Preterm Premature Rupture of Membranes (PPROM)
Definition
Preterm premature rupture of membranes (PPROM) is defined as premature rupture of membranes before 37 completed weeks.
Risk Factors for PROM
- Increasing friability/decreased tensile strength of membranes mainly due to infections like bacterial vaginosis Z.
- Polyhydramnios
- Multiple pregnancy
- Cervical incompetence
- Previous H/O PROM
Diagnosis
- Frank leakage
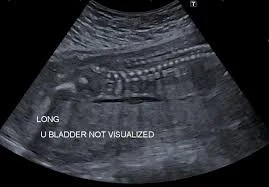
- Ultrasound
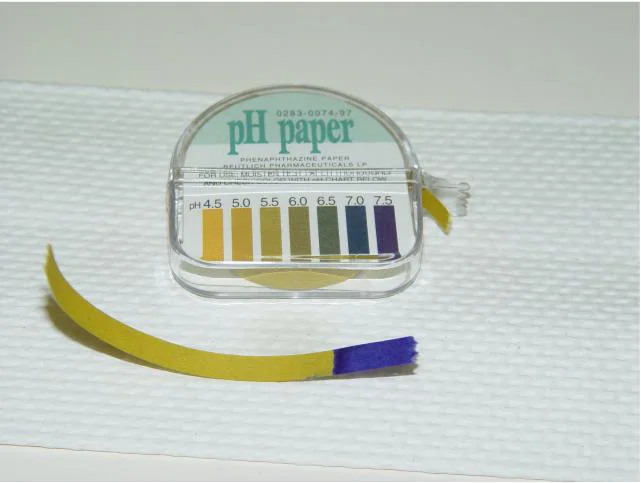
- Nitrazine test
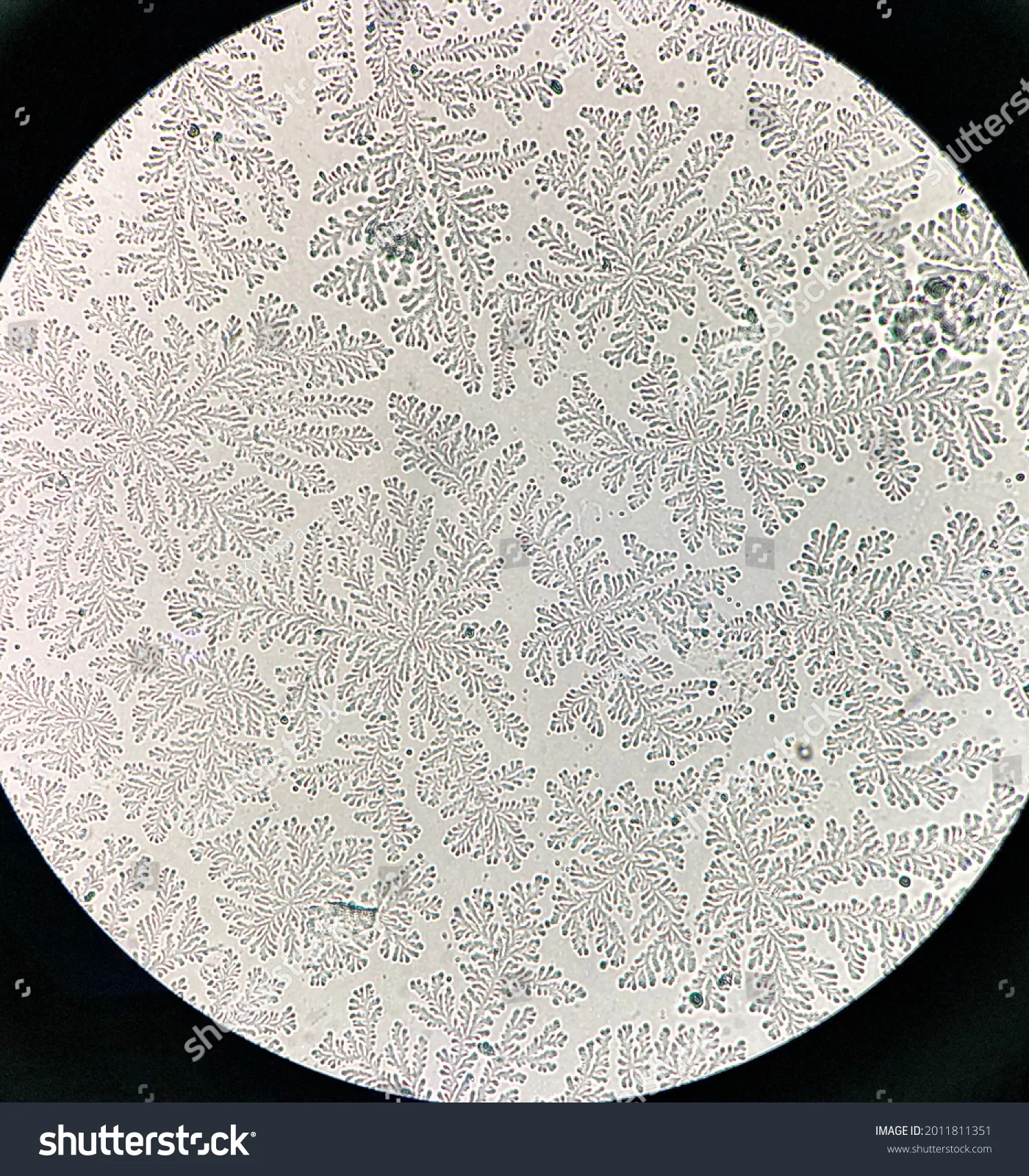
- Ferin test
- Fibronectin

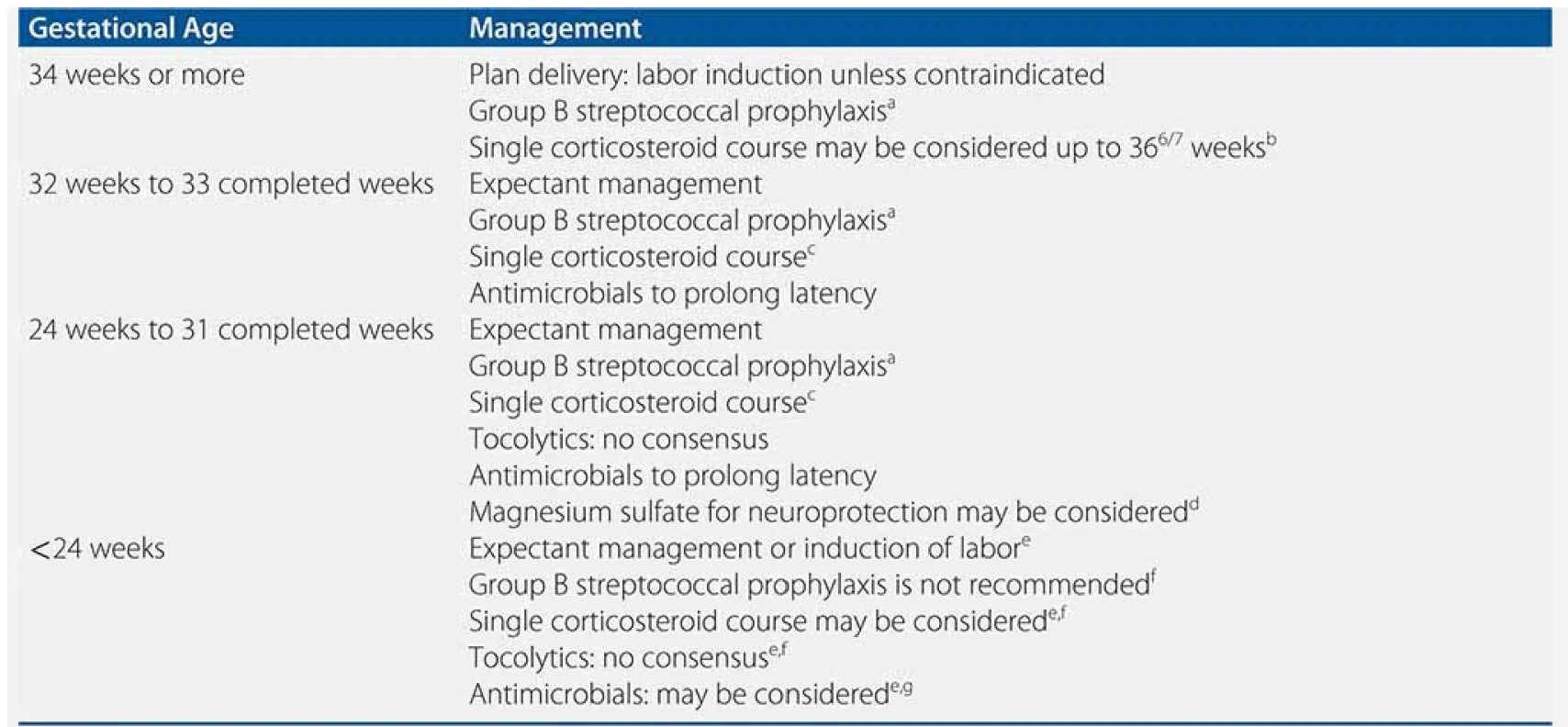
Management Based on Gestational Age Y
34 weeks or more
- Plan delivery: labor induction unless contraindicated
- Group B streptococcal prophylaxis[^1]
- Single corticosteroid course may be considered up to weeks[^2]
32 weeks to 33 completed weeks
- Expectant management
- Group B streptococcal prophylaxis[^1]
- Single corticosteroid course[^3]
- Antimicrobials to prolong latency
24 weeks to 31 completed weeks Y
- Expectant management
- Group B streptococcal prophylaxis[^1]
- Single corticosteroid course[^3]
- Tocolytics: no consensus
- Antimicrobials to prolong latency
- Magnesium sulfate for neuroprotection may be considered[^4]
<24 weeks
- Expectant management or induction of labor[^5]
- Group B streptococcal prophylaxis is not recommended[^6]
- Single corticosteroid course may be considered[^5][^6]
- Tocolytics: no consensus[^5][^6]
- Antimicrobials: may be considered[^5][^7]
Antenatal Corticosteroids (ACS)
Drugs
- steroids
- Betamethasone (12 mg Q24h × 2 doses)
- Dexamethasone (6 mg Q12h × 4 doses)
Mechanism
- Accelerates development of type 1 and type 2 pneumocytes
- Stimulates the synthesis and release of surfactant
- Induces airway epithelial sodium channel gene expression
Benefits for Newborn
- Decrease incidence of respiratory distress
- Decrease need for respiratory support
- May decrease duration of NICU/special care nursery stay
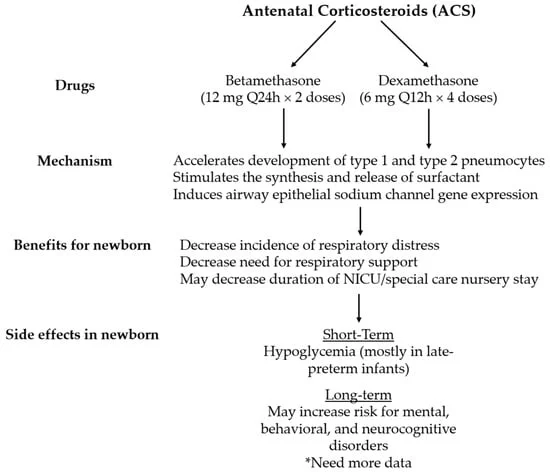
Side effects in newborn shorterm: Hypoglycemia in late-preterm infants Longterm: May increase risk for mental behavioral and neurocognitive disorder
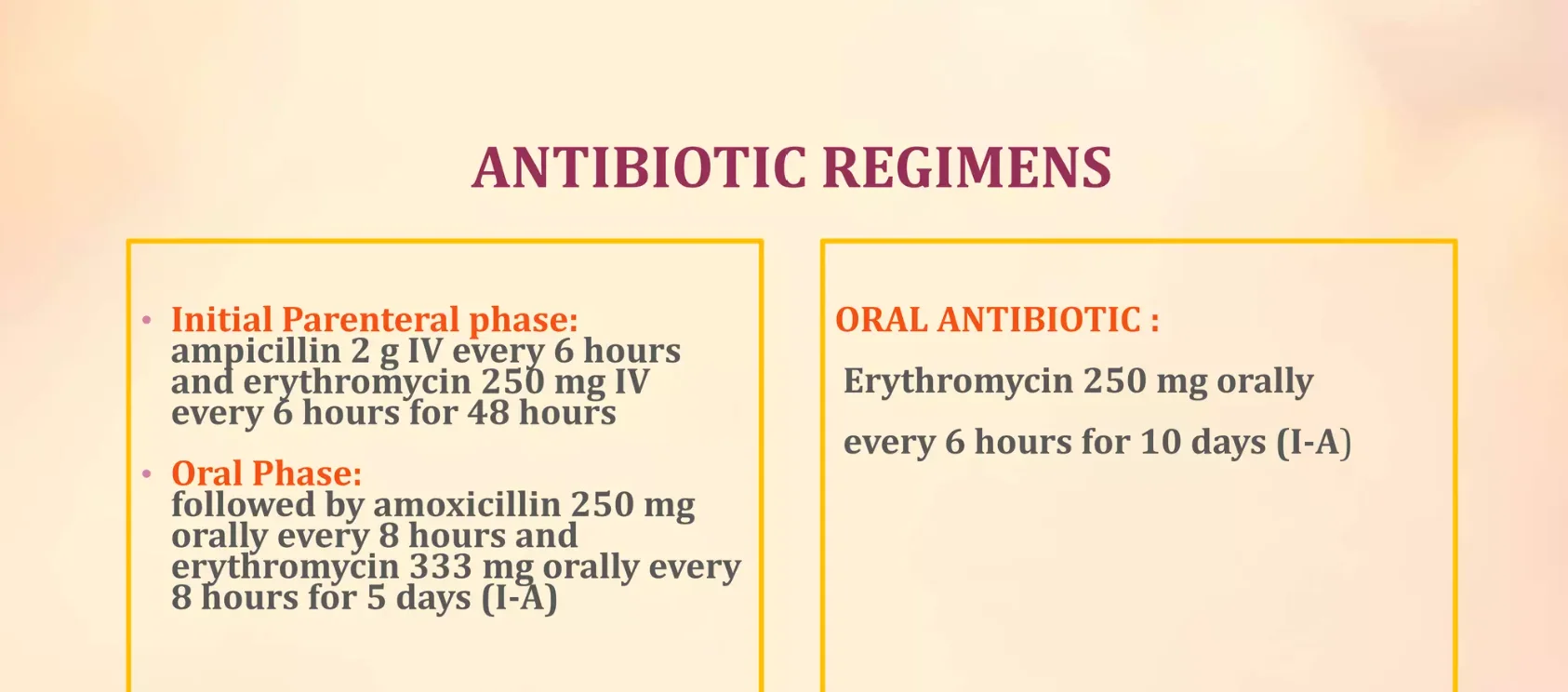
Antibiotic Regimens
Initial Parenteral Phase:
- Ampicillin 2 g IV every 6 hours and erythromycin 250 mg IV every 6 hours for 48 hours
Oral Phase:
- Followed by amoxicillin 250 mg orally every 8 hours and erythromycin 333 mg orally every 8 hours for 5 days (I-A)
Oral Antibiotic:
- Erythromycin 250 mg orally every 6 hours for 10 days (I-A)
Why We Give Antibiotics
- Protects against infection-related complications.
- Prolongs the pregnancy course.
- Reduces preterm-related morbidity and mortality.