Amenorrhea
Definitions
Amenorrhea is the absence of menses, could be: Z
- Physiologic during pregnancy, lactation and menopause.
- Pathologic :the lack of menses for any other reason after the expected age of menarche.
a. Primary amenorrhea:
- No menses by age 14 years in the absence of secondary sexual development
- or
- No menstruation by age 16 years with the presence of secondary sexual characteristics.
b. Secondary amenorrhea:
- The absence of menses in a previously menstruating woman.
- It is also defined as the lack of menses for 6 months or for three menstrual cycles in women that have experienced menarche.
World Health Organization (WHO) Amenorrhea Groups
-
WHO group I (hypogonadotropic hypoestrogenic) has no endogenous estrogen production, normal or low follicle-stimulating hormone (FSH) levels, normal prolactin (PRL) levels, and no lesion in the hypothalamus or pituitary.
-
WHO group II (normogonadotropic normoestrogenic) has endogenous estrogen production and normal levels of FSH and PRL.
-
WHO group III (hypergonadotropic hypoestrogenic) has elevated FSH levels and low to absent estrogen, indicative of premature ovarian failure (POF).


Differential Diagnosis of Primary Amenorrhea
Table 39-1
| Breast Development Present | Breast Development Absent | |
|---|---|---|
| Uterus present |
|
Hypothalamic or pituitary failure
|
| Uterus absent |
|
Androgen Insensitivity (Testicular Feminization) Breast Present, Uterus Absent
-
Etiology : absence of androgen receptors or lack of responsiveness to androgen stimulus.
-
Genetic :X- linked, recessive disorder
-
karyotype 46 XY
-
Gonads: normally functioning Intra-abdominal testes .
-
Hormones :normal male levels of testosterone and dihydrotestosterone.
- The müllerian ducts regress due to the presence of antimüllerian hormone.
-
Internal organs :no male or female internal genitalia
- The wolffian ducts do not develop because they are not stimulated by testosterone.
-
External genitalia : have normal female ,short or absent vagina.
-
2ry Sexual characteristic: normal breasts tanner stage IV and scant or absent axillary and pubic hair.
-
Risk :Intra-abdominal testes or those in the inguinal canal have an ↑ risk of developing a malignancy (gonadoblastoma or dysgerminoma), usually after age 20.
-
Management :The gonads should be removed after puberty to allow for breast development and adequate bone growth. Estrogen is then given. These patients are raised as females.
Breast Present, Uterus Absent
Table 42-1 MÜLLERIAN AGENESIS VERSUS ANDROGEN INSENSITIVITY
| MÜLLERIAN AGENESIS | ANDROGEN INSENSITIVITY | |
|---|---|---|
| Breast tissue | Normal breast development | Normal breast development |
| Axillary and pubic hair | Normal | Scant or absent |
| Uterus and vagina | Absent uterus and blind vagina | Absent uterus and blind vagina |
| Testosterone level | Normal testosterone | High testosterone (male range) |
| Karyotype | 46,XX | 46,XY |
| Complications | Renal anomalies | Need gonadectomy |
Causes of Secondary Amenorrhea
Physiological: pregnancy, post OCP amenorrhea and lactat. amenorrhea Outflow tract: (normogonadotropic, normogonadism): a. Cervical stenosis :due to Surgical procedure (i.e., LEEP) b. Asherman syndrome :(intrauterine synechiae) :
- Causes:
- Aggressive postpartum curettage or abortion.
- uterine or cervical surgeries, such as cesarean section, septoplasty and myomectomy.
- Infectious causes include :endometritis, tuberculosis, schistosomiasis.
- Diagnosis can be confirmed with HSG, Sonohysterogram, or hysteroscopy.
- Treatment requires hysteroscopic lysis of intrauterine adhesions and placement of intrauterine stent or hormonal IUCD.
Ovarian Cause
1-Premature ovarian failure: Z
- ✔️ Idiopathic.
- ✔️ Chromosomal abnormality.
- ✔️ Autoimmune disease.
- ✔️ Infection. (Mumps)
- ✔️ Iatrogenic.
2-Polycystic ovary syndrome. Z
Pituitary Causes (Hypo/Hypo)
a. Hyperprolactinemia : Etiology : pituitary adenoma, drugs (e.g) Antipsychotics, metocloprami hypothyroidism
- cause negative feedback on hypothalamic GnRH secretion thereby lowering gonadotropin release.
- May associated galactorrhea
Dx: serum prolactin level, TFT , MRI of brain if PRL>1000. Rx : dopamine agonist therapy (bromocriptine or cabergoline)
b. Sheehan syndrome : pituitary necrosis and hypopituitarism following postpartum hemorrhage and hypotension.
Dx :
- Hormone profiles including cortisol, plasma ACTH, thyroid hormones, TSH, FSH, LH and prolactin were all low as a result of panhypopituitarism
- pituitary and cerebral MRI which showed an *empty sella turcica
Rx : replacement of pituitary hormones (thyroxin , hydrocortisone ,HRT)
CNS Causes
Hypothalamic Dysfunction:
- Stress.
- Eating disorders ( e,g anorexia nervosa).
- Weight loss , athletes
Brain injury Inflammatory or infiltrative process
Other Endocrinopathies
- Hypothyroidism: Thyrotropin-releasing hormone (TRH) stimulates the release of TSH and PRL from the anterior pituitary
- late-onset adrenal hyperplasia
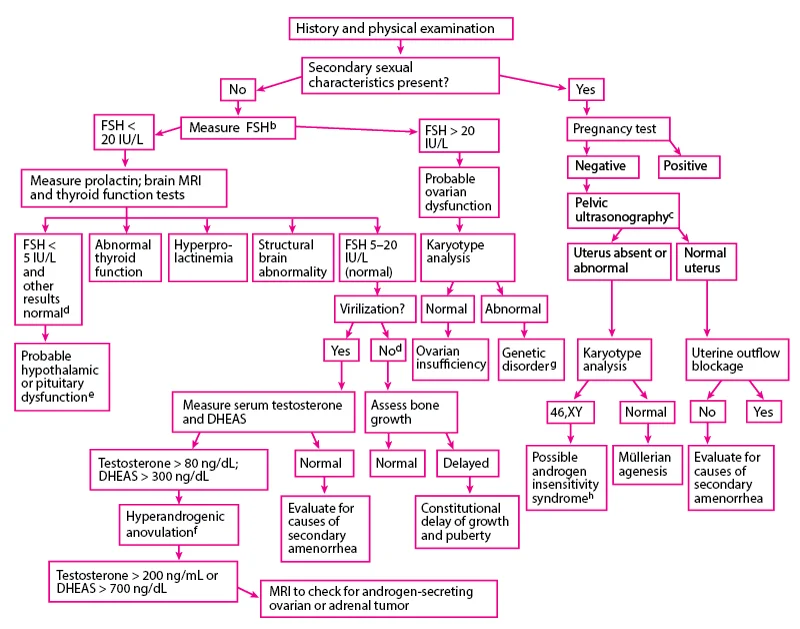
Evaluation of Amenorrhea
- Rule out pregnancy, as both primary and secondary amenorrhea require an immediate evaluation for pregnancy.
- Use a systematic approach:
Evaluating each critical component of menstruation: hypothalamus.
- Pituitary.
- Ovaries.
- Uterus.
- and genital outflow tract.

