Scaphoid Fracture
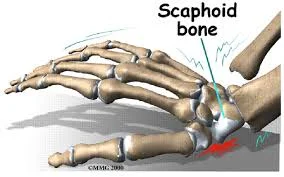
- Scaphoid is the common fractured carpal bone
- Fall on the palm of the outstretched hand
- Presents with pain, tenderness in the anatomical snuffbox

Scaphoid Fracture
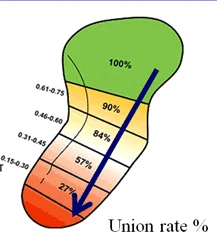
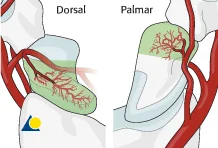
- Blood supply comes from distal to proximal
- Avascular necrosis (AVN) common with proximal 1/3 fracture
- Radiology:
- AP and Lateral not enough
- Need an special scaphoid view

Scaphoid Fracture
- Complications
- Avascular necrosis (AVN):
- Mainly proximal 1/3 fracture
- Non-union:
- In undiagnosed or undertreated scaphoid#
- Wrist osteoarthritis
- A result of non-union and AVN
- Avascular necrosis (AVN):
narrowing+ sclerosis


Scaphoid Fracture - Treatment
-
Not all fractures are apparent initially in image, If tenderness is present:
- Treat by thumb Spica cast
- Repeat x ray after 2 weeks
-
Non / minimally displaced waist & distal fractures
- Short arm thumb Spica
- Extend to16 weeks depending on fracture location
-
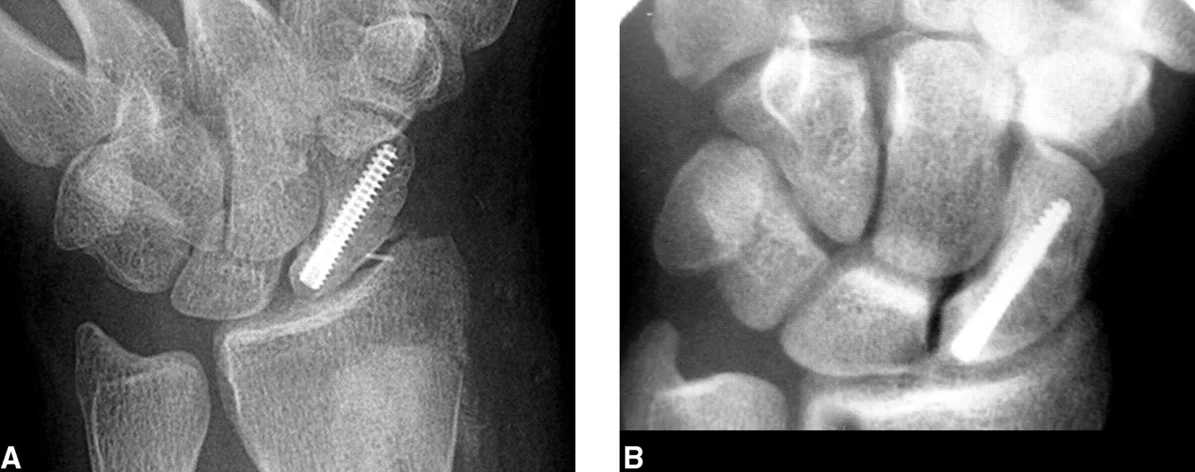
Displaced and proximal fractures
- Internal fixation with special screw

Metacarpal Fractures
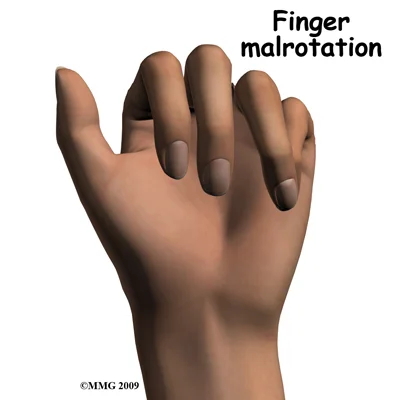
- Careful about rotational malalignment
- Check rotation by flexing the fingers
Finger malrotation

- Undisplaced / or only one MC
- Treatment by cast / or splint



- Displaced / Rotated / Multiple
- Treated by internal fixation (screws / plates / wires)




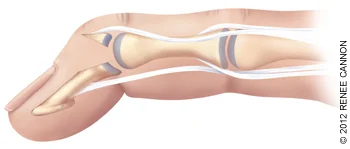
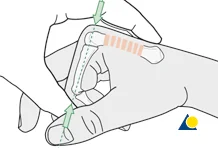
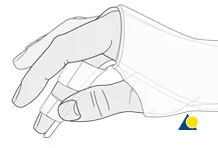
Mallet Finger
-
Avulsion injury of extensor tendons insertion to distal phalanx
-
Mechanism of injury
- Sudden forceful flexion (e.g. ball hits tip of finger)
-
Clinical picture
- Flexed distal IP joint
- Loss of active extension of DIP joint
-
Treatment
- Mallet finger splint
- Internal fixation if avulsed bone is large