Dysmenorrhea Seminar
By:
- Yaman Mardini
- Omar Badughaysh
- Abdullah Bohairi
Guided by: Dr. Mona Ahmed
Epidemiology:
- 50% of all menstruating women are affected by dysmenorrhea
- 90% of 1ry dysmenorrhea occur within first 2y of menarche
- Endometritis affects 10% of reproductive age – 50% of infertile
- Fibroids: 40–60% by age 35 (especially in African descent)
- PID affects 8% in sexually active women
- Polyps: 10–24% in women with abnormal uterine bleeding
Definition:
Refers to the pain associated with menstruation
Types & Pathophysiology
-
1ry: Occurs without an underlying medical condition. It is often linked to hormonal changes during menstruation, particularly the increase in prostaglandins, which cause uterine contractions. - Pain is primarily due to the release of prostaglandins during menstruation. Prostaglandins cause the uterus to contract, which can lead to reduced blood flow to the uterus, causing ischemia (lack of oxygen) and pain. The increased levels of prostaglandins contribute to uterine hypercontractility, which is often felt as cramping pain. This pain typically peaks at the beginning of the menstrual period and usually decreases as menstruation progresses.
-
2ry: caused by underlying conditions like endometriosis, fibroids, or pelvic inflammatory disease. It typically develops later in life. - The pathophysiology here involves underlying conditions.
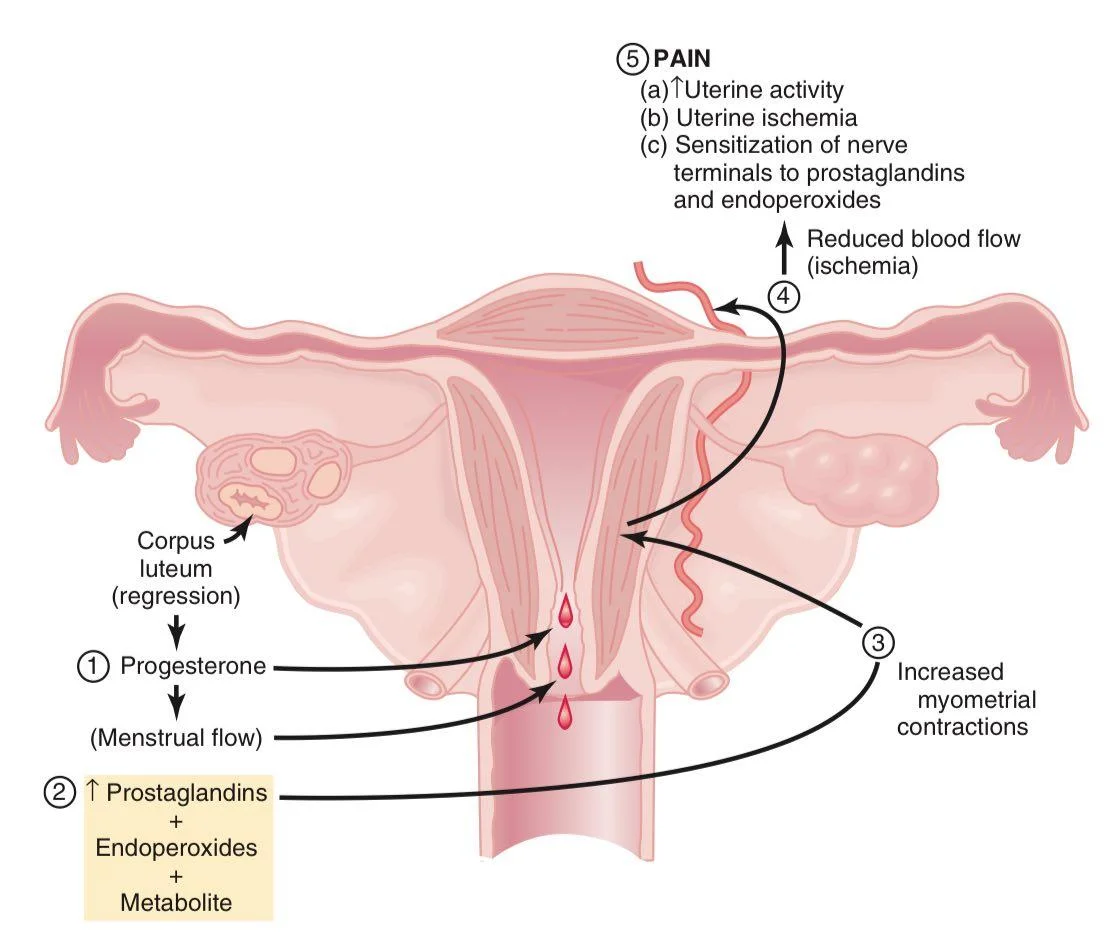
PAIN Mechanism:
- Progesterone (Menstrual flow)
- ↑ Prostaglandins + Endoperoxides + Metabolite Z
- Increased myometrial contractions
- Reduced blood flow (ischemia)
- PAIN
- (a) ↑Uterine activity
- (b) Uterine ischemia
- (c) Sensitization of nerve terminals to prostaglandins and endoperoxides
Etiology:
Secondary Dysmenorrhea:
- Endometriosis: Implantation of endometrial tissue outside uterine cavity.
- Adenomyosis: Where endometrial tissue extends into the myometrium.
- Pelvic inflammatory disease (PID): Infection causing chronic inflammation.
- Cervical stenosis and hematometra: Obstructed outflow of menstrual blood causing retained blood and pressure.
Characteristics of Primary Dysmenorrhea:
- S: Lower abdomen
- O: Sudden
- C: Cramp like
- R: Back – Inner thighs
- A: Nausea – Vomiting – Fatigue – Headache
- T: 2h before or just after menstruation
- E: NSAIDs relief symptoms
- S: 5 – 7 out of 10
-ve findings on exam
Sign of 1ry
±
2w prior – 1w after
Sign of 2ry
Investigation:
- CBC
- Ultrasound
| Etiology | ESR CRP | US | CS | Laparos copy | MRI | Swab / Biopsy |
|---|---|---|---|---|---|---|
| Endometriosis | Chocolate cyst | Gold | Deep lesion | |||
| Adenomyosis | Bulky uterus | Gold | ||||
| Fibroids | Well defined mass | |||||
| PID ± fluid Z | Douglas pouch | + | ||||
| Polyps | SIS | Diagnostic |
Iatrogenic Cause:
IUD (Copper)* ↑ PGs 20%
Management:
Primary Dysmenorrhea:
- Reassurance
- NSAIDs (2 – 3 days before flow)
- Contraceptive measures (OCP – Patches – Rings)
- Progestogens
Secondary Dysmenorrhea:
- Treat the underlying disease
- NSAIDs – Analgesics (useful)