Infection & Tumors in Orthopedics
Instructor: Dr. Tarif Al Akhras
Case 1: Pediatric Elbow Infection (6 years old)
Clinical Presentation
- Localized tenderness
- Hotness and local redness
- Swelling and edema
- Reduced range of motion of the elbow

Differential Diagnosis
- Osteomyelitis
- Cellulitis
- Septic arthritis
- Both septic arthritis and osteomyelitis (can occur simultaneously, especially proximal femur and hip)
- Ewing sarcoma

Laboratory Investigations
- Complete Blood Count (CBC): Leukocytosis with neutrophilia
- C-reactive protein (CRP): Raises very early in infection
- Erythrocyte Sedimentation Rate (ESR): Raises several days later
- Blood culture: Identify causative organism
- Aspiration from sub-periosteal collection or joint:
- Gram stain
- Culture and sensitivity testing
Aspiration Fluid Analysis
- Clear colorless: Normal
- Clear yellow (can read through): Non-inflammatory
- Turbid: Inflammatory
- Pus: Bacterial infection
- Blood: Hemorrhagic or traumatic tap

Imaging Studies
- X-ray: First signs appear at 10-14 days
- Metaphyseal rarefaction
- Periosteal reaction (new bone formation)
- Bone Scan: Detects early signs of infection
- MRI: Shows area of affection (joint vs. metaphysis vs. both)

Note: MRI is perfect for detecting early signs of infection, replacing bone scan in many cases.
Treatment Protocol
- Supportive treatment: Pain management and hydration
- Splint immobilization: To prevent further damage
- Antibiotic therapy:
- I.V. flucloxacillin (must start early after aspiration)
- Consult microbiologist for optimal antibiotic selection
- Modify based on culture and sensitivity results
- Surgical intervention: Debridement and drainage as needed
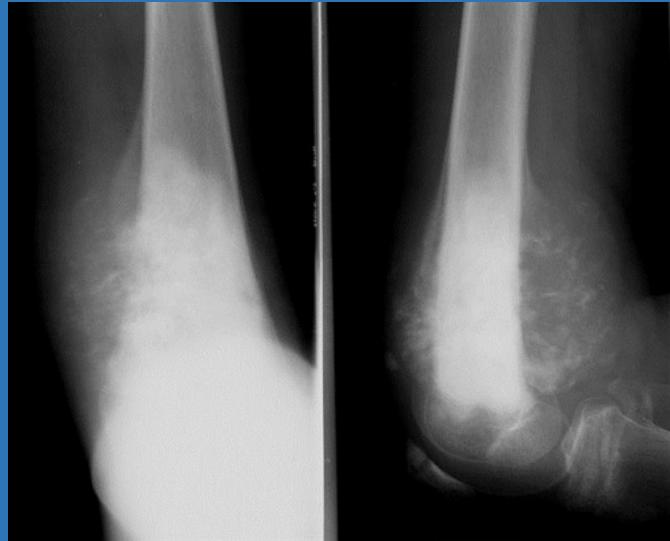
Case 2: Distal Femur Mass (16 years old)
Clinical Presentation
- Painless swelling at the distal right femur
- No inflammatory signs
- No general systemic symptoms

Initial Workup
- X-ray imaging of the distal femur

Diagnosis: Osteochondroma (Exostosis)
Clinical Features
- Bony exostosis projecting from the external surface of a bone
- Usually has a hyaline cartilaginous cap
- Most are asymptomatic
- Common complaint: Hard palpable mass
- Symptoms arise due to:
- Location
- Size
- Pressure effects on adjacent structures
Complications
- Growth disturbance (in multiple lesions)
- Malignant transformation (Rare in solitary lesions: 1%)
Management and Prognosis
- Observation for asymptomatic lesions
- Surgical excision for symptomatic or complicated cases
- Regular monitoring for potential malignant transformation
Case 3: Pathological Fracture (11 years old)
Clinical Presentation
- Pain in right arm after fall at home
- No significant medical history
- Incidental discovery of bone lesion on X-ray
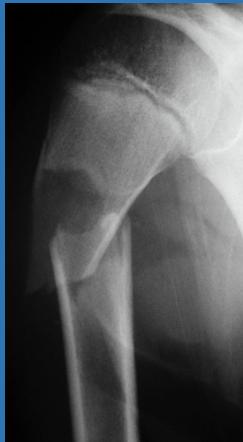

Diagnosis: Simple Bone Cyst
Characteristics
- Solitary (unicameral) lesion
- Children (typically 5-15 years)
- Metaphyseal location
- Not seen in adults
- Commonly discovered by pathological fracture
Treatment Options
- Observation: Cyst might heal spontaneously
- Multiple bone marrow injections
- Fracture fixation: Flexible intramedullary nailing
- Surgical curettage and bone grafting

Differential Diagnosis: Cyst-Like Lesions in Bone

Simple Bone Cyst
- Fills medullary cavity
- Does not expand bone

Aneurysmal Bone Cyst
- Located at metaphyseal side of physis
- Expansile lesion

Giant Cell Tumor
- Occurs after physeal fusion
- Extends to sub-articular region
Case 4: Aggressive Bone Tumor (18 years old)
Clinical Presentation
- Painful mass at right femur
- Limited knee joint motion
- History of trauma 8 weeks prior (simple fall at home)
- Initially diagnosed as simple contusion by primary care physician
Radiographic Findings
- Radiolucency and sclerosis
- Poorly defined margins
- Extension into soft tissue
- Periosteal reaction:
- Sunburst (sun-ray) appearance
- Codman’s triangle
Diagnosis: Osteosarcoma
Staging Investigations
- CT chest:
- Mandatory staging study
- Evaluates for pulmonary metastasis
- MRI:
- Very informative, must include entire involved bone
- Determines soft tissue and marrow involvement
- Bone scan:
- Mandatory imaging study to discover skip lesions
- Always shows increased uptake
Treatment Protocol
- Metastasis workup:
- Well-planned incision for biopsy
- Neoadjuvant chemotherapy
- Surgical management:
- Wide resection
- Custom-made prosthesis reconstruction
- Adjuvant chemotherapy
Summary of Key Points
Infection vs. Tumor Differentiation
- Inflammatory signs (redness, heat, tenderness) → Infection
- Painless progressive swelling → Tumor
- Systemic symptoms → Consider malignancy
- Pathological fracture → Underlying bone lesion
Diagnostic Approach
- Clinical examination and history
- Laboratory studies (CBC, CRP, ESR)
- Imaging studies (X-ray, MRI, CT, bone scan)
- Biopsy when malignancy suspected
- Multidisciplinary management for optimal outcomes