Abnormal Labour
Definition
Abnormal labour refers to a labour that does not progress normally, either due to issues with the power (uterine contractions), the passenger (fetus), or the passage (birth canal).


Aetiologies
The causes of abnormal labour can be categorized into three main areas:
- Power: Poor uterine contraction; 1st stage, poor maternal effort; 2nd stage.
- Passenger: Large baby, malpresentation.
- Passage: Contracted pelvis, soft tissue abnormalities (myoma, cervical cancer).
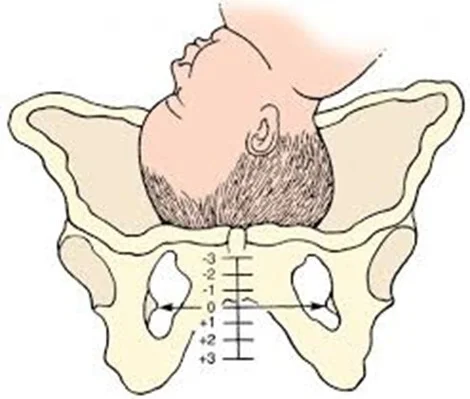
Abnormal Labor Indicators Y
| Indication | Nullipara | Multipara |
|---|---|---|
| Prolonged latent phase | >20 h | >14 h |
| Average second stage | 50 min | 20 min |
| Prolonged second stage without (with) epidural | >2 h (>3 h) | >1 h (>2 h) |
| Protracted dilation | < 1.2 cm/h | < 1.5 cm/h |
| Protracted descent | < 1 cm/h | < 2 cm/h |
| Arrest of dilation* | >2 h | >2 h |
| Arrest of descent* | >2 h | >1 h |
| Prolonged third stage | >30 min | >30 min |
When We Consider Labour as Abnormal
- Poor progress (as evidenced by a delay in cervical dilatation or descent of the presenting part)
- The fetus shows signs of compromise.
- There is a fetal malpresentation
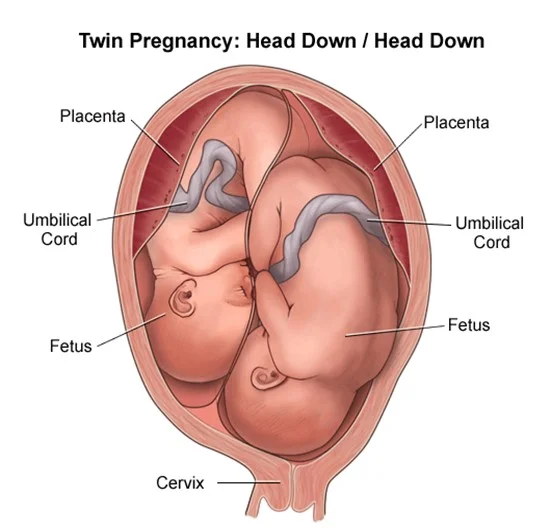
- A multiple gestation
- A uterine scar
- Labour has been induced.
Complications
- Maternal infection
- Fetal compromise.
- Hyperstimulation of the uterus. ⇒ rupture
- fetal compromise.
- cord compression.
- Uteroplacental insufficiency.
- Uterine rupture.
- Postpartum hemorrhage
Power (Uterine Contraction)
Types of Abnormal Uterine Contraction
- hypotonic uterine dysfunction
- oxytocin
- hypertonic/uncoordinated uterine dysfunction
- tocolytic / position fluid
Poor Progress
First Stage of Labour
Defined as cervical dilatation of less than 2 cm in 4 hours. Usually associated with failure of descent and rotation of the fetal head. Divided into: Primary and secondary arrest
Poor Progress in the Second Stage of Labour
Diagnosed if delivery is not imminent after 2 hours in a nulliparous & 1 hour in a parous woman. With epidural use …3 hours in nulliparous (prolonged w/ epidural) …and 2 hours in parous women
Causes of Poor Progress in Labour
- A. Dysfunctional uterine activity
- B. Abnormal fetal size, presentation, and position.
- C. Abnormalities of the birth canal (the ‘passages’)
passage - passenger - power
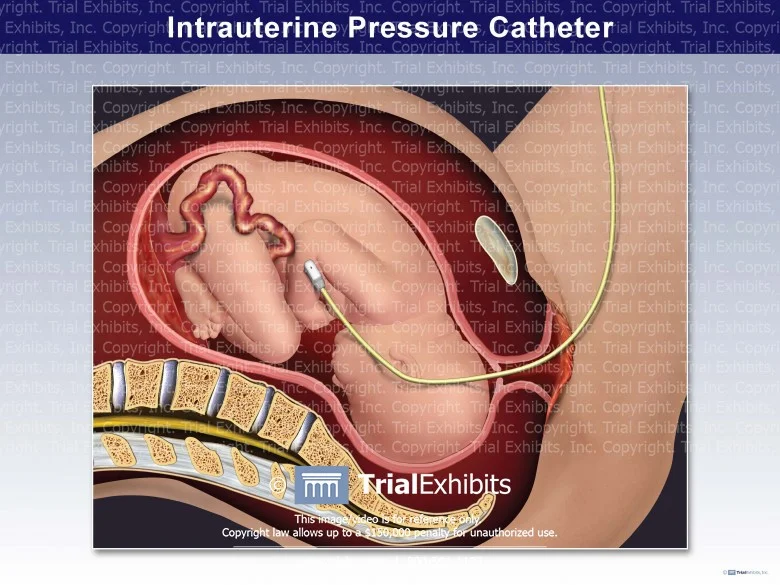
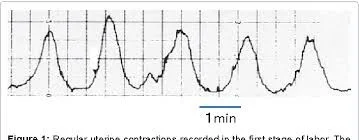
Assessing Uterine Activity
- By clinical examination
- By using external uterine topography (CTG)
- Intrauterine pressure catheters
Efficient Uterine Contractions Z
- 3-4 cont. 10 min.
- Each lasting 45-60 sec.


Passenger (Fetal Causes)
- Abnormal fetal size…fetal macrosomia:
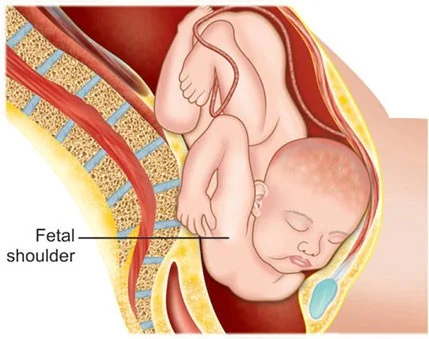
- Abnormal fetal presentation
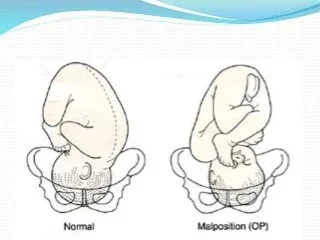
- Abnormal Fetal position

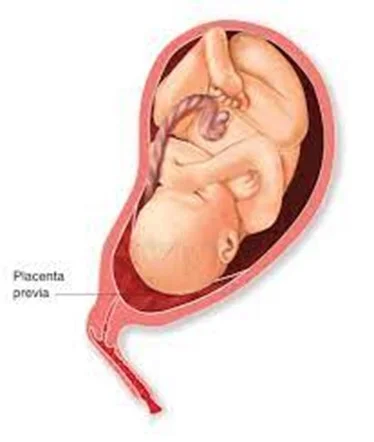
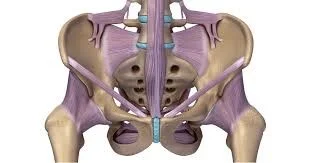
Passage (Birth Canal)
- Abnormalities of the birth canal.
- The bony pelvis may cause delay in the progress of labour (android pelvis).
- Abnormalities of the uterus and cervix can also delay labour
- fibroid in the lower uterine segment.
- cervical dystocia (noncompliant cervix)
- …….usually as a result of cone biopsy.
Cephalopelvic Disproportion (CPD)
Anatomical disproportion between the fetal head and maternal pelvis
Causes of CPD
- Large head. B
- Small pelvis. P
- Combination of the two. B&P
- Previous fracture. P
- Metabolic bone disease. P
- Fetal anomaly (hydrocephaly). B
- Malposition like OP. B
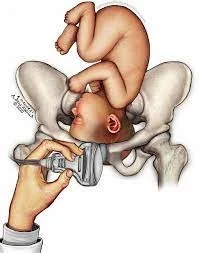
Diagnosis of Cephalopelvic Disproportion
- Progress is slow or actually arrests despite efficient uterine contractions
- The fetal head is not engaged
- Vaginal examination shows severe moulding and caput formation
- The head is poorly applied to the cervix
- Haematuria