Guillain-Barré Syndrome (GBS)
DR FAROOQ SATTAR DHEDHI https://next.amboss.com/us/article/7R04of?q=guillain-barr%C3%A9+syndrome
Introduction
- GBS is an acute immune-mediated polyneuropathy.
- Most common cause of acute flaccid paralysis worldwide.
- Often follows infection, vaccination, or surgery.
- Medical emergency due to risk of respiratory failure.
Epidemiology
- Incidence: 1–2 per 100,000 per year.
- Can occur at any age.
- Slight male predominance.
- Often triggered by infections.
Pathophysiology
- Immune-mediated demyelination and/or axonal degeneration of peripheral nerves.
- Molecular mimicry between microbial antigens and nerve components.
- Results in impaired nerve conduction and muscle weakness.
Demyelination and Axonal Damage in GBS
Etiology and Triggering Pathogens
Common triggering pathogens include:
- Campylobacter jejuni (most common) - 30% of cases
- Cytomegalovirus - 10% of cases
- Epstein-Barr virus - 10% of cases
- Mycoplasma
- Other triggers: Zika virus, influenza, COVID-19
GBS typically occurs days to weeks after the trigger.
Clinical Presentation
Cardinal Features
- Rapidly progressive, symmetrical weakness (ascending paralysis).
- Weakness starts in legs → arms → cranial nerves.
- Lower limbs → Upper limbs → Rest of the body progression (Original: L. LOWER LIMBS — UPPER LIMBS — REST OF THE BODY).
- Weakness is rapidly progressive.
- Areflexia (absent deep tendon reflexes).
- Reaches maximum severity within 4 weeks.
Sensory and Autonomic Features
- Sensory symptoms: tingling, numbness, mild pain.
- Paresthesias (tingling, pins and needles).
- Pain (moderate to severe in 50% of patients).
Cranial Nerve and Bulbar Involvement
- Cranial nerve involvement (facial weakness, dysphagia).
Autonomic Dysfunction
- Tachycardia.
- Blood pressure fluctuations (BP fluctuations).
- Cardiac arrhythmias.
- Sweating abnormalities.
Respiratory Involvement
- Respiratory muscle involvement → ventilatory failure.
- Respiratory compromise in severe cases (20-30% of patients).
- Severe cases clients can develop:
- Flaccid paralysis.
- Difficulty moving/walking.
Clinical Presentation Summary Table
| Flaccid Paralysis (FLACCIO BARRYSS) | Difficulty Moving/Walking (OFFICULTY) | Absent Deep Tendon Reflexes (ABSENT DEEP TENDEN REFLEXES) |
|---|---|---|
 |
LEARN MORE … (OCHOSIS.org)
Diagnostic Criteria
Brighton Criteria Diagnostic Levels
Diagnosis relies on clinical features, CSF findings, and nerve conduction studies. The Brighton criteria provide diagnostic certainty levels from Level 1 (highest certainty) to Level 4 (lowest certainty) based on clinical presentation and supporting evidence.
GBS Variants
- Acute Inflammatory Demyelinating Polyneuropathy (AIDP) – most common in Europe/USA.
- Acute Motor Axonal Neuropathy (AMAN) – common in Asia, children.
- Miller Fisher Syndrome – ophthalmoplegia, ataxia, areflexia.
- Others: Acute Motor-Sensory Axonal Neuropathy (AMSAN).
Investigations and Diagnostic Workup
Cerebrospinal Fluid (CSF) Analysis
- Albuminocytologic dissociation (↑ protein, normal cells).
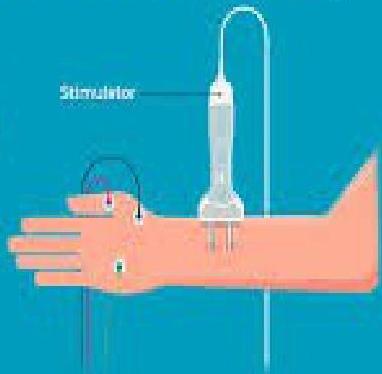
Nerve Conduction Studies
- Demyelination/axonal loss patterns.

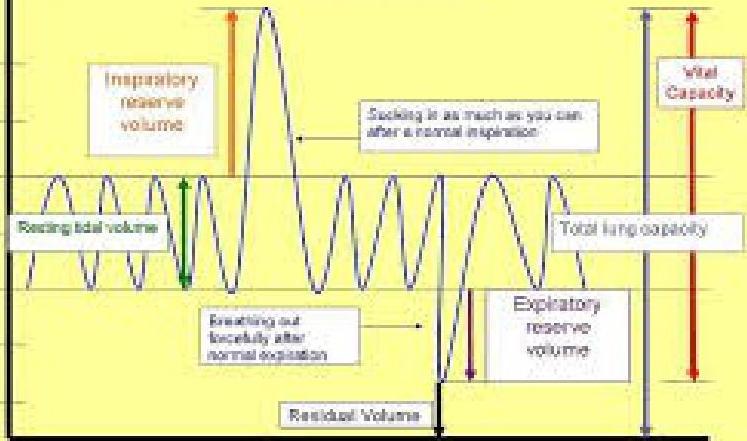
Pulmonary Function Tests
- Vital capacity monitoring.

Blood Tests
- Blood tests to exclude other causes.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Poliomyelitis | Asymmetric weakness |
| Myasthenia gravis | Fluctuating weakness |
| Botulism | Descending paralysis |
| Spinal cord disease | Upper motor neuron signs |
| Hypokalemic periodic paralysis | Electrolyte abnormality |
Management
Supportive Care
- Monitoring of respiration and autonomic function.
- Physiotherapy and rehabilitation.
Immunomodulatory Therapy
- Plasma exchange (plasmapheresis).
- IV Immunoglobulin (IVIG).
- Steroids are NOT effective.
Complications
Acute Complications
- Respiratory failure (most serious acute complication).
- Aspiration pneumonia.
- Deep vein thrombosis and pulmonary embolism.
- Pressure sores and contractures.
- Residual neurological deficits.
Mechanical Ventilation Requirements
- Respiratory failure is the most serious acute complication.
- Requires ICU admission and mechanical ventilation in approximately one-fifth of patients.
Prognosis
Recovery Rates
- Most patients recover fully over weeks to months.
- Full Recovery Rate: Majority of patients recover completely or with minor residual deficits within 12 months.
- Recovery begins within weeks to months after symptom plateau.

Mortality
- Mortality: 5% (due to respiratory/autonomic failure).
- Death occurs in approximately 5% of cases, usually from complications like respiratory failure, autonomic dysfunction, or thromboembolic events.
Long-term Outcomes
- 20% of patients left with persistent disability.
- Persistent Symptoms: About 20% of patients experience residual weakness, fatigue, or sensory symptoms that may persist for years.
- Recurrence is rare (2-5%) but possible.
- Ongoing rehabilitation is crucial for optimizing functional outcomes.
Clinical Images Gallery

Summary
- GBS is an acute immune-mediated neuropathy causing ascending paralysis.
- Commonly follows infection (e.g., Campylobacter jejuni).
- Diagnosis: clinical + CSF + nerve studies.
- Treatment: IVIG or plasmapheresis + supportive care.
- Prognosis: Good recovery in majority, but can be fatal if untreated.