Pulmonary Embolism
Mohammed Alageel MBBS FRCP(C) ABEM
Goals
- Review the pathophysiology of thromboembolic disease
- Assess the diagnostic strategy and approach to pulmonary embolisms
- Review diagnostic modalities in pulmonary embolisms
- Define UpToDate guidelines in regard to thromboembolic disease
Definition
- Lungs are responsible for gas exchanges and the blood flow to the lungs for that exchange occurs through the pulmonary arteries
- If a blood clot (thrombus) forms in one of the body’s veins (deep vein thrombosis or DVT), it has the potential to embolize (move) through the circulatory system through the heart and become lodged in one of the branches of the pulmonary artery of the lung
- A pulmonary embolus is one of the life-threatening causes of chest pain and should always be considered when a patient presents to a healthcare provider with complaints of chest pain and shortness of breath
Types of Pulmonary Embolism
- Primarily due to thromboembolic event → DVT
- Fat embolism (blunt trauma and in bone fractures)
- Amniotic fluid embolism (pregnancy)
- Tumor embolism (renal cell carcinoma)
- Air embolism (central catheter placement)
- IV drug users self-inject hair, talc, and cotton that contaminate the drug they have acquired. These patients also have susceptibility to septic PE, which can cause endocarditis of the tricuspid or pulmonic valves
Pathophysiology and Risk Factors
Virchow’s Triad
Rudolf Virchow (1821–1902), who first described PE.
 The three components of Virchow’s triad that contribute to thrombus formation:
The three components of Virchow’s triad that contribute to thrombus formation:
- Intimal vessel injury
- Stasis of blood flow
- Hypercoagulability
Risk Factors for Venous Thromboembolism
Modifiable Risk Factors
- Obesity
- Metabolic syndrome
- Cigarette smoking
- Hypertension
- Abnormal lipid profile
- High consumption of red meat and poor consumption of fruits/vegetables
Non-Modifiable Risk Factors
- Advancing age
- Arterial disease, including carotid and coronary disease
- Personal or family history of venous thromboembolism
- Recent surgery, trauma, or immobility, including stroke
- Congestive heart failure
- Chronic obstructive pulmonary disease
- Acute infection
- Air pollution
- Long-haul air travel
- Pregnancy, oral contraceptive pills, or postmenopausal hormone replacement therapy
- Pacemaker, implantable cardiac defibrillator leads, or indwelling central venous catheter
- Prothrombin gene mutation
- Antithrombin deficiency
- Protein C deficiency
- Protein S deficiency
- Antiphospholipid antibody syndrome
Clinical Presentation
Symptoms
Symptoms vary and may include:
- Chest pain, often pleuritic but can be non-specific
- Dyspnea (shortness of breath)
- Anxiety
- Cough
- Cardiac arrest due to impaired right ventricular function
Signs
- Tachycardia
- Tachypnea
- Low-grade fever
- Accented P2 - no heart sound
- Hemoptysis
- Leg edema (exam findings of DVT)
Diagnostic Evaluation
Blood Tests
- Regular blood tests are often normal
- Troponin may be normal if not ischemic cause
- D-dimer has a high negative predictive value (sensitive but not specific)
- Good screening test but has false positives
- If negative, helps exclude diagnosis but not 100% certain
- Generally not useful for acutely ill hospitalized inpatients (usually elevated)
- A normal D-dimer appears as diagnostically useful as a normal lung scan to exclude PE
- Patients with low clinical probability and negative D-dimer may not need additional testing* Z
Electrocardiogram (EKG) Findings
no specific
- Most patients have sinus tachycardia
- Incomplete or complete bundle branch block with right axis deviation
- T wave inversion in leads III and aVF or in leads V1-V4 (diffuse)
- S wave in lead I and Q wave with T wave inversion in lead III (S1Q3T3 pattern)
- Usually not present but very specific when present
- Atrial fibrillation and flutter
Imaging Studies
Chest X-ray (CXR)
- Mostly normal - severe respiratory distress with normal CXR should raise suspicion of PE
- Focal oligemia (Westermark sign) indicates massive central embolic occlusion (very rare)
- Peripheral wedge-shaped density above diaphragm (Hampton hump) indicates pulmonary infarction
- Subtle abnormalities include enlargement of descending right pulmonary artery
Computed Tomography (CT) Angiography
Gold Standard Test
- Spiral CT or CT angiography
- Defines size, location, and extent of thrombus
- May identify other diagnoses explaining PE symptoms:
- Pneumonia
- Atelectasis
- Pericardial effusion
- Pneumothorax
- Left ventricular enlargement
Other CT Features
- Pulmonary artery enlargement (suggestive of pulmonary hypertension)
- Age of thrombus: acute, subacute, chronic
- Location of thrombus: pulmonary arteries, pelvic veins, deep leg veins, upper extremity veins
- Right ventricular enlargement (pulmonary hypertension)
- Contour of interventricular septum: bulging toward left ventricle indicates right ventricular pressure overload (massive or submassive PE)
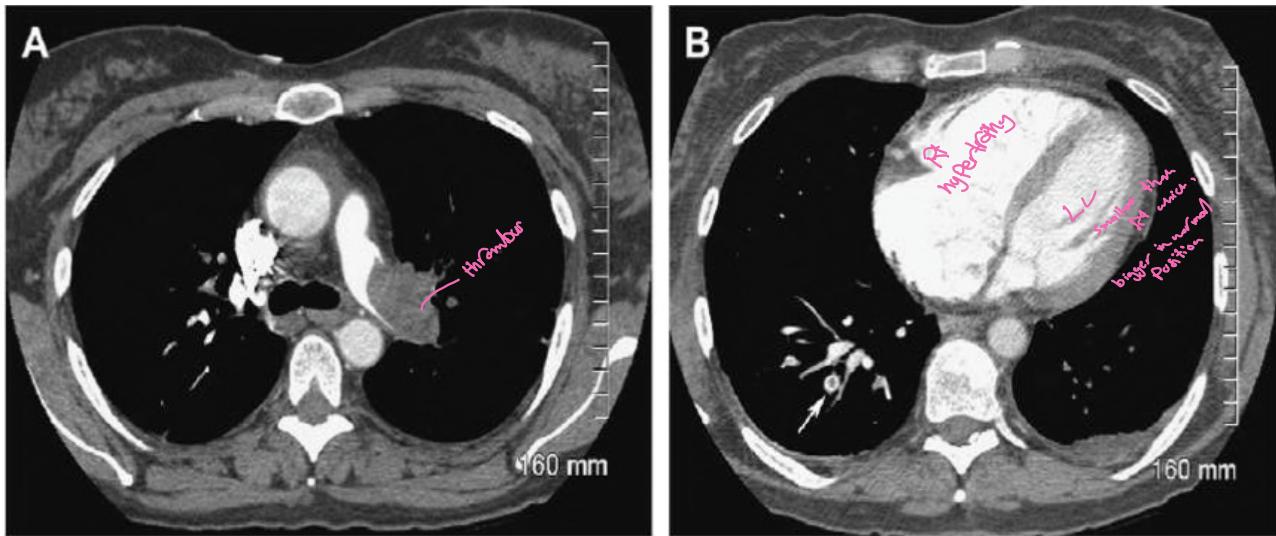
Two axial CT scans of the chest:
- A) Shows acute pulmonary embolism (PE) in the left main pulmonary artery (LMA) as a complete filling defect
- B) Shows right ventricle (RV) and right atrium (RA) moderately dilated, with central partial filling defect of acute PE (arrow) in right lower lobe posterobasal segmental artery (Polo mint sign)
Other Imaging Modalities
- Duplex ultrasound of deep veins (for patients who cannot receive contrast)
- V/Q scan may have role in pregnant patients, severe anaphylaxis, and possibly renal insufficiency
- Pulmonary angiography (previous reference standard, usually used to remove thrombus)
- Contrast venography
Differential Diagnosis
- Anxiety, pleurisy, costochondritis
- Pneumonia, bronchitis
- Myocardial infarction
- Pericarditis
- Congestive heart failure
- Idiopathic pulmonary hypertension
Clinical Decision Rules and Scoring Systems
Wells Criteria
Clinical Decision Rule:
-
4 score points = high probability
- ≤4 score points = non-high probability
| Criteria | Points |
|---|---|
| DVT symptoms or signs | 3 |
| Alternative diagnosis is less likely than PE | 3 |
| Heart rate > 100/min | 1.5 |
| Immobilization or surgery within 4 weeks | 1.5 |
| Hemoptysis | 1 |
| Cancer treated within 6 months or metastatic | 1 |
Geneva Score
| Variable | Points |
|---|---|
| Age > 65 years | +1 |
| Previous venous thromboembolism | +3 |
| Surgery requiring anesthesia or fracture of lower limb in past month | +2 |
| Active malignancy | +2 |
| Unilateral leg pain | +3 |
| Hemoptysis | +2 |
| Unilateral leg edema | +4 |
| Heart rate 75-94 bpm | +3 |
| Heart rate > 95 bpm | +5 |
| Probability of PE | Score | Prevalence of PE |
|---|---|---|
| Low | ≤3 | 8% |
| High | >11 | 74% |
PERC Score
Used to rule out need for D-dimer testing in low-risk PE patients.
| Criteria | Points |
|---|---|
| Clinical signs and symptoms of DVT | 3 |
| PE is #1 diagnosis OR equally likely | 3 |
| Heart rate > 100 | 1.5 |
| Immobilization at least 3 days OR surgery in previous 4 weeks | 1.5 |
| Previous, objectively diagnosed PE or DVT | 1.5 |
| Hemoptysis | 1 |
| Malignancy with treatment within 6 months or palliative | 1 |
Simplified PESI Score
| Parameters | Points |
|---|---|
| Age > 80 years | +1 |
| History of cancer | +1 |
| History of cardiopulmonary disease | +1 |
| Systolic BP < 90 mm Hg | +1 |
| Heart rate > 110 beats/minute | +1 |
| O₂ saturation < 90% | +1 |
Disease Severity Classification
Massive Pulmonary Embolism
- Patients susceptible to cardiogenic shock and multisystem organ failure
- Hypotension requiring pressor support is defining feature
- Renal insufficiency, hepatic dysfunction, and altered mentation common
- Thrombosis affects at least half of pulmonary arterial vasculature
- Clot typically present bilaterally
- Dyspnea common; chest pain unusual
- Transient cyanosis common
- Cardiac arrest possible
Moderate to Large (Submassive) Pulmonary Embolism
- Patients frequently present with moderate or severe right ventricular hypokinesis
- Elevated troponin, pro-BNP, or BNP
- Maintain normal systemic arterial pressure
- May appear clinically well initially (misleading)
- At risk to progress to massive pulmonary embolism
- At risk for chronic thromboembolic disease causing pulmonary hypertension
- Requires hospital admission
- Consider thrombolytic therapy or embolectomy if moderate/severe RV dysfunction persists
- Consider IVC filter if anticoagulation fails
• Especially if moderate or severe right ventricular dysfunction persists, one should consider thrombolytic therapy or embolectomy. (controversial)
• If neither thrombolysis nor embolectomy appears warranted, placement of an inferior vena caval filter is controversial but may be employed as a “back-up” in case heparin anticoagulation fails.
Small to Moderate Pulmonary Embolism
- Most common presentation
- Normal systemic arterial pressure
- No cardiac biomarker release
- Normal right ventricular function
- Patients appear clinically stable
- Adequate anticoagulation results in excellent clinical outcome
- Can be discharged from emergency department
Complications
Pulmonary Infarction
- Characterized by pleuritic chest pain (may be unremitting or wax/wane)
- Pleurisy occasionally accompanied by hemoptysis
- Embolus usually lodges in peripheral pulmonary arterial tree near pleura
- Tissue infarction occurs 3 to 7 days after embolism
- Syndrome includes fever, leukocytosis, elevated ESR, and radiologic evidence of infarction
Treatment
Prevention
Best treatment is prevention of reversible causes:
- Immobility
- Smoking
- Steroid use
- Obesity
Anticoagulation Regimens
Suggested Anticoagulation for Initial Treatment of VTE
DVT, Lower Extremity:
- LMWH:
- Enoxaparin, 1 mg/kg subcutaneously twice daily
- Enoxaparin, 1.5 mg/kg subcutaneously daily
- Tinzaparin, 175 units/kg subcutaneously daily
- Dalteparin, 200 units/kg subcutaneously daily
- Subcutaneous UFH with aPTT monitoring:
- 15,000 units or 17,500 units every 12 h (initial dose for patients weighing 50–70 kg and >70 kg, respectively)
- Subcutaneous UFH without aPTT monitoring:
- 330 units/kg × 1 then 250 units/kg every 12 h
- Fondaparinux:
- 7.5–10 mg subcutaneously daily, depending on weight
- IV UFH:
- 80 units/kg bolus (minimum 5,000 units; maximum 10,000 units) followed by continuous infusion of 18 units/kg/h
- Note: Begin warfarin concurrent with initial dose of parenteral anticoagulant
DVT, Upper Extremity:
- Consider thrombolysis in appropriate candidates
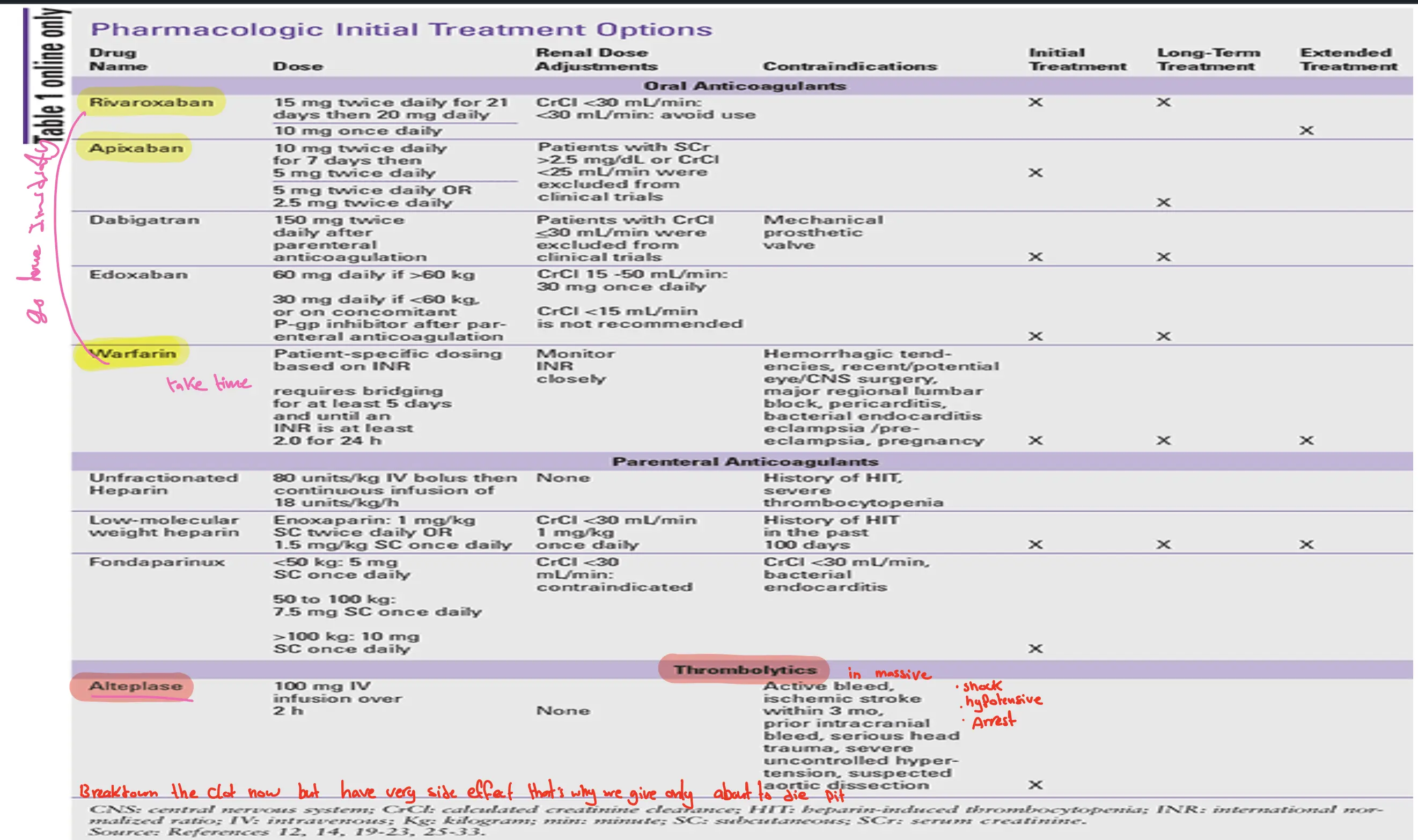
Pharmacologic Treatment Options
Duration of Anticoagulation
-
Provoked PE (specific factor trigger like surgery, immobilization):
- First provoked PE/proximal leg DVT: 3 to 6 months
- First provoked upper extremity DVT or isolated calf DVT: 3 months
- Second provoked VTE: Uncertain
- Third VTE: Indefinite duration
-
Unprovoked PE (no specific factor):
- Unprovoked PE/proximal leg DVT: Consider indefinite duration
- First unprovoked calf DVT: 3 months
- Second unprovoked calf DVT: Uncertain
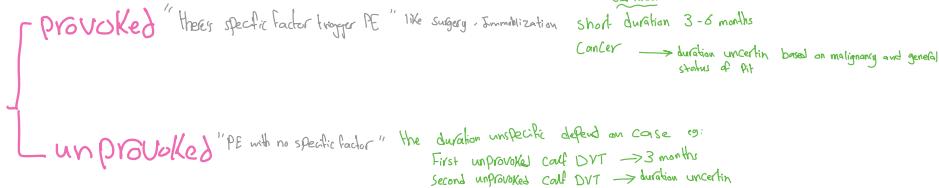
- Cancer-related VTE:
- Duration uncertain based on malignancy and general status
- Consider indefinite duration or until cancer resolved
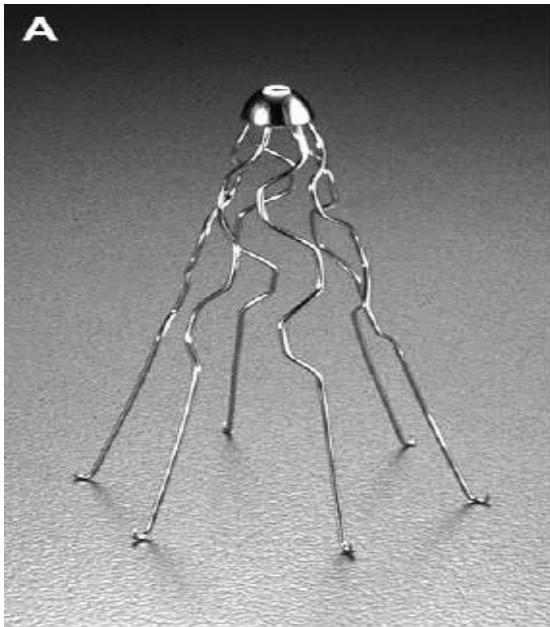
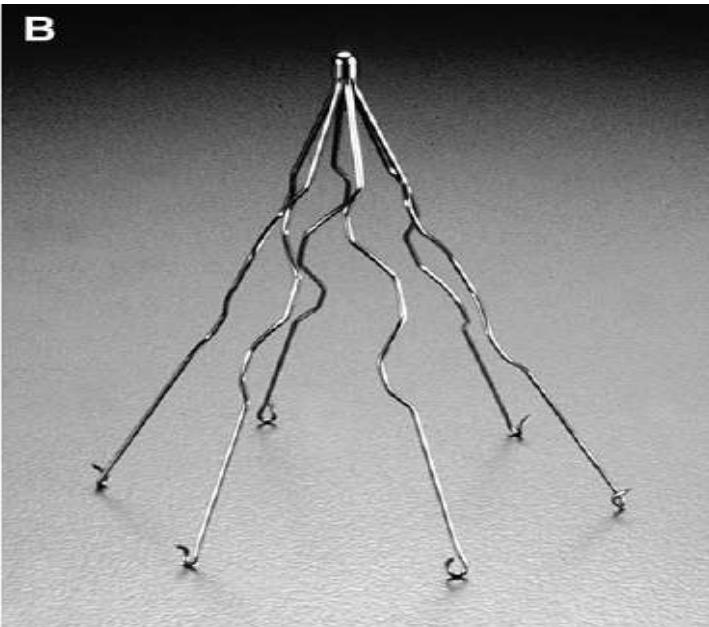
Inferior Vena Cava (IVC) Filters
Indications:
- Patients who cannot take anticoagulants (e.g., active bleeding, liver failure, renal failure, upper GI bleeding)
- Contraindications to anticoagulation
- Bleeding complications during anticoagulation
- Extension of known thrombosis/recurrent PE during therapeutic anticoagulation
- Chronic thromboembolic pulmonary hypertension
Clinical Pearls
-
Patients with respiratory distress and unremarkable chest imaging should be suspected to have PE until proven otherwise
-
Thrombolytics have proven benefit only in cases of shock or cardiac arrest
-
IVC filters have very limited indications, most often used in patients with active thromboembolic disease and contraindication to anticoagulation
-
Most patients with pulmonary embolism can be initiated on oral anticoagulation and likely discharged home