Cardiac Arrest
Dr. Nasr Eldin Yousif Ahmed
https://next.amboss.com/us/article/kN0mYg?q=cardiac+arrest+and+cardiopulmonary+resuscitation
DEFINITION
Cardiac arrest is the cessation of normal circulation of the blood due to failure of the heart to contract effectively. Medical personnel can refer to an unexpected cardiac arrest as a sudden cardiac arrest or SCA.

CLASSIFICATION
Cardiac arrest is classified based upon the ECG rhythm into:
- Shockable (Ventricular fibrillation and Pulseless ventricular tachycardia)
- Non-shockable (Asystole and Pulseless electrical activity)

Ventricular Tachycardia

Ventricular Fibrillation

Ventricular Standstill (Asystole)

CARDIAC CAUSES
a) Coronary Heart Disease
- Approximately 60–70% of SCD is related to coronary heart disease.
- Among adults, ischemic heart disease is the predominant cause of arrest.
b) Non-Ischemic Heart Disease
- Cardiomyopathy
- Cardiac rhythm disturbances (VT/VF/Asystole/PEA)
- Hypertensive heart disease
- Congestive heart failure
Hs AND Ts (REVERSIBLE CAUSES)
“Hs and Ts” is the name for a mnemonic used to aid in remembering the possible treatable or reversible causes of cardiac arrest.
Hs
- Hypovolemia
- Hypoxia
- Hydrogen ions
- Hyperkalemia
- Hypokalemia
- Hypothermia
- Hypoglycemia
Ts
- Tablets or Toxins
- Cardiac Tamponade
- Tension
- Pneumothorax
- Thrombosis
- Thromboembolism
- Trauma
SIGNS & SYMPTOMS
The most reliable sign is absence of pulse.
- Unconsciousness
- No breathing
- No Blood Pressure
- Pupils begin dilating within 45 seconds
- Seizures may/may not occur
- Death – like appearance
- Lips & nail buds turn blue
DIAGNOSIS
- Cardiac arrest is synonymous with clinical death.
- Lack of carotid pulse is the gold standard for diagnosing cardiac arrest.
- Cardiac arrest is usually diagnosed clinically by the absence of a pulse, but lack of a pulse (particularly in the peripheral pulses) may be a result of other conditions (e.g., shock), or simply an error on the part of the rescuer.
MANAGEMENT OVERVIEW
Sudden cardiac arrest may be treated via attempts at resuscitation. This is usually carried out based upon:
- Basic Life Support (BLS)
- Advanced Cardiac Life Support (ACLS)
- Pediatric Advanced Life Support (PALS)
- Neonatal Resuscitation Program (NRP)
Management Interventions
- Cardiopulmonary resuscitation (CPR)
- Defibrillation
- Medications
- Therapeutic hypothermia
- Extracorporeal membrane oxygenation (ECMO) devices

CARDIO-PULMONARY RESUSCITATION (CPR)


Steps in Resuscitation (DRSCABD)
- D – Check for Danger
- R – Check for Response
- S – Send for help
- C – Chest compressions
- A – Open the Airway
- B – Check Breathing
- D – Defibrillation (AED)
Steps in CPR
- Recognition of the arrest
- Compressions
- Managing the airway
- Rescue breaths
RECOGNITION OF ARREST
- Check for response
- Tap the victim on the shoulder and shout, “Are you all right?”
- Take no more than 10 seconds to check for a pulse
- Adults – Check carotid artery
- Infants – Check brachial artery
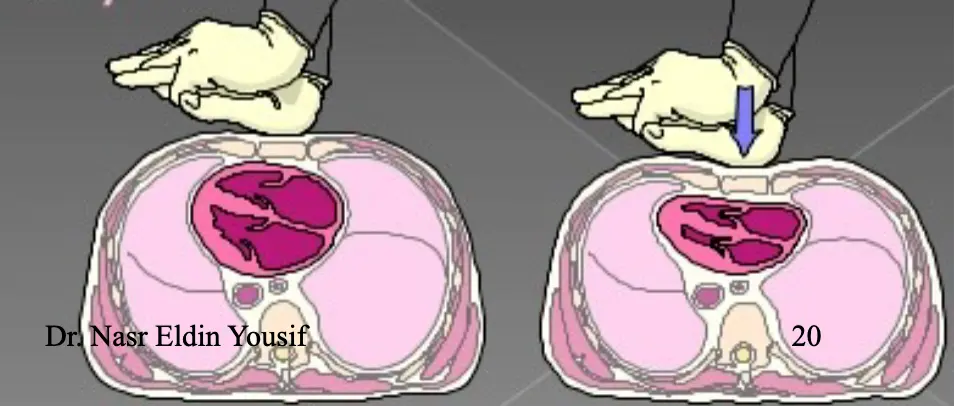
COMPRESSIONS
- Push hard & fast (at least 100/min)
- Compressions to relaxation ratio 50:50
- Ensure full chest recoil
- Minimal interruption of compressions

Circulation (C)
Restore the circulation, start external cardiac massage.


How CPR Works
- Effective CPR provides 1/4 to 1/3 normal blood flow
- Rescue breaths contain 16% oxygen (vs. 21% in room air)
USING AN AUTOMATED EXTERNAL DEFIBRILLATOR (AED)
Steps (1 of 8)
- Assess responsiveness
- Stop CPR if in progress
- Check breathing and pulse
- If patient is unresponsive and not breathing adequately, give two slow ventilations

AIRWAY MANAGEMENT
Head Tilt-Chin Lift
- Place one hand on the victim’s forehead & push with your palm to tilt the head back
- Place the fingers of the other hand under the bony part of the lower jaw near the chin
- Lift the jaw to bring the chin forward
Jaw Thrust
Indication
- Cervical spine injury
Procedure
- Place one hand on each side of the victim’s head, resting your elbows on the surface on which the victim is lying
- Place your fingers under the angles of the victim’s lower jaw & lift with both hands, displacing the jaw forward
- If the lips close, retract the lower lip with your thumb
Checking Vital Signs: A – Airway
- ☐ A – Airway
- Open the airway
- Head tilt-chin lift

A (Airway) – Ensure Open Airway






RESCUE BREATHS
- Deliver each rescue breath over 1 second
- Look for visible chest rise
- Compression to ventilation ratio: 30:2 (30 chest compressions to 2 ventilations)
Advanced Airway (in place)
- Give 1 breath every 6 to 8 seconds without attempting to synchronize breaths between compressions
- This equals 8 to 10 breaths/min
MOUTH-TO-MOUTH RESCUE BREATHING
- Hold the victim’s airway open with a head tilt-chin lift
- Pinch the nose closed with your thumb & index finger (using the hand on the forehead)
- Take a regular breath (not deep) & seal your lips around the victim’s mouth, creating an airtight seal
- Give 1 breath over 1 sec & watch for chest rise
- If the chest doesn’t rise, repeat the head tilt-chin lift
- Give a second breath & watch for chest rise
B (Breathing)

Place your mouth over the victim’s mouth and exhale.

TWO-RESCUER CPR
- One rescuer should kneel at the victim’s side and perform compressions (CPR)
- The other rescuer should kneel at the opposite side near the victim’s head and deliver artificial breaths
- Switch roles every 2 minutes to prevent fatigue

WHEN TO STOP CPR
- The person revives and starts breathing again on their own
- Medical help (e.g., ambulance paramedics) arrives to take over
- The rescuer is forced to stop from physical exhaustion
- Death of the victim
- If onset of CPR was < 6 minutes: Continue CPR for 30 minutes
- If onset of CPR was > 6 minutes: CPR can be terminated after 15 minutes
ADVANCED CARDIAC LIFE SUPPORT (ACLS)
DEFIBRILLATION
External depolarization of the heart to stop Ventricular Fibrillation (VF) or Ventricular Tachycardia (VT) that has not responded to other maneuvers.
Automated External Defibrillator (AED)

Defibrillation Procedure

- Position paddles correctly
- “Clear” the patient (ensure no one is touching)
- Deliver shock and then resume CPR for 5 cycles
- Re-analyze rhythm after each shock
- Prepare drug therapy
ADULT BASIC LIFE SUPPORT (BLS) ALGORITHM
- Call for help and an AED
- Open the victim’s airway, check for breathing, give two breaths
- Start CPR – 30 compressions to 2 ventilations (100 compressions/minute)
- On arrival of a defibrillator or AED, check for a shockable rhythm
- Give one shock if indicated, then resume CPR for another 5 cycles
- If no shock is indicated, continue another 5 cycles of CPR


MEDICATIONS IN CARDIAC ARREST
Amiodarone (Cordarone)
Indications
- Like Lidocaine – for Ventricular Tachycardia (VTach) and Ventricular Fibrillation (VFib)
IV Dose
- 300 mg in 20-30 ml of N/S or D5W (initial bolus)
- Supplemental dose of 150 mg in 20-30 ml of N/S or D5W
- Followed with continuous infusion of 1 mg/min for 6 hours, then 0.5 mg/min to a maximum daily dose of 2 grams
Contraindications
- Profound Sinus Bradycardia
- 2nd and 3rd degree heart block
Atropine
Indications
- Symptomatic sinus bradycardia
- Second Degree Heart Block Mobitz I
- May be tried in asystole
- Organophosphate poisoning
IV Dose
- 0.5 – 1 mg every 3-5 minutes
- Max dose is 0.04 mg/kg
- Can be given down ET tube (endotracheal)
Side Effects
- May worsen ischemia
Epinephrine (Adrenaline)
- Because of alpha, beta-1, and beta-2 stimulation, it increases:
- Heart rate
- Stroke volume
- Blood pressure (BP)
- Helps convert fine VFib to coarse VFib
- May help in asystole
- Also used in EMD/PEA and symptomatic bradycardia
IV Dose
- 1 mg every 3-5 minutes
- Can be given down the ET tube
- Can also be given intracardiac
Considerations
- May increase ischemia because of increased O2 demand by the heart
Norepinephrine (Levophed)
- Similar in effect to epinephrine
- Used for severe hypotension that is NOT due to hypovolemia
- Used in cardiogenic shock
- Administered as a continuous infusion
Adult Dose
- Usually 2-12 micrograms/min
- Range is 0.5-1 microgram up to 30 micrograms
Side Effects
- Like epinephrine, it may worsen ischemia
- Extravasation causes tissue necrosis
Dopamine
- Used for hypotension (not due to hypovolemia)
- Usually tried before norepinephrine
- Has alpha, beta, and dopaminergic properties
- Dopaminergic effect dilates renal and mesenteric arteries
- Second choice for bradycardia (after Atropine)
IV Dose
- 1-20 micrograms/kg/min
Side Effects
- Ectopic beats
- N & V
Dobutamine
- Actions similar to Dopamine
- Used for CHF with hypotension
IV Dose
- 2-20 micrograms/minute
Side Effects
- Tachycardia
- Nausea & Vomiting (N & V)
- Headache
- Tremors
ACLS MEDICATION SUMMARY TABLE
 |
|---|
ACLS ALGORITHMS


