Obstetric Abdominal Examination

Before Examination
- Explain to the patient the need, nature, and purpose of the examination.
- Obtain verbal consent.
- The examiner should be accompanied by another female.
- Respect her privacy and examine in a private room.
- Expose only the relevant part of the examination.
- Ensure the patient is comfortable and warm.
- Ask the patient to empty her bladder.
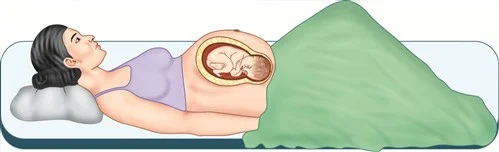
Patient Positioning
- Patient should lie in the dorsal position.
- Stand to her right.
- Roll her slightly to the left (to decrease vena cava compression).
- Ask about any tender area before palpation.
General Examination
- Vital signs
- Weight
- Height
- Gait
- Face
- Skin
- Eyes
- Neck
- Breast
- Hands
- Legs
Vital Signs
- Blood pressure: Chronic hypertension, Gestational hypertension.
- Pulse rate/Heart rate (increased): Haemic murmur.
- Respiratory rate: Usually unaffected, slight increase (diaphragm raise).
- Temperature (increase due to increase MR)



Weight and Height
-
Weight: Abnormal (obesity, underweight, overweight, emaciation). Check every visit. Weight gain (11-16 kgs); at 2nd or 3rd trimester.
-
Height: Short stature (small pelvis).
Skin, Face, and Eyes
Face:
- Appearance
- Psychological status
- Diseases (thyrotoxicosis).
- Hyperpigmentation (chloasma).
Eyes
- Pallor
- jaundice cyanosis.
Tongue
- Pallor
- dehydration
- stomatitis
- jaundice
 Hyperpigmentation (chloasma).
Hyperpigmentation (chloasma).
Neck, Breast, Hands, and Legs
- Neck: JVP, Thyroid, Hyperpigmentation (acanthosis nigricans), Dilated veins, Lymph nodes.
- Breast: Enlarged in size, 2ry areola, Montgomery’s gland, Redness, Vascular engorgement, Colostrum, Cracked or fissure nipple.
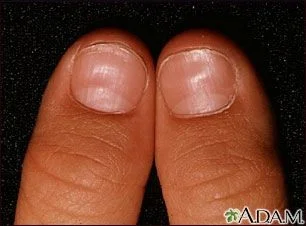
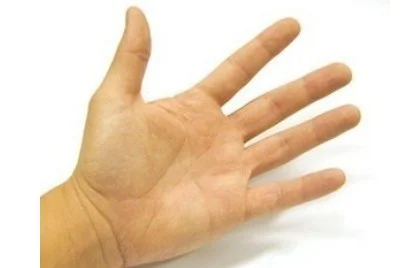
- Hands: Nails (clubbing, spooning (koilonychia), cyanosis), Palms (Pallor, Palmer erythema, spider navi).
- Legs: Varicose vein, Oedema ± causes; (Physiological, Preeclampsia, Anaemia, Heart failure, Nephrotic syndrome).










General Systemic Review
- CNS
- GIT
- Urinary system
- Locomotor system
Abdominal Examination
Can be examined in three parts:
- Inspection
- Palpation
- Auscultation
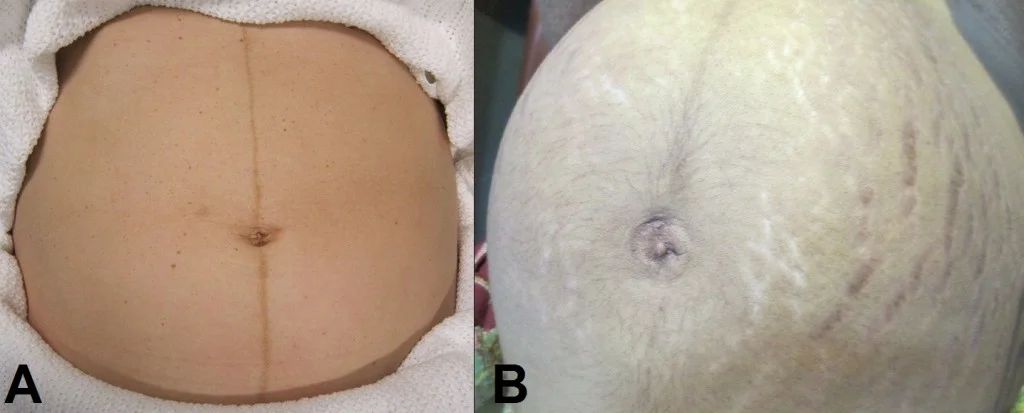
Inspection
- Skin of the abdomen
- Linea nigra
- Striae gravidarum
- Dilated veins
- Umbilicus (flat, inverted, everted)
- Fetal parts
- Skin conditions



Inspection Details
- Size of uterus
- Shape of uterus
- Fetal movement
- Scars
- Herniation

Palpation
- Superficial palpation: AF, Organomegaly, Uterine contractions.
- Deep palpation
What the Examiner Should Identify
- First fundal grip
- Second fundal grip
- Lateral grip
- Fetal heart auscultation
- First pelvic grip
- Second pelvic grip
- Vaginal examination (if indicated)

1. Fundal Height (1st Fundal Grip)
-
Keep the ulnar border of the curved left hand on the woman’s abdomen parallel to the symphysis pubis.
-
Start from the xiphisternum and gradually proceed towards the symphysis pubis, lifting the hand between each step till a bulge/resistance of the uterine fundus is felt.
-
Mark the level of the fundus.

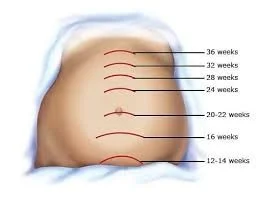
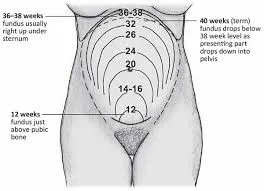
Fundal Height (FH) ≈ Gestational Age (weeks) after ~20 weeks
The fundal height is measured in centimeters (cm) from the upper edge of the pubic bone to the top of the uterus (the fundus). After about 20 weeks of pregnancy the measurement generally correlates with the gestational age in weeks, with a typical variance of ± 2 cm.
Below is the commonly used reference table (rounded to whole centimeters). Values are median expected FH; actual measurements may fall 1–2 cm above or below and still be normal.
| Gestational Age (weeks) | Expected FH (cm) | Typical Range (cm) |
|---|---|---|
| 12 | 10 | 9 – 11 |
| 14 | 12 | 11 – 13 |
| 16 | 14 | 13 – 15 |
| 18 | 16 | 15 – 17 |
| 20 | 20 | 18 – 22 |
| 22 | 22 | 20 – 24 |
| 24 | 24 | 22 – 26 |
| 26 | 26 | 24 – 28 |
| 28 | 28 | 26 – 30 |
| 30 | 30 | 28 – 32 |
| 32 | 32 | 30 – 34 |
| 34 ** | 34** | 32 – 36 |
| 36 | 36 | 34 – 38 |
| 38 | 38 | 36 – 40 |
| 40 | 40 | 38 – 42 |
| Interpret |
- **Within range** – growth is proceeding normally.
- **> 2 cm above** – consider macrosomia, polyhydramnios, or over‑estimation of dates.
- **> 2 cm below** – consider intra‑ uterine growth restriction (IUGR), oligohydramnios, or under‑estimation of dates.
Estimating Gestational Age from Fundal Height
- Measurement of fundal height: Divide the abdomen by imaginary lines passing through the umbilicus.
- Divide the lower abdomen into 3 parts with 2 equidistant lines between the pubic symphysis and the umbilicus.
- Divide the upper abdomen into 3 parts again with 2 imaginary equidistant lines between the umbilicus and xiphisternum.


Significance of Fundal Height
Indicates:
- Duration of pregnancy
- Fetal growth
- Any abnormality in the pregnancy
Reasons for Fundal Height Less or More Than Date
- Less than date: Wrong date, IUGR, Missed abortion, IUD, Transverse lie, Deep engagement, Oligohydramnios.
- More than date: Wrong date, Polyhydramnios, Macrosomia, Multiple pregnancy, Placenta previa, Tumours, Hydrocephalus, Molar pregnancy.
Leopold Maneuvers
2. 2nd Fundal Grip (Leopold I)
Using two hands and compressing the maternal abdomen till a sense of the fetal part is reached.
This determines which part of the baby is occupying the fundus.
How to identify head? Hard smooth , rounded .
How to identify breech?
Soft irregular broad.

3. Lateral Grip (Leopold II)
- To detect the lie.
- To detect the fetal back (hard, regular).
why?
- To determine the scapula to
- know where to put the sonic aid
- (hearing Fetal heart sound).
How ?
- The sides of the uterus are palpated to determine the
- position of the Fetal back.(hard regular)

4. Detect Fetal Heart
- Below umbilicus if cephalic presentation.
- Above umbilicus if breech presentation.
How to measure?
- Pinnards stethoscope.
- Regular sthesoscope.
- Ultrasound.
- Doppler machine.
- CTG machine.

5. First Pelvic Grip and 6. Second Pelvic Grip
- To determine which part of the fetus is occupying the pelvis.
- To determine engagement.

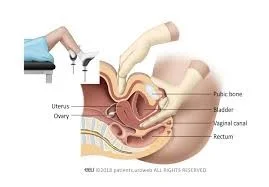
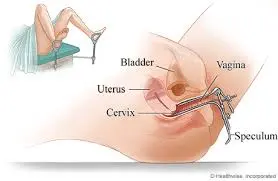
Vaginal Examination (PV)
- Patient should be in the lithotomy position.
How to Perform
- Bimanual examination.
- Speculum examination.
Vaginal Examination In Pregnancy
Bimanual examination is no longer a routine part of antenatal examination but still sometimes required: 1. To assess maturity in early pregnancy
-
To exclude suspected abnormalities such as incarcerated retroversion of the uterus or ovarian tumor.
-
To identify a presenting part this cannot be confidently identified abdominally.
-
To exclude or confirm gross degrees of contraction (in very small patients).
5. To assess the ripeness of the cervix near term.
6. To assess pelvic cavity.
Suspicion of multiple pregnancy - an abdominal examination
-
An unexpectedly large uterus for the estimated gestational age
-
Multiple Fetal parts felt on abdominal palpation
-
FHS is heard at more than one place.
-
Poly hydramnios.
To Summarize
Abdominal Examination is done for:
- Fundal height
- Fetal lie and presentation
- Fetal movement
- Fetal heart sounds
- Any other abdominal finding