PEDIATRIC DIABETIC KETOACIDOSIS
Dr Tariq Al thobaiti ,MBBS
Pediatric Diabetic Ketoacidosis
- Children with Diabetes specially type I, remain at risk for developing diabetic ketoacidosis (DKA).
- Children who are type I diabetics have incidence of DKA of 8/100 patients.
- In children younger than 19 years old, DKA is the admitting diagnosis in 65% of all hospital admissions of patients with diabetes mellitus.
Pediatric Diabetic Ketoacidosis
- The overall mortality rate for children in DKA is not unimpressive.
- Range of mortality is between 0.15 – 0.31 %
- The mortality associated with cerebral edema may approach 20-50 %
- The incidence of neurologic morbidity is significant and reported in 35-40% of survivors.
- Cerebral edema has largely been a complication of treatment in the pediatric population.
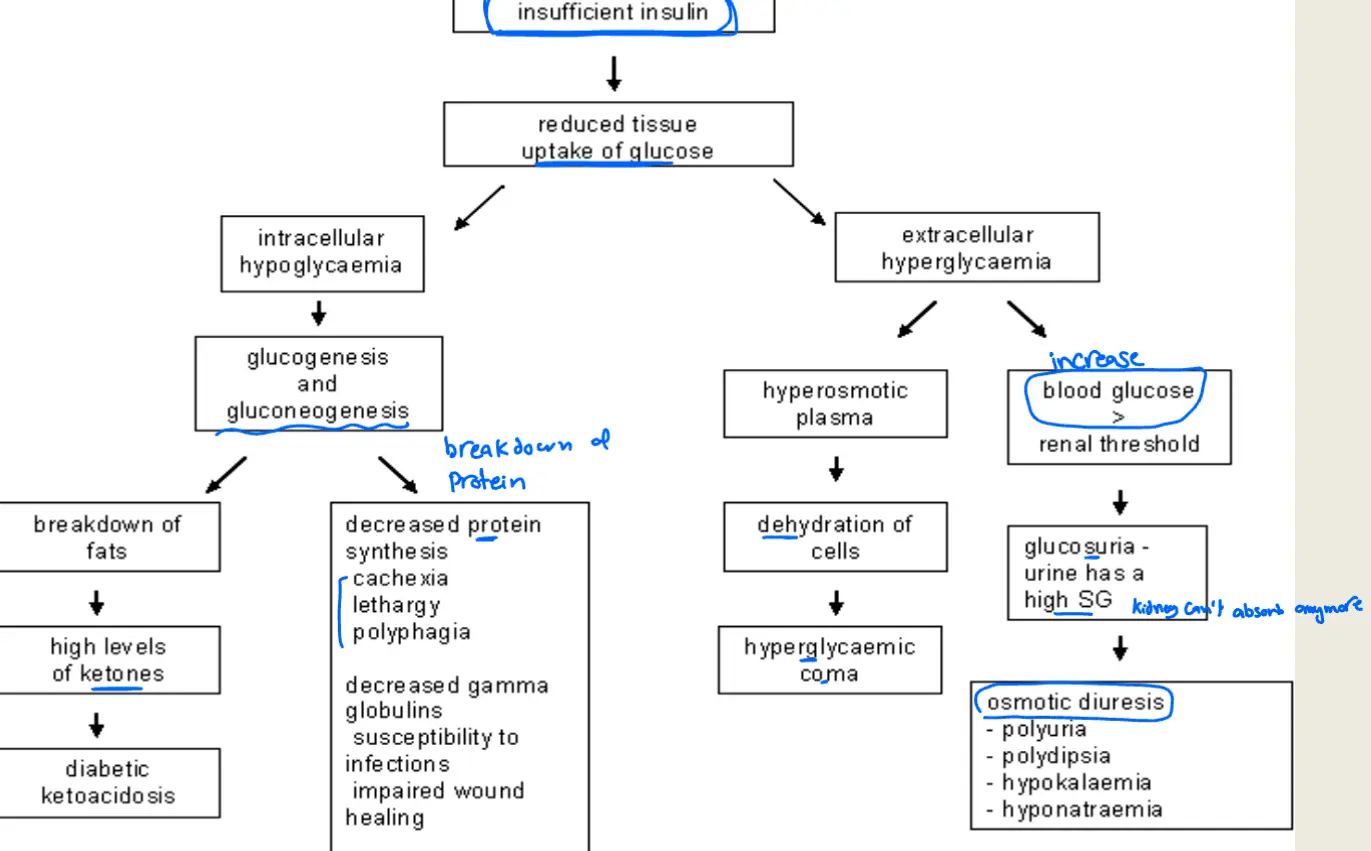
Pathophysiology of Diabetes Type I
Pediatric Diabetic Ketoacidosis
DEFINITION:
-
Hyperglycemia >200mg/dl = 11 mmol/l
-
Acidosis ph<7.3
-
Bicarbonate < 15 meq/l
-
Ketonemia (Beta hydroxy butyrate and acetoacetate) >3 mmol/l
-
Ketonuria
ETIOLOGY:
- Error in insulin management at home or inadequate insulin administration.
- Secondary to child or parental non-compliance because of emotional and psychological stress
- Insulin pump malfunction
- Infections any stress
- Pre-pubertal and pubertal phase
* 1 st presentation
Assessment of severity of diabetic ketoacidosis in children
| Mild | Moderate | Severe | |
|---|---|---|---|
| Defining features | |||
| Venous pH | 7.2-7.3 | 7.1-7.2 | <7.1 |
| Serum bicarbonate (mEq/L) | 10-15 | 5-10 | <5 |
Clinical Presentation:
- Sometimes can be challenging and subtle requiring high degree of suspicion.
- Classically: Polyuria, Polydipsia, weight loss also abdominal pain, nausea, vomiting.
- Physical examination:
-
- Dehydrated
-
- Dry mucous membranes, tachycardia, delayed capillary refill, hypo-perfusion, hypothermia, kussmaul’s breathing, diffuse abdominal pain.
Management:
1- Fluids:
-
1st ABCD
-
2nd Look For the Cause
-
3rd Treat the Cause
-
1- Fluids: Carefully regulated treatment plan to prevent the most lethal complication of DKA → cerebral edema & electrolytes
-
pediatric dose: 10-20 ml x Kg until normalize the vital sign
-
in adult: 1 l
-
then calculate deficit (4, 2, 1)
-
give 1 1/2 maintenance
2- Electrolytes:
check for K before you start insulin
A- serum sodium:
- As serum glucose fall with therapy, serum sodium should rise to normal or above normal level.
- Clinicians should consider the possibility of pseudohyponatremia that may result from elevated glucose.
- Corrected Na level: Na decreased 1.6mEq/l for each 100mg/dl rise in glucose
B- serum potassium:
- At initial presentation in DKA, normally they have high or normal potassium level even though total body potassium stores are depleted (extra-cellular shift of potassium)
- Potassium is lost from the body via 3 routes: vomiting, urinary loss.
- Massive volume depletion 2ry hyperaldosteronism increased excretion of potassium through kidney.
CAUSES: because of high acid (Pseudohyperkalemia) but need K+ after insulin dose because will back into cell
- High plasma osmolality osmotic shift of water to ECF potassium follows this gradient hyperkalemia
- Acidosis
- Insulin deficiency glycogenolysis and proteolysis worsen osmotic gradient.
C- Serum phosphate:
-
Renal excretion of phosphate + rapid entry of phosphate intracellularly hypophosphatemia
-
Phosphorus replacement if level below 1 mg/dl as it may cause muscle weakness and insult diaphragmatic tissues.
-
Always keep in mind that phosphorus administration may cause hypocalcemia.
Insulin as infusion
3- Insulin and glucose:
- Although there is consensus that blood sugar level must be greater than 200 mg/dl for patient to be in DKA, there are some infrequent reports of euglycemic DKA.
Reasons:
- Fasting child.
- Poor nutrient intake
- Insulin is crucial in the treatment of pediatric DKA as it suppresses lipolysis and ketogenesis.
- Care should be taken to avoid precipitous drop in glucose level, should not drop at a rate faster than 100mg/dl/hr to decrease the risk of cerebral oedema.
4- Acidosis and bicarbonate:
- There is absolutely no role for bicarbonate administration in DKA patients leads to cerebral oedema (paradoxical CNS acidosis).
Indications for bicarbonate administration:
- Severe academia with
- Life threatening hyperkalemia with ECG changes.
- Causing arrhythmia
Complications of DKA:
1- Hypoglycemia:
-
2ry to insulin infusion→ Do hourly blood glucose check.
-
Treatment: various types of IV dextrose
-
if BG
-
now change fluid to dextrose 5%.
2- Hypokalemia:
-
2ry to insulin therapy which shifts potassium intracellularly.
-
Potassium losses from the body via: vomiting, urinary loss.
-
Massive volume depletion→2ry hyperaldosteronism→increased excretion of potassium through kidney.
-
It is prudent to add some potassium chloride to IVF according to protocol.
3- Cerebral edema:
-
treat it by hypertonic saline
-
It is a multifactorial process
-
(cerebral oligemia, hyperemia, inflammation, cyto-toxic insult)
-
Overhydration leads to cerebral edema.
-
bicarbonate administration in DKA patients leads to cerebral oedema (paradoxical CNS acidosis).
-
Rapid drop in glucose level leads to osmotic shift cerebral edema
-
Failure of correction of Na with treatment
-
Epidemiologically patients with high blood urea concentrations are at risk.
-
Epidemiologically patients with severe hypocapnia are at risk for cerebral edema.
Clinically:
- Altered mental status
- Headache
- Vomiting
- Bradycardia
- Hypertension
- Irregular breathing
- Seizures
- Anisocoria
maybe alter DKA protocol
- Hypoglycemia is defined as a plasma glucose level of <45 milligrams/dL in any symptomatic patient or <35 milligrams/dL in an asymptomatic neonate.
- Evaluation of urine for ketones is the second important step. Ketonuria is characteristic of ketotic hypoglycemia, adrenal or growth hormone deficiency, and other inborn errors of metabolism.
Hypoglycemia
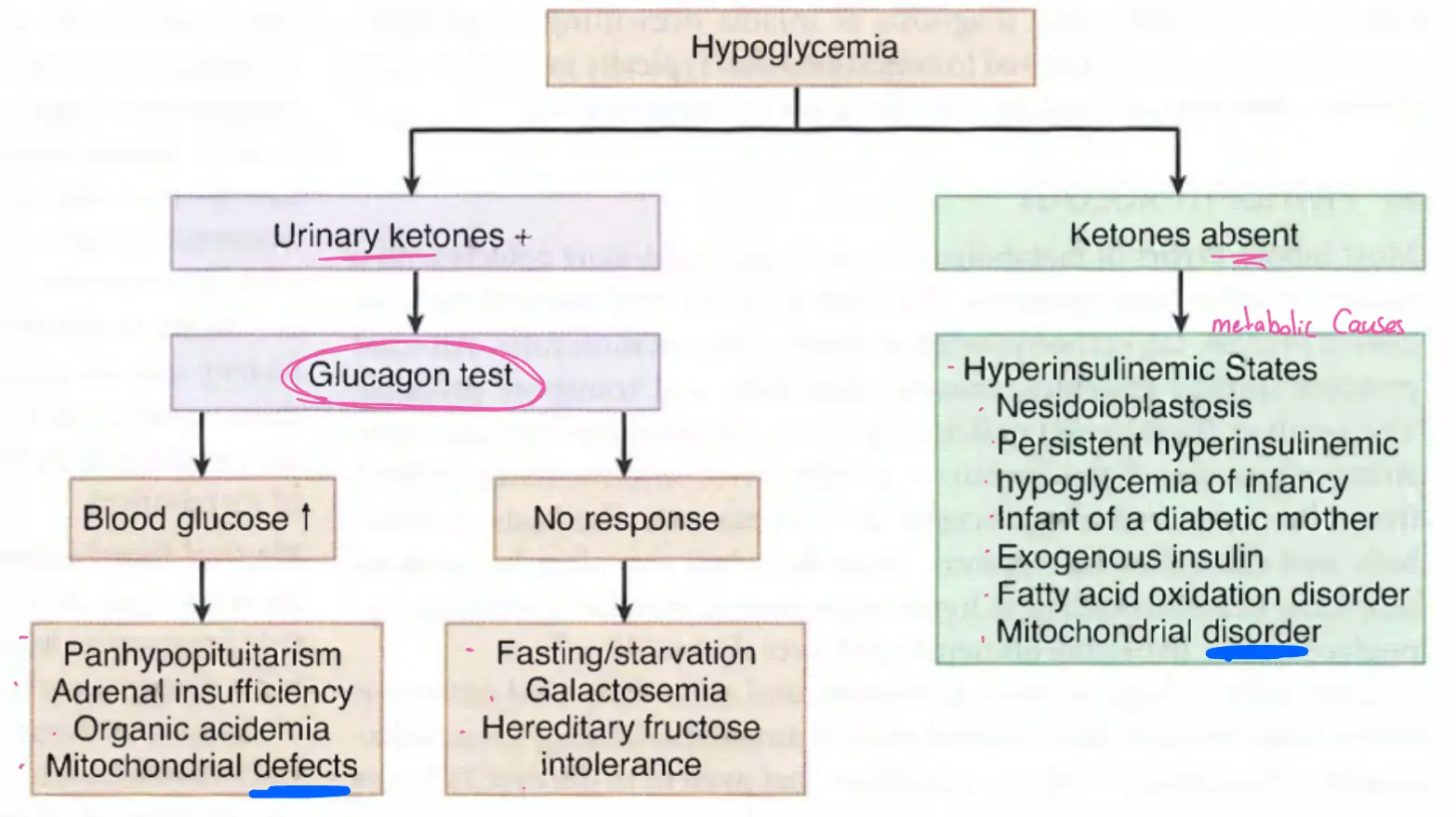
TABLE 137-1 Management of Hypoglycemia in the ED
| Patient Age | Dextrose Bolus Dose | Dextrose Maintenance Dosage | Other Treatments to Consider |
|---|---|---|---|
| Neonate | D10 5 mL/kg PO/NG/IV/IO → give 5 | 6 mL/kg/h D10 | Glucagon, 0.3 milligram/kg IM Hydrocortisone, 25 grams PO/IM/IV/IO |
| Infant | D10 5 mL/kg PO/NG/IV/IO or D25 2 mL/kg | 6 mL/kg/h D10 | Glucagon, 0.3 milligram/kg IM Hydrocortisone, 25 grams PO/IM/IV/IO |
| Child | D25 2 mL/kg PO/NG/IV/IO → give 2 to reach 50 | 6 mL/kg/h D10 for the first 10 kg + 3 mL/kg/h for 11–20 kg + 1.5 mL/kg/h for each additional kg >20 kg | Glucagon, 0.3 milligram/kg IM Hydrocortisone, 50 grams PO/IM/IV/IO |
| Adolescent | — | 6 mL/kg/h D10 for the first 10 kg + 3 mL/kg/h for 11–20 kg + 1.5 mL/kg/h for each additional kg >20 kg | Glucagon, 0.3 milligram/kg IM Hydrocortisone, 100 grams PO/IM/IV/IO |
| adult | D50 |