills, night sweats | Tumor, infection |
| Weight loss | Tumor, infection |
| Injection drug use | Infection |
| Immunocompromised status | Infection |
| Recent genitourinary or gastrointestinal procedure | Infection |
| Night pain | Tumor, infection |
| Unremitting pain, even when supine | Tumor, infection, abdominal aortic aneurysm, nephrolithiasis |
| Pain worsened by coughing, sitting, or Valsalva maneuver | Herniated disc |
| Pain radiating below knee | Herniated disc or nerve root compression below the L3 nerve root |
| Incontinence | Cauda equina syndrome, spinal cord compression |
| Saddle anesthesia | Cauda equina syndrome, spinal cord compression |
| Severe or rapidly progressive neurologic deficit | Cauda equina syndrome, spinal cord compression |
Mnemonic: TUNA FISH
- T = Trauma
- U = Unexplained Weight Loss
- N = Neurologic Symptoms
- A = Age > 50
- F = Fever
- I = IVDU (Intravenous Drug Use)
- S = Steroid Use
- H = History of Cancer (Prostate, Renal, Breast, Lung)
Reference: www.rebelem.com
Imaging
- Plain Radiography: Limited to patients with:
- Findings suggestive of systemic disease
- Trauma
- CT and MRI: More sensitive for cancer and infections; also reveal herniation and stenosis.
- Recommendation: Reserve for suspected malignancy, infection, or persistent neurologic deficit.
MRI
- Shows tumors and soft tissues (e.g., herniated discs) much better than CT scan.
- Almost never an emergency.
- Exceptions:
- Cauda equina syndrome (acute neurologic deficit)
- Spinal epidural abscess
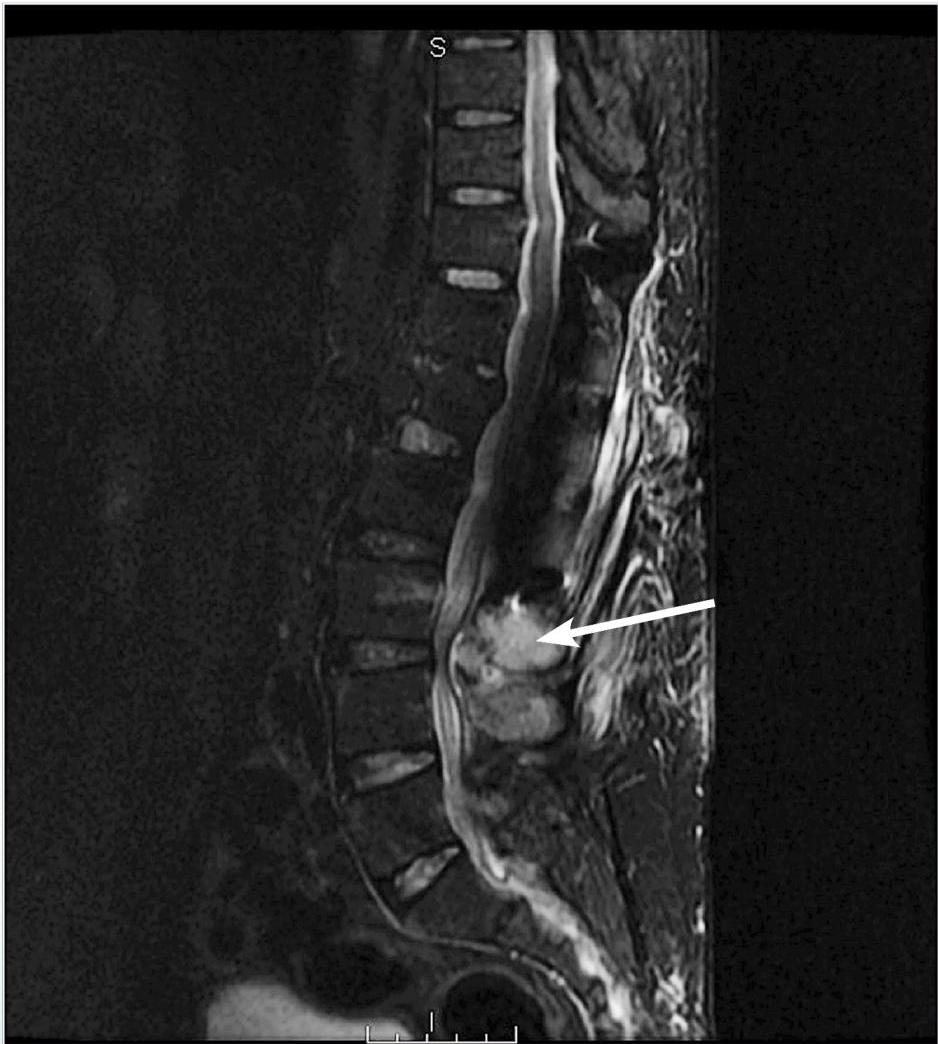
Figure 3. Osteomyelitis And Abscess
Magnetic resonance imaging reveals edema of paraspinal muscles and a fluid collection near L3-L4 with possible osteomyelitis (see arrow). The patient underwent interventional radiology abscess drainage that grew methicillin-sensitive Staphylococcus aureus. He was treated with 6 weeks of intravenous nafcillin.
Image courtesy of Pierre Borczuk, MD.

Figure 4. Posterior Disc Herniation
Magnetic resonance imaging (MRI) T2 sagittal images without contrast demonstrates a L5-S1 posterior disc herniation in a patient with back pain and sciatica symptoms. Since his symptoms had been ongoing for 3 months, were resistant to medical therapy, and had concordant MRI findings, he underwent epidural steroid injection treatment. The asterisk is over the L5 vertebral body; the arrow points to the herniated disc.
Image courtesy of Pierre Borczuk, MD.
CT Scan
- Shows bone (e.g., fractures) very well.
- Good in acute situations (trauma).
- Sagittal reconstruction is mandatory.
- Soft tissues (discs, spinal cord) are poorly visualized.
- CT-myelogram adds contrast in the CSF and shows the spinal cord and nerves contour better.
Clinical Assessment
Dermatomes and Myotomes

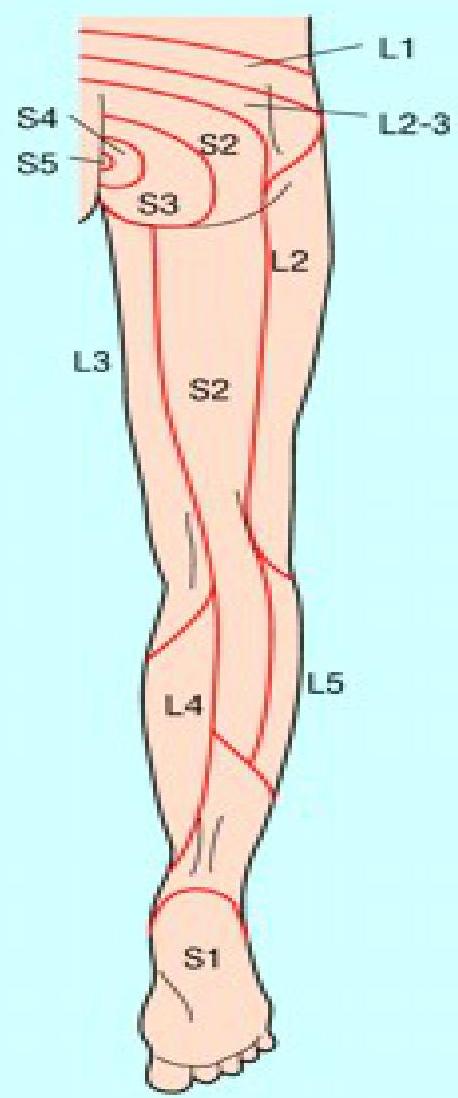
Table 4. Affected Nerve Roots And Their Corresponding Neurologic Examination Findings
| Affected Nerve Root | Reflex | Pain Distribution | Affected Motor Weakness | Affected Sensory Loss |
|---|---|---|---|---|
| L1 | Cremasteric | Inguinal | Hip flexion | Inguinal |
| L2 | Cremasteric, thigh adductor | Inguinal, anterior thigh | Hip flexion and adduction | Anterior thigh |
| L3 | Patellar | Anterior thigh, knee | Quadriceps adductors | Anterior, medial thigh |
| L4 | Patellar | Anterior thigh, medial leg | Knee extension, hip flexion | Anterior leg, first toe, medial malleolus |
| L5 | None | Posterolateral thigh, lateral leg | Great toe dorsiflexion | Dorsal foot, middle 3 toes |
| S1 | Achilles | Posterior thigh and leg, lateral foot | Plantar flexion | Lateral foot, heel |
Reference: July 2013 • www.ebmedicine.net
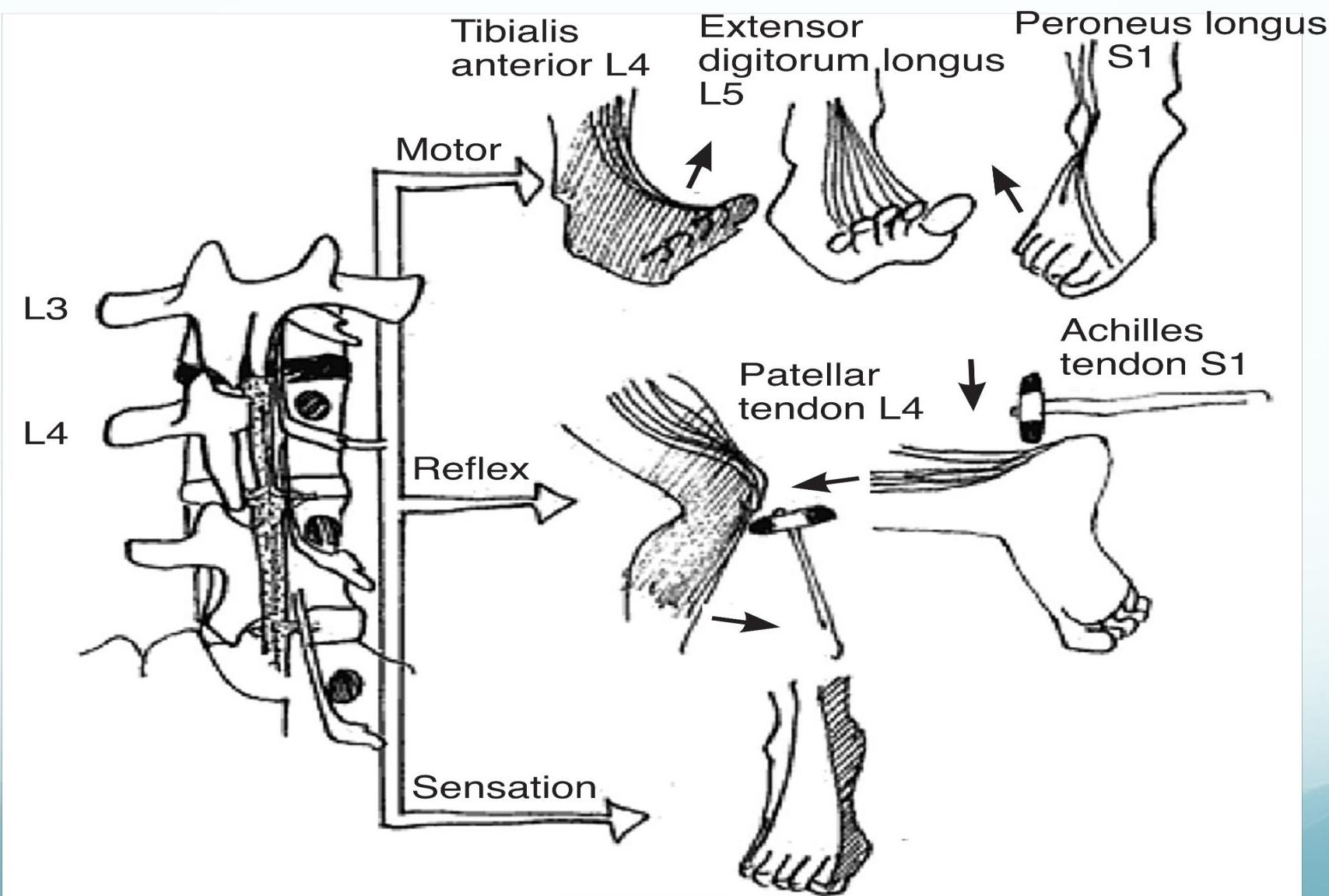
Figure 2. Summary Of Neurologic Examination At L4-S1 Levels
Image used with permission from the American Academy of Neurology.
Straight Leg Raise Test
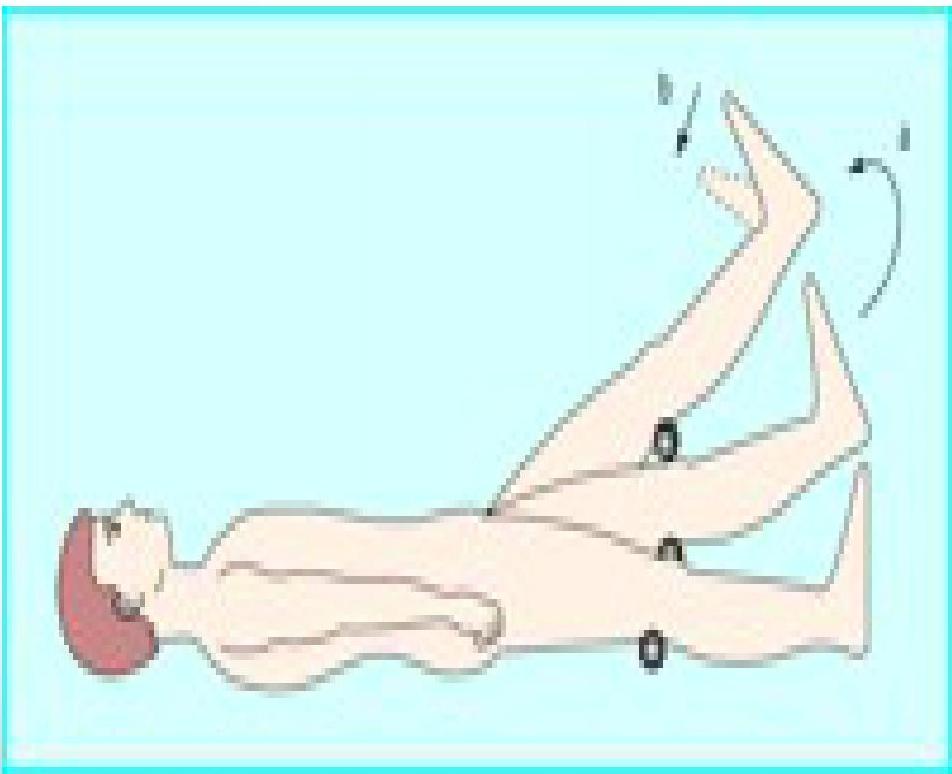
The straight leg raise test is positive if pain in the sciatic distribution is reproduced between 30° and 70° passive flexion of the straight leg. Dorsiflexion of the foot exacerbates the pain.
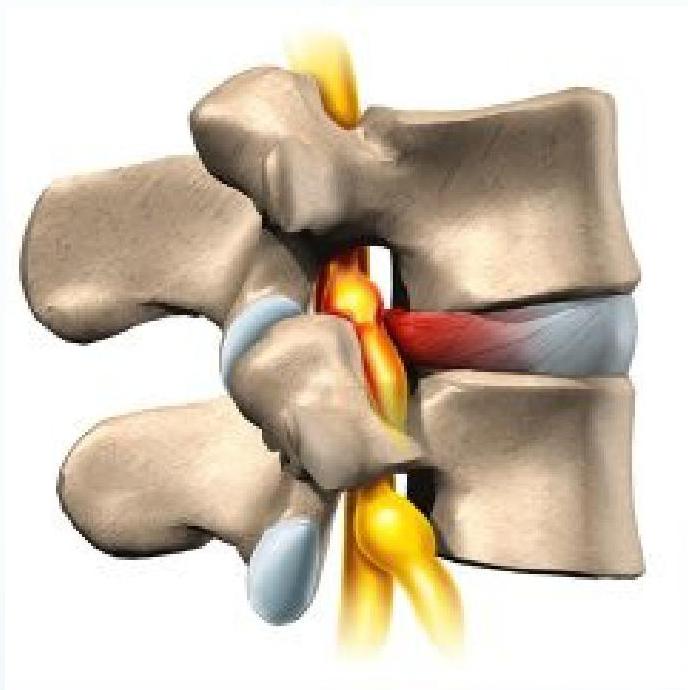
Pathophysiology: Disc Herniation
- Tears in the annulus
- Herniation of nucleus pulposus
- Compression of the nerve root in the foramen leads to pain
Algorithm and Summary
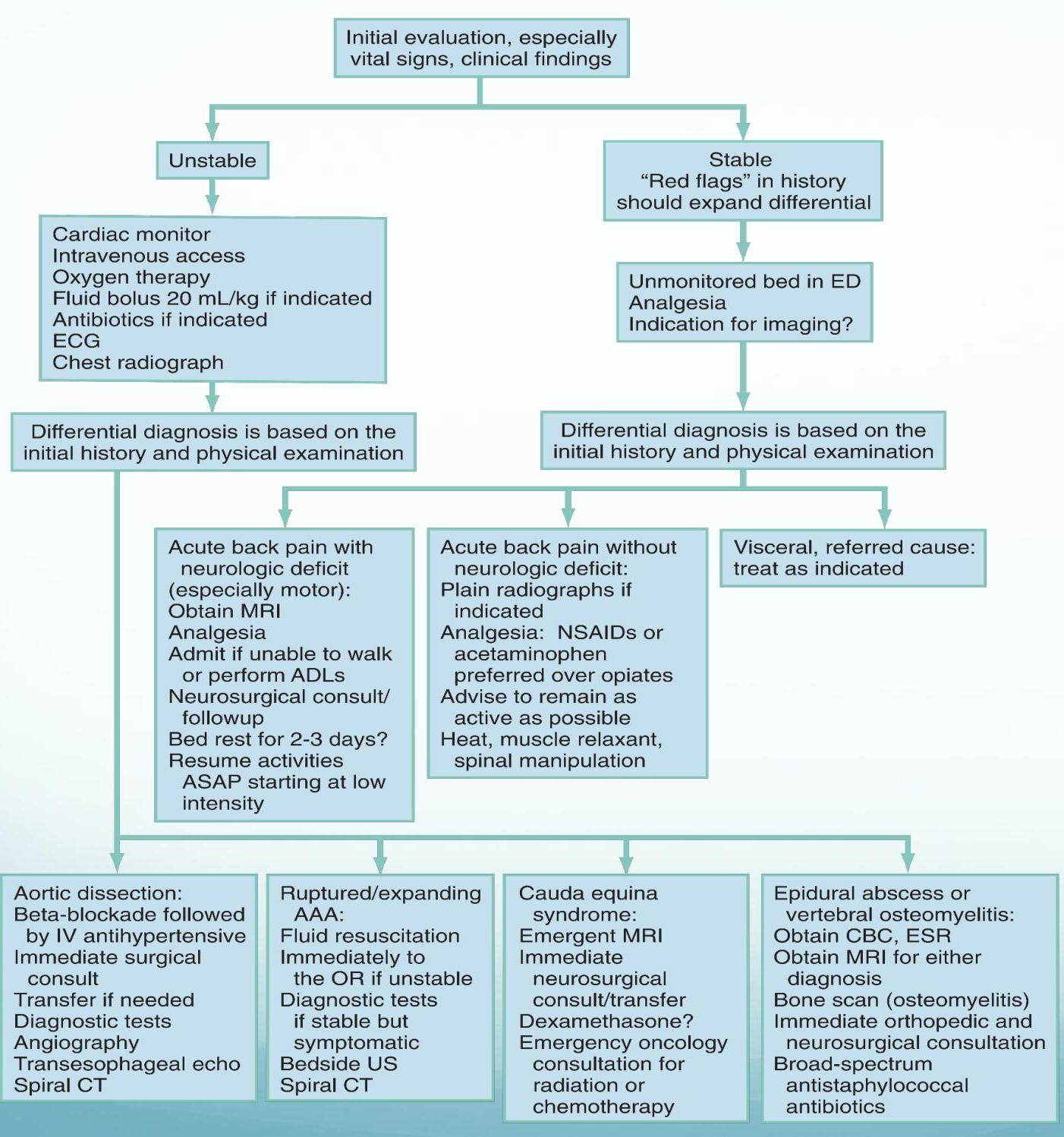
Rosen’s 8th edition
Take Home Message
- Imaging is NOT generally needed to diagnose acute low back pain.
- Always look for RED FLAGS.
- Do NOT stop everyday activity and exercise (but no heavy lifting).
- Acetaminophen and NSAIDs are first line pain medications unless there is contraindication.
