Fracture Humerus

Proximal end fracture
- The head
- Greater tuberosity
- Lesser tuberosity
- Surgical neck

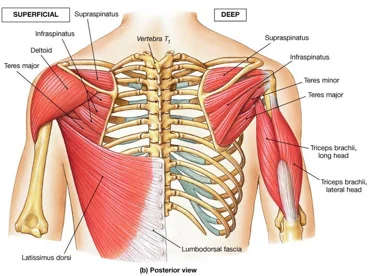
Greater Tuberosity
- Provides attachment to:
- Supraspinatus, infraspinatus, Teres Minor

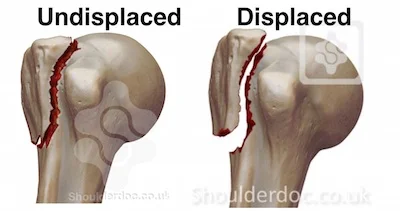
Greater Tuberosity
- Management:
- Minimally/non displaced:
- conservative Sling
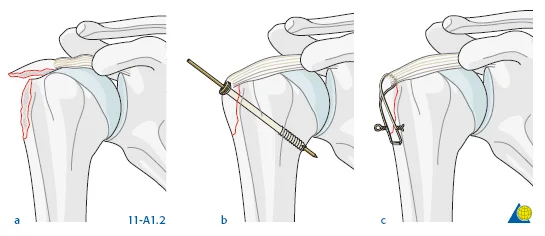
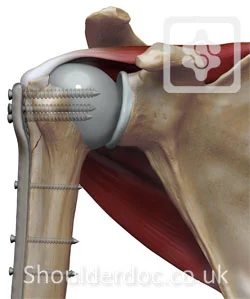
- Severely displaced: internal fixation
- By screws / tension band / plate
- To regain function of rotator cuff
- Minimally/non displaced:
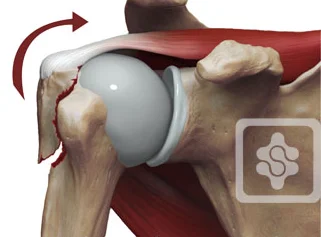
Surgical Neck- Problem
- If osteoporotic bone
- Difficult fixation
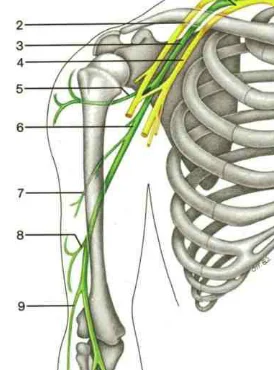
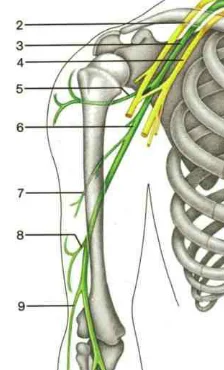
- Possible associated injury to Axillary nerve
- Motor: Deltoid
- Sensory: upper lateral arm

Humeral Shaft Fracture
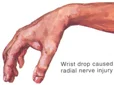
- Possible associated injury to The Radial nerve (why?)(signs?)


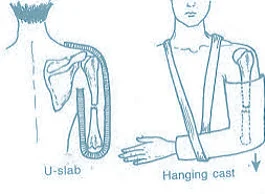
Humeral Shaft Fracture- Management
- Conservative: U-shape slab) / splint / orthosis
- Gravity maintains reduction

- Gravity maintains reduction
Humeral Shaft Fracture
- Management:
- Operative: (plate or IMN)
- Indications:
- Sever displaced Unreduced,
- Bilateral,
- multiple injuries
- floating elbow,
- Needs to use crutches
- Patients’ preference (active, athlete)



Fracture Distal Humerus
- Treated by open anatomical reduction and internal fixation by plates and screws
- Early mobilization to prevent elbow stiffness

