Pediatric Neuromuscular Disorders
Author: Dr. Sultan Almisfer, MD Specialty: Pediatric Orthopedic Consultant


Cerebral Palsy
Definition
- Non-progressive injury to developing brain
- Leads to motor control and tone abnormalities
- Static brain injury, dynamic musculoskeletal manifestations
Epidemiology & Etiology
- Incidence: 2–3 per 1000 live births
- Causes: prematurity, hypoxic-ischemic injury, malformations, infections
Classification
- By tone: Spastic (most common), athetoid, ataxic, mixed
- By distribution: hemiplegia, diplegia, quadriplegia
- GMFCS I–V (functional classification)
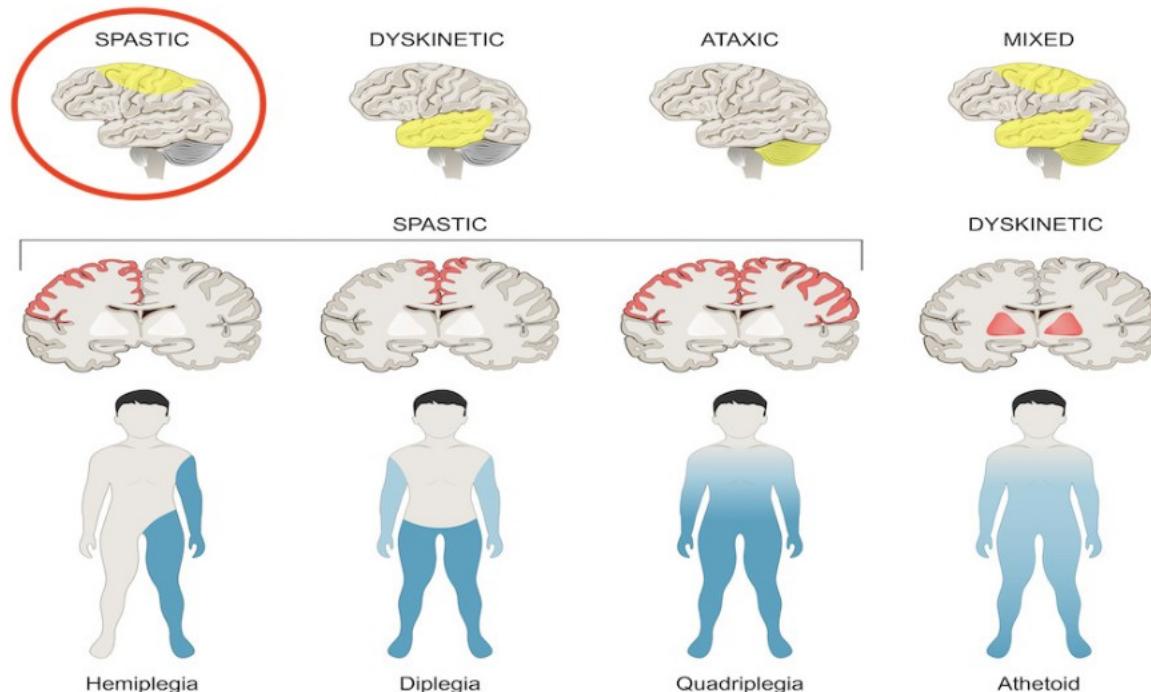
Classification Diagram
Tone Classification (Top Row):
- SPASTIC (Highlighted)
- DYSKINETIC
- ATAXIC
- MIXED
Distribution Classification (Bottom Row):
- SPASTIC (Corresponding to Hemiplegia, Diplegia, and Quadriplegia)
- DYSKINETIC (Corresponding to Athetoid)
Corresponding Body Maps:
- Hemiplegia: Spastic tone affecting one side of the body
- Diplegia: Spastic tone affecting the legs more than the arms
- Quadriplegia: Spastic tone affecting all four limbs
- Athetoid: Dyskinetic tone affecting the entire body
Clinical Features
- Spasticity, contractures, abnormal gait
- Hip subluxation/dislocation, scoliosis, foot deformities
- Associated problems: seizures, vision/hearing, cognition, swallowing issues
Management
- Multidisciplinary approach: PT, OT, orthotics, spasticity control
- Spasticity control: botulinum toxin, baclofen (oral/intrathecal)
- Surgical interventions: soft tissue releases, tendon transfers, osteotomies, SEMLS
- Selective dorsal rhizotomy (specialized cases)
Duchenne Muscular Dystrophy
Definition & Genetics
- X-linked recessive disorder; absence of dystrophin protein
- Onset: 2–6 years
Clinical Features
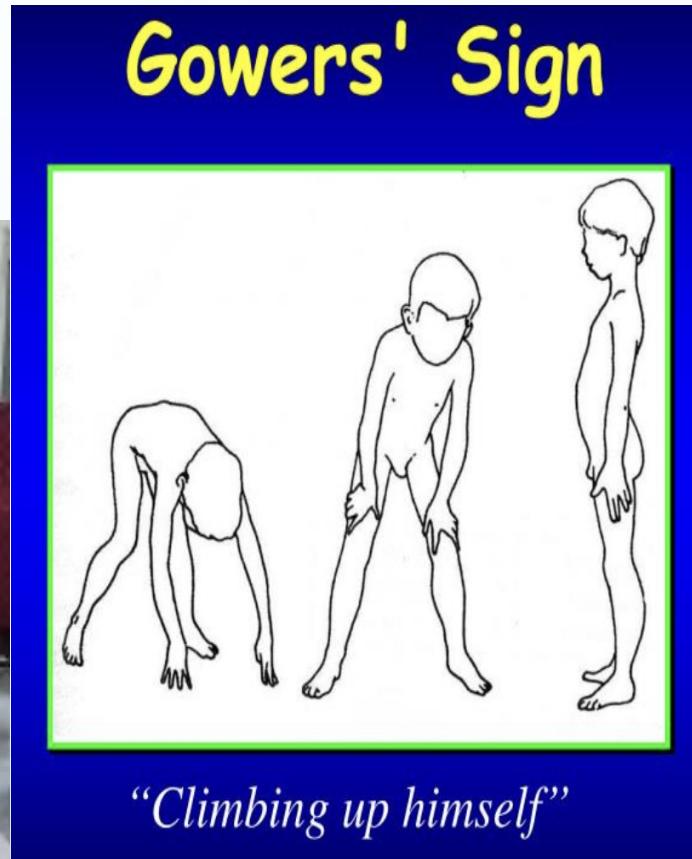
- Proximal muscle weakness, waddling gait
- Gower’s sign
- Calf pseudohypertrophy
- Contractures, scoliosis, cardiomyopathy, respiratory decline

Investigations
- CPK ↑ (10–200x normal)
- Genetic testing for dystrophin mutation
- Muscle biopsy if needed
- Echo & pulmonary function tests
Management
- Corticosteroids prolong ambulation
- Exon skipping therapies (eteplirsen)
- Cardiac medications, respiratory support, physical therapy
- Orthopaedic surgery: soft tissue releases, scoliosis fusion
Prognosis
- Without treatment: wheelchair by 12 years, death ~20 years
- With therapy: survival into 30s, prolonged ambulation
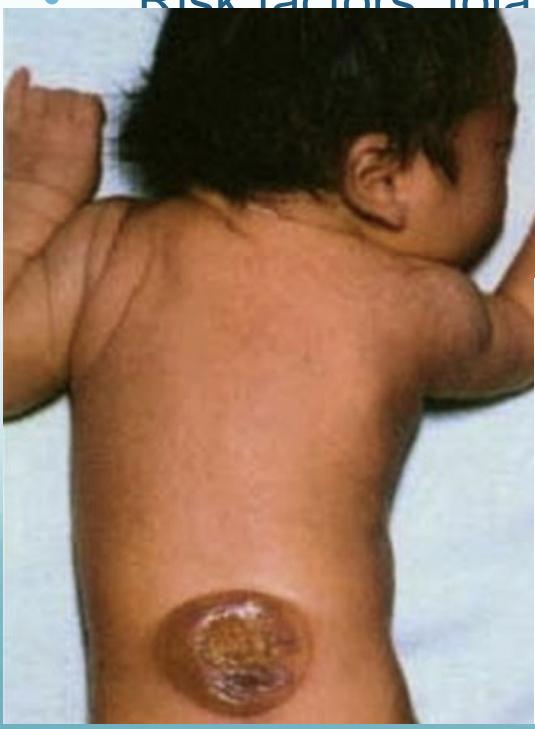
Myelodysplasia (Spina Bifida)
Definition & Etiology
- Failure of neural tube closure
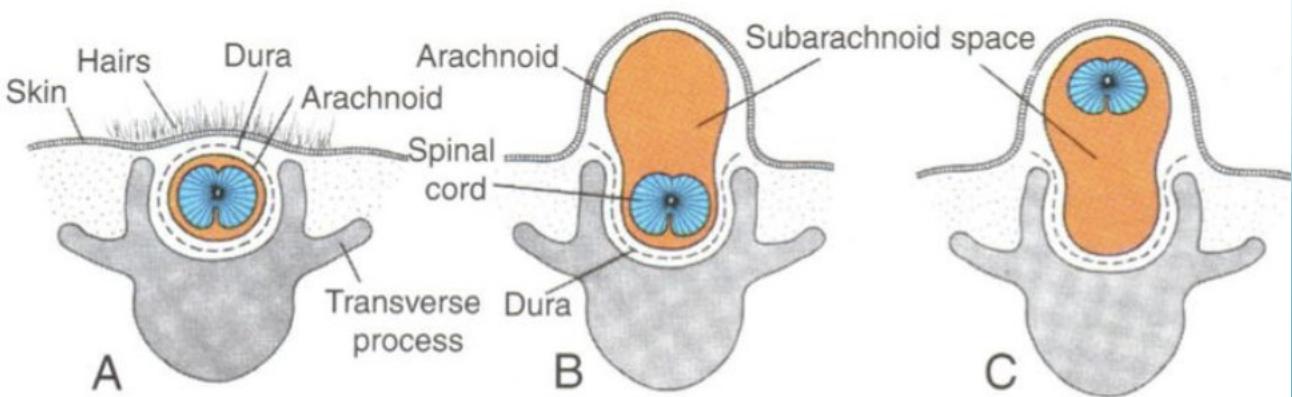
- Types: spina bifida occulta, meningocele, myelomeningocele
- Risk factors: folate deficiency, maternal diabetes, valproic acid
Clinical Features
- Orthopaedic: hip dislocation, foot deformities, scoliosis/kyphosis
- Neurologic: hydrocephalus, Chiari II, tethered cord
- Urologic: neurogenic bladder
Diagnosis
- Prenatal: ↑ AFP, ultrasound
- Postnatal: MRI spine, radiographs for deformities
Management
- Multidisciplinary: neurosurgery, orthopaedics, urology, rehabilitation
- Spine fusion for scoliosis/kyphosis
- Hip and foot surgery as needed
- Fracture care with caution (osteopenia, insensate limb)
Take-Home Messages
- Cerebral Palsy: static brain injury, spasticity, contractures
- Duchenne: progressive disease, steroids/gene therapy, scoliosis fusion
- Myelodysplasia: congenital defect, multisystem involvement
- Team care is essential: orthopaedics, neurosurgery, rehabilitation, urology, cardiology