Fetal Growth Restriction
Overview
Fetal Growth Restriction (FGR), also known as Intrauterine Growth Restriction (IUGR), occurs when a fetus does not grow at a normal rate inside the womb.
Definition
IUGR: When the birth weight of newborn infant is below the 10th percentile for a given gestational age
Low birth weight: (<2500 grams)
Small for Gestational Age (SGA) indicates that a fetus or neonate is below a defined reference range of weight for a gestational age.
Etiology of IUGR
Maternal Factors
-
Behavioral:
- Poor nutritional intake
- Cigarette smoking
- Drug abuse
-
Medical:
- Hereditary thrombophilia
- Early cardiovascular disease
- Hypertension
- Diabetes
- Obesity (associated with leptin resistance)
- Alcoholism
- Cyanotic heart disease
- Pulmonary insufficiency
- Antiphospholipid syndrome
Other Factors
-
Teratogen Exposure: Exposure to harmful substances during pregnancy.
-
Extreme Maternal Age: Being at the extremes of reproductive age.
-
Fetal Factors:
- Intrauterine infection (listeriosis and TORCH)
- Congenital anomalies
-
Placental Factors:
- Poor implantation
- Placenta previa
- Umbilical cord abnormality (Mcikeymouse, 2 artery, 1 vein normally, single down usually)
Types of IUGR
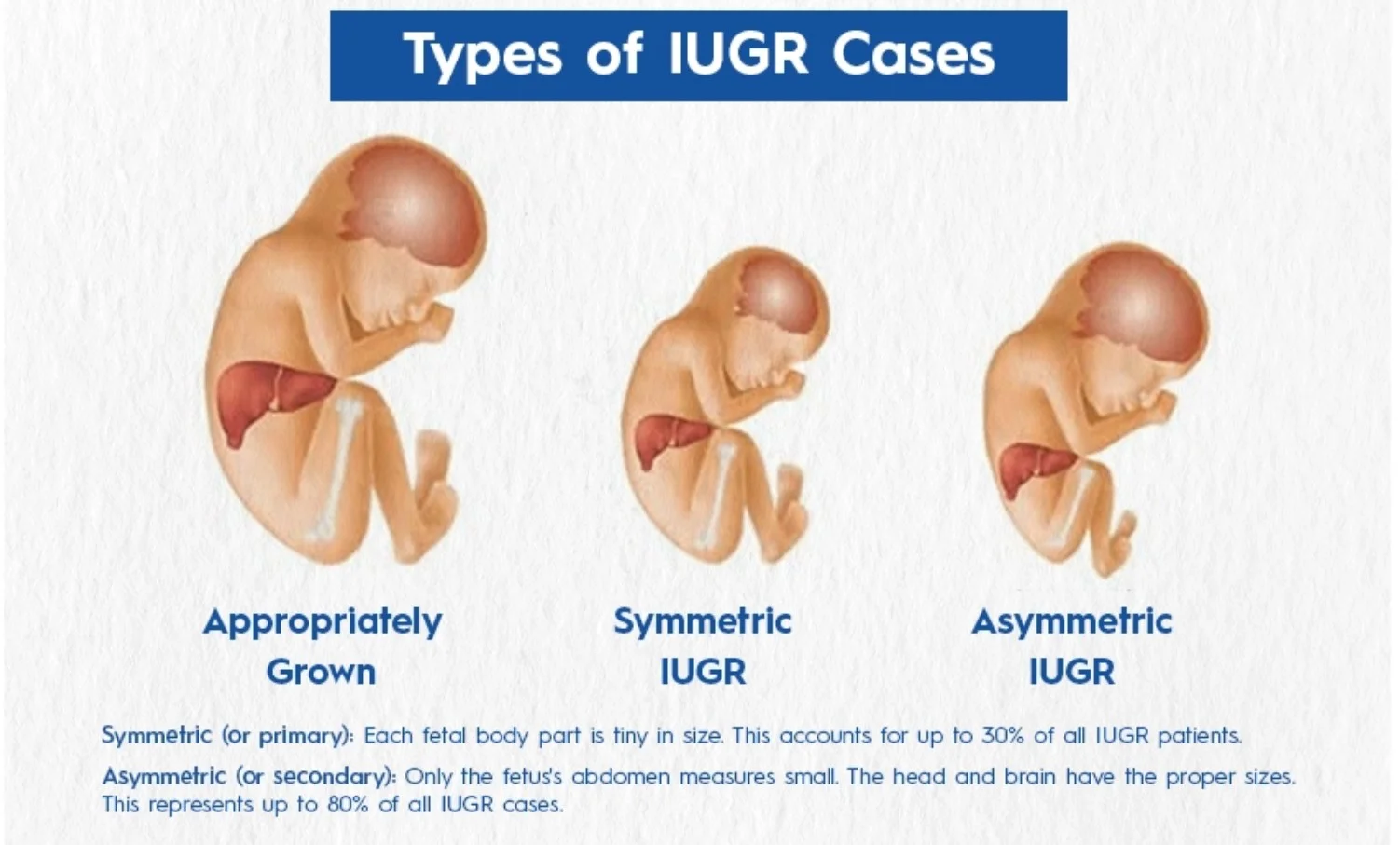
Symmetric vs. Asymmetric IUGR
- Symmetric (or Primary) IUGR: Each fetal body part is tiny in size, accounting for up to 30% of all IUGR patients.
- Asymmetric (or Secondary) IUGR: Only the fetus’s abdomen measures small, with the head and brain having proper sizes, representing up to 80% of all IUGR cases.
Classification Based on Gestational Age
- Early FGR: Less than 32 weeks.
- Late-Onset FGR: Diagnosed at or after 32 weeks.
Diagnosis
- Serial uterine fundal height measurements: Fundal height lags more than 3 cm behind expectations.
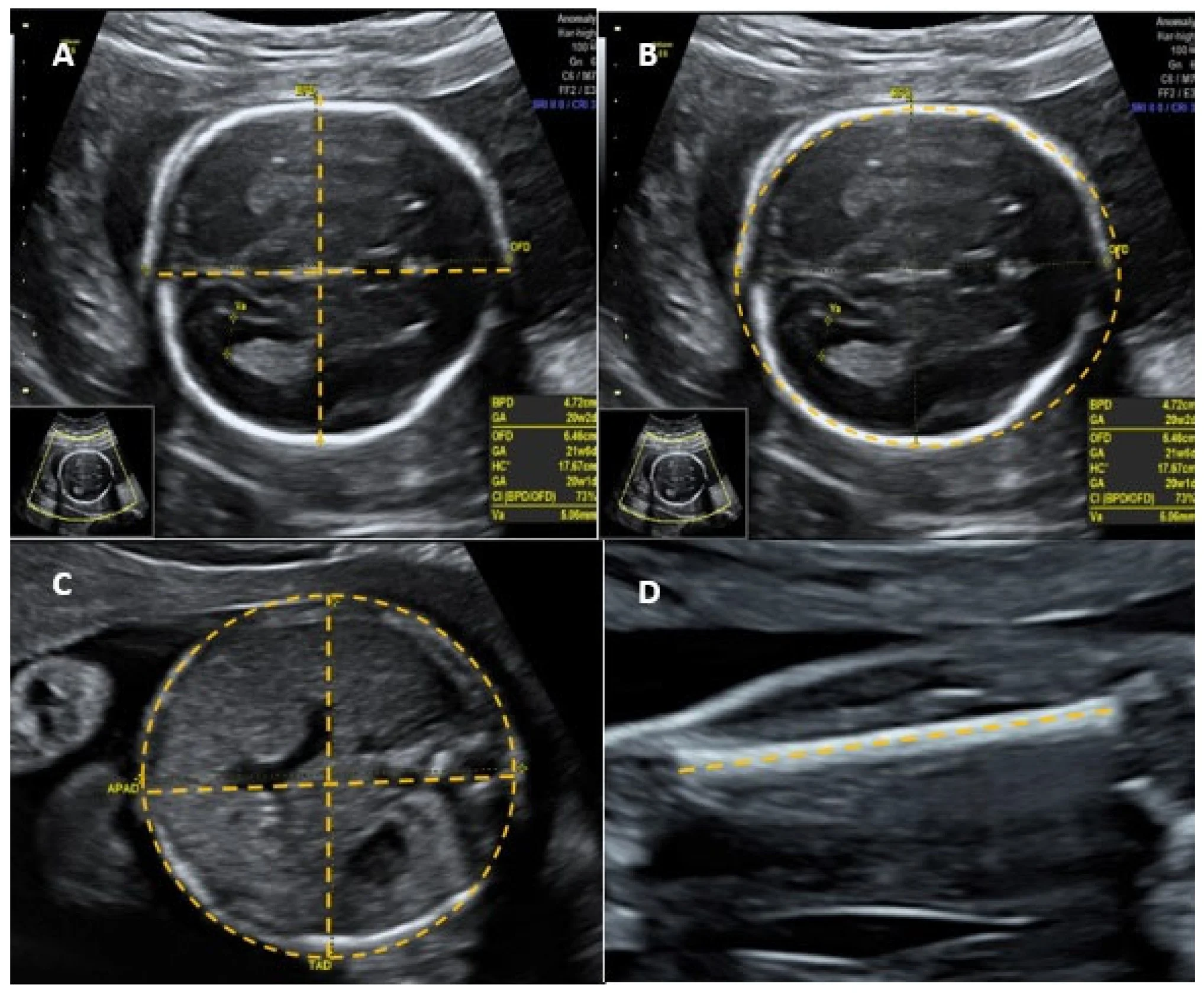
- Ultrasound:
- Fetal biometry: biparietal diameter (BPD), head circumference, abdominal circumference, femoral length, calculated fetal weight.
- Amniotic fluid volume. (index 5-25; divide abdomen in four, no fetal or cord part, measure. vertical from four areas, take ratio of total of >25 poly <5 oligio //// - >8 poly <2 olig pockets of air)
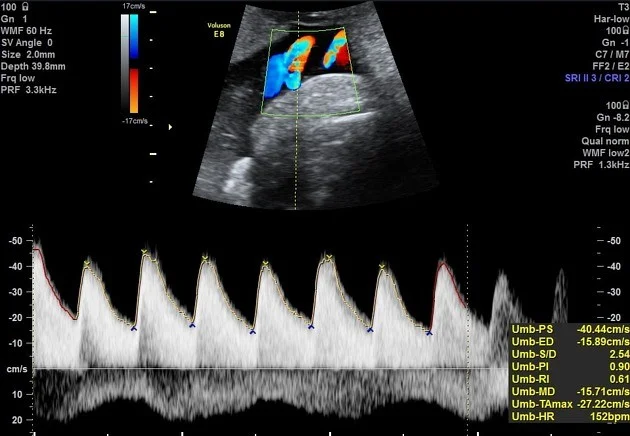
- Umbilical artery Doppler: low, absent, or reversal of diastolic flow.
Ultrasound Images of a Fetal Head
Umbilical Artery Doppler Ultrasound
 FGr at term deliver, before 37wk, assess doppler if abnormal deliver
FGr at term deliver, before 37wk, assess doppler if abnormal deliver
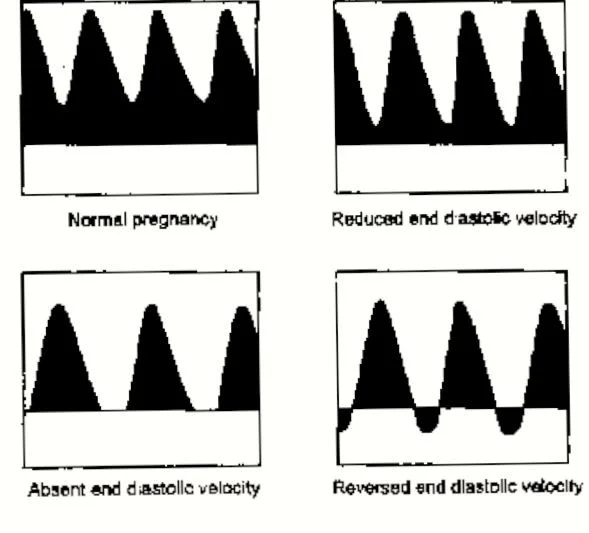
Progression of Umbilical Artery Doppler Changes
- Normal pregnancy
- Reduced end diastolic velocity
- Absent end diastolic velocity
- Reversed end diastolic velocity (Dexamethasone + Deliver now)
Key Diagnostic Parameters
- Abdominal circumference is the single most effective parameter for predicting fetal weight. Z
- Maternal lab tests: serology, amniocentesis.
Management
Pre-Pregnancy
- Stop smoking and alcohol consumption.
- Improve nutrition.
- Aspirin 81mg/day. z
Antepartum
- Stop smoking.
- Improve nutrition.
- Work leave. z
- Teach the patient about fetal kick count. z
- Hospitalization. (if absent fetal kick or reduced, if doppler is absent must be done twice week in such patient, medically unstsable, severe IUGR, if patient lives far away-;, biophysical profile is done)
Monitoring
- Twice-weekly nonstress test (NST) and biophysical profile (U/S, fetal movement, breathing, amniotic fluid, gross movement, ). - modified (Amniotic fluid index + CTG) - normal 8-10 - 4-6 suspicious, <4 abnormal CC?
- Umbilical artery Doppler weekly.
Labor and Delivery
Treatment of a fetus with suspected IUGR hinges on the clinical context, especially gestational age.
-
Gestational age < 34 weeks – administer a course of antenatal corticosteroids to promote lung maturation.
-
IUGR itself is not a contraindication to induction of labor; however, maintain a low threshold for proceeding to caesarean section if maternal or fetal status warrants.
Complications
- Increased chance of C-section and early birth.
- Breathing and feeding issues during birth.
- Hypoxia.
- Hypoglycemia.
- Having trouble regulating body temperature.
- Meconium aspiration.
- Polycythemia.
- Infection.
- NICU admission.
Clinical Scenarios Z
Case 1
 -D 2-3 weeks difference in size estimatino, doppler twice weekly or once
-D 2-3 weeks difference in size estimatino, doppler twice weekly or once
Case 2
 -A basic = fetal biomentry
-A basic = fetal biomentry
biometry initially, biophysical detailed.