Gastrointestinal bleeding
Clinical Approach
Dr. Eatimad Mahgoub Osheik
Learning Objectives
- Define and classify GIT bleeding
- Recognize clinical presentations
- Perform initial assessment and resuscitation
- Choose appropriate diagnostic investigations
- Identify common causes of upper and lower GIT bleeding
- Outline management of peptic ulcer disease and esophageal varices
Introduction
- GIT bleeding is a common medical emergency
- Severity ranges from occult bleeding to life-threatening hemorrhage
- Early recognition and prompt management are essential
Classification of GIT Bleeding
Based on Anatomical Location
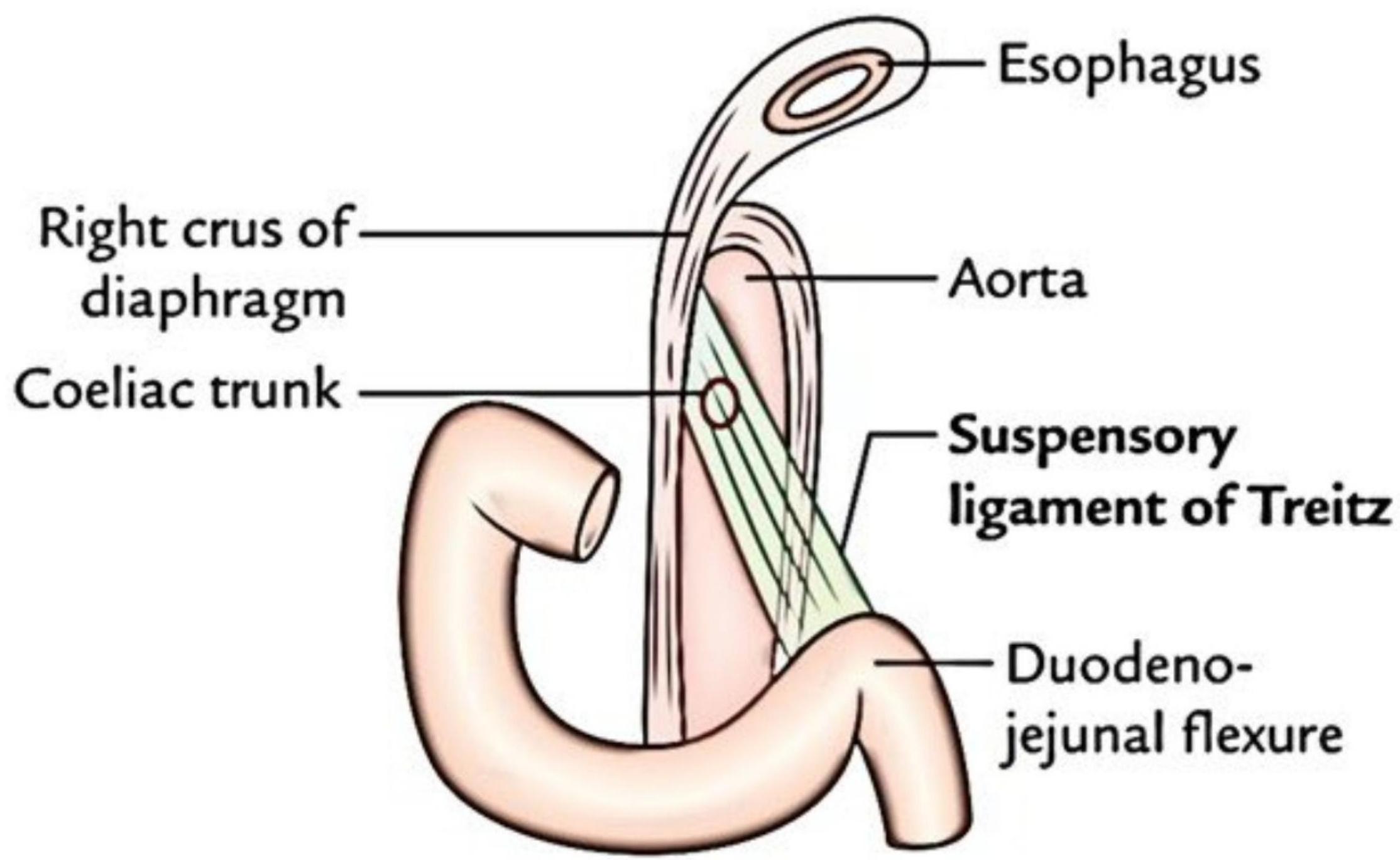
- Upper GIT bleeding: From esophagus to the duodenum (proximal to ligament of Treitz)
- Lower GIT bleeding: From jejunum to anus (distal to ligament of Treitz)
Based on Clinical Severity
- Occult bleeding: Not visible, detected by fecal occult blood test
- Overt bleeding: Visible bleeding (hematemesis, melena, hematochezia)
- Massive bleeding: Hemodynamic instability, shock, need for transfusion
Clinical Definitions
- Hematemesis: Vomiting of fresh blood (UGIB)
- Coffee-ground emesis: emesis of blood exposed to gastric acid (UGIB)
- Melena: Black, tarry, foul-smelling stool from digested blood (Usually UGIB but can be from small bowel or right colon)
- Hematochezia: Passage of fresh blood per rectum (LGIB)
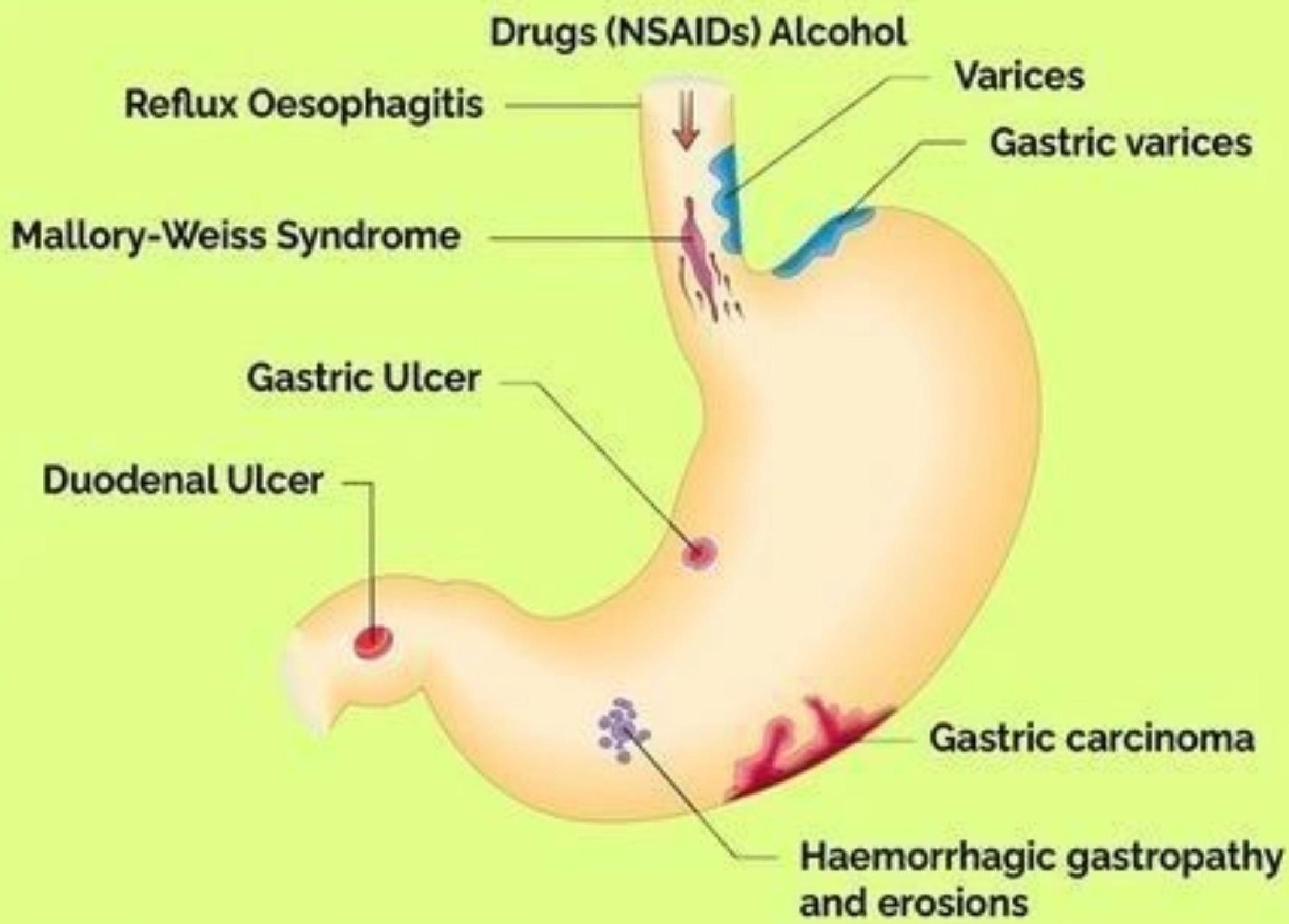
Common Causes of Upper GI Bleeding
1. Peptic Ulcer Disease (most common)
- Gastric ulcers
- Duodenal ulcers
- Causes: H. pylori, NSAIDs, stress, smoking
2. Esophageal Causes
- Esophageal varices (portal hypertension, liver cirrhosis)
- Esophagitis (reflux, drugs, infections)
- Mallory-Weiss tear (forceful vomiting/retching)
3. Gastric Causes
- Erosive gastritis
- Gastric cancer
- Stress-related mucosal disease (ICU, burns, sepsis)
4. Vascular Lesions
- Angiodysplasia
- Aortoenteric fistula
5. Post procedure
Causes of Upper GIT Bleeding
Initial Management of GIT Bleeding
1. Severity Assessment
- Airway: Risk of aspiration in massive hematemesis
- Breathing: Oxygen saturation, respiratory distress
- Circulation:
- Blood pressure, pulse rate
- Signs of shock (tachycardia, hypotension, cold extremities, altered mental state)
2. Focused History
- Nature of bleeding (hematemesis, melena, hematochezia)
- Duration and amount of bleeding
- History of:
- Peptic ulcer disease
- Liver disease / alcohol use
- NSAIDs, aspirin, anticoagulants
- Previous GI bleeding
- Associated symptoms: epigastric pain, weight loss, dysphagia
3. Physical Examination
- Vital signs and postural hypotension
- Signs of anemia (pallor)
- Abdominal examination (tenderness, masses)
- Stigmata of chronic liver disease (spider nevi, ascites)
- Digital rectal examination
4. Initial Fluid Resuscitation
Insert two wide bore intravenous lines
Crystalloids first: Ringer’s lactate or normal saline
Rapid bolus: 1 liter IV in adults, reassess
Monitor with BP, heart rate, mental status, urine output
5. Bloods (send immediately)
- CBC
- Type & crossmatch
- Coagulation profile (INR, PT, aPTT)
- Urea/creatinine
- LFTs (look for cirrhosis)
- Lactate
6. Early blood transfusion
- Target Hb:
- ≥7 g/dL (most patients)
- ≥8–9 g/dL if CAD, ongoing shock
7. Correct Coagulopathy
- Platelets if <50,000
- Fresh frozen plasma if INR >1.5
- Vitamin K if warfarin-related
- PCC for rapid warfarin reversal
8. Alert Endoscopy team for EGD
- Consider Intensive care unit admission if unstable vital signs
- Consider Intubation if shock, poor respiratory status, or GCS < 8.

9. Pharmacologic Therapy
Proton Pump Inhibitors (PPIs)
- IV PPI is first-line in suspected peptic ulcer bleed
- Loading: 80 mg IV bolus
- Then continuous infusion: 8 mg/hour IV for 72 hours
If Suspect Variceal bleeding
Clues for variceal bleed:
- Cirrhosis
- Alcohol use
- Stigmata of liver disease
Start immediately (don’t wait for endoscopy):
- Octreotide (or terlipressin)
- IV antibiotics (e.g., ceftriaxone)
Antibiotics save lives in variceal bleeds
Diagnostic Studies
Esophagogastroduodenoscopy (EGD) is the diagnostic modality of choice for UGI bleeding.
- Timing: Ideally within 24 hours, sooner (within 12 hours) if high-risk features (shock, massive hematemesis

Imaging Studies
- CT Angiography: Detects active bleeding ≥0.3–0.5 mL/min; useful if endoscopy inconclusive
- Conventional Angiography: For ongoing bleeding; allows embolization
- Radionuclide Scan (Tagged RBC)
- Capsule endoscopy

Risk Stratification for UGIB
1. Glasgow-Blatchford Score (GBS) – Best for initial triage
Before endoscopy
Predicts: Need for intervention (transfusion, endoscopy, surgery)
Interpretation
- GBS = 0–1 → Low risk → Often safe for outpatient management
- GBS ≥2 → Admit, urgent evaluation
Most sensitive for ruling out serious bleeding
Glasgow Blatchford score
| Admission risk marker | Score value |
|---|---|
| Blood urea (mmol/L) | |
| 6.5–8 | 2 |
| 8–10 | 3 |
| 10–25 | 4 |
| >25 | 6 |
| Hb (g/L) for men | |
| 120–130 | 1 |
| 100–120 | 3 |
| <100 | 6 |
| Hb (g/L) for women | |
| 100–120 | 1 |
| <100 | 6 |
| Systolic blood pressure (mmHg) | |
| 100–109 | 1 |
| 90–99 | 2 |
| <90 | 3 |
| Pulse ≥100/minute | 1 |
| History/co-morbidities | |
| Presentation with melaena | 1 |
| Presentation with syncope | 2 |
| Hepatic disease* | 2 |
| Cardiac failure† | 2 |
Rockall Score
Used pre- and post-endoscopy
Interpretation
- ⇐2 → Low mortality/rebleeding risk
- >=3 → High risk → Close monitoring
Better at predicting mortality than need for intervention
| 0 | 1 | 2 | 3 | |
|---|---|---|---|---|
| Age | <60 | 60-79 | >80 | |
| Shock | No shock | HR >100 | HR >100, SBP <100 | |
| Comorbidity | Cardiac failure, ischaemic heart disease | Renal failure, liver failure, disseminated malignancy | ||
| Diagnosis | Mallory Weiss, no lesion, no stigmata of recent haemorrhage | All other diagnoses | Malignancy of upper gastrointestinal tract | |
| SRH (Endoscopy) | None, or dark spot | Fresh blood, adherent clot, visible or spurting vessel |
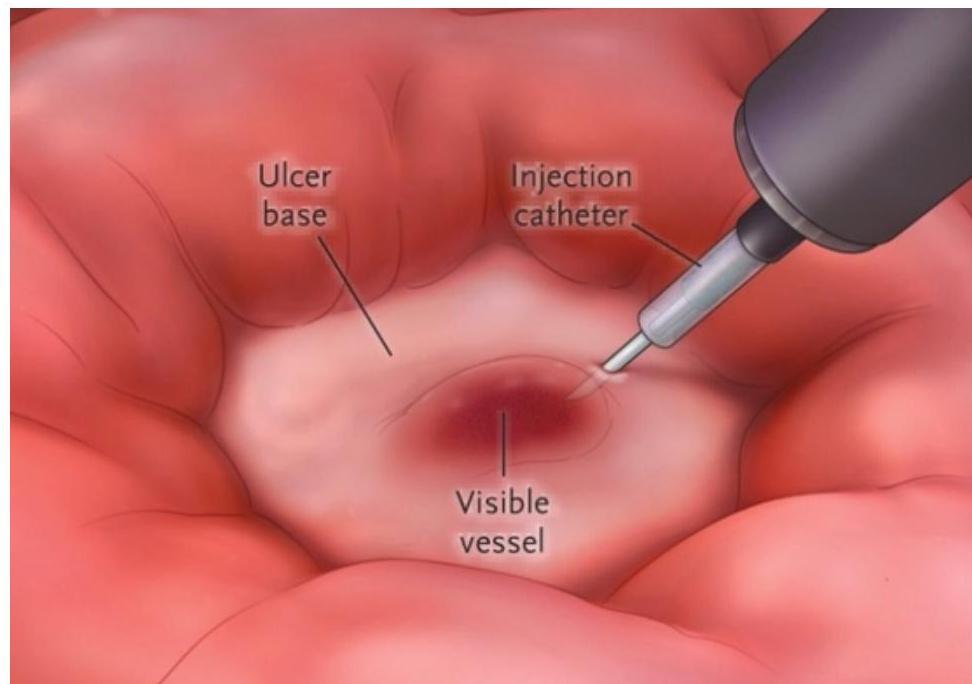
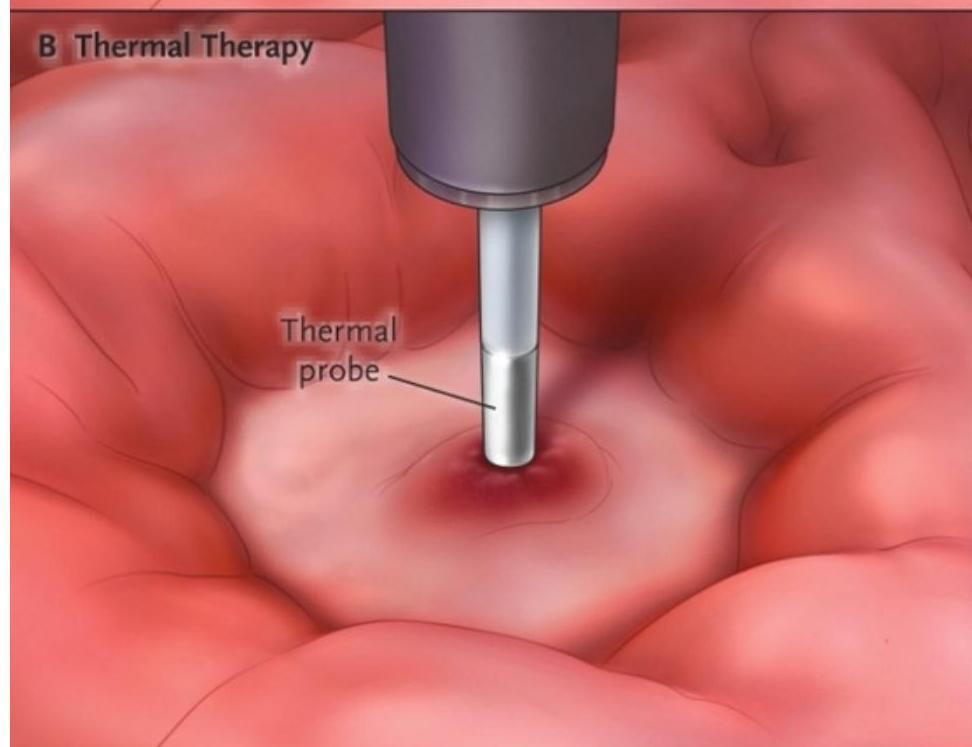
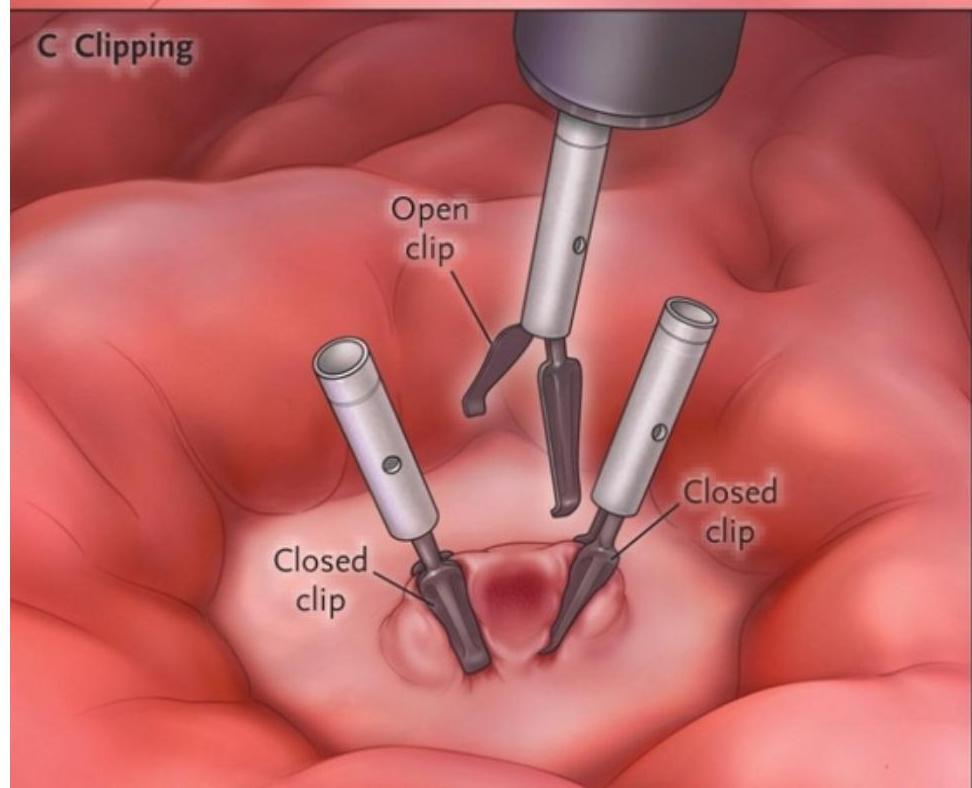
Endoscopic Therapy
Peptic Ulcer Bleeding
- Adrenaline injection (with another method)
- Thermal coagulation
- Hemoclips
- Best: Combination therapy
- Post-procedure: IV PPI
- Test and Treat H.pylori if present
- Biopsy
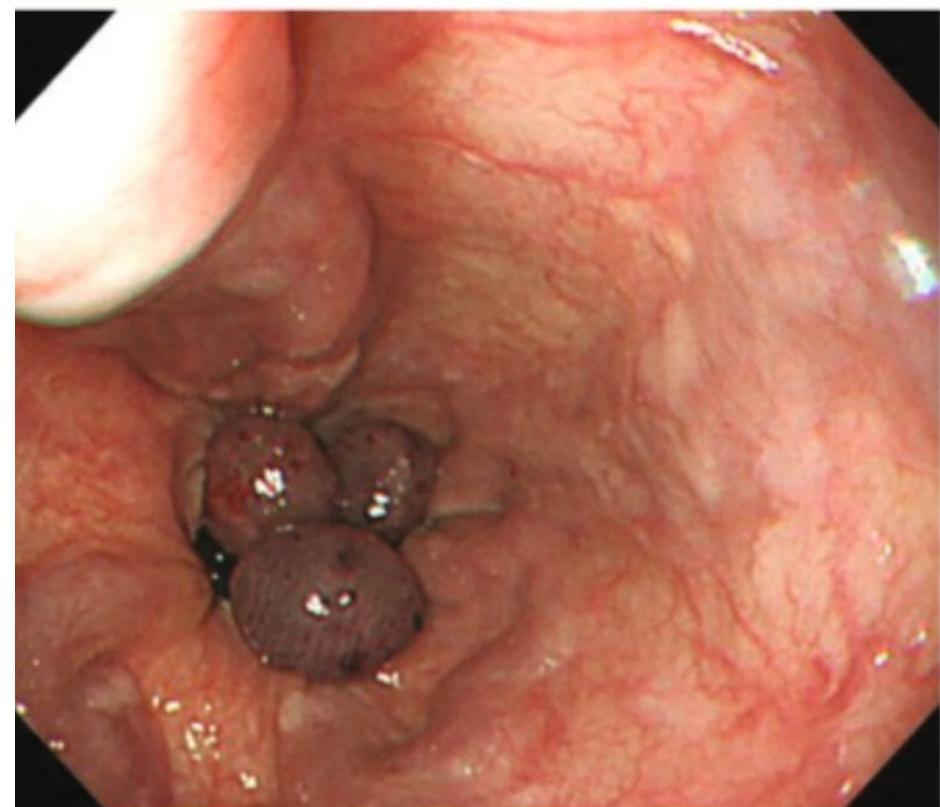
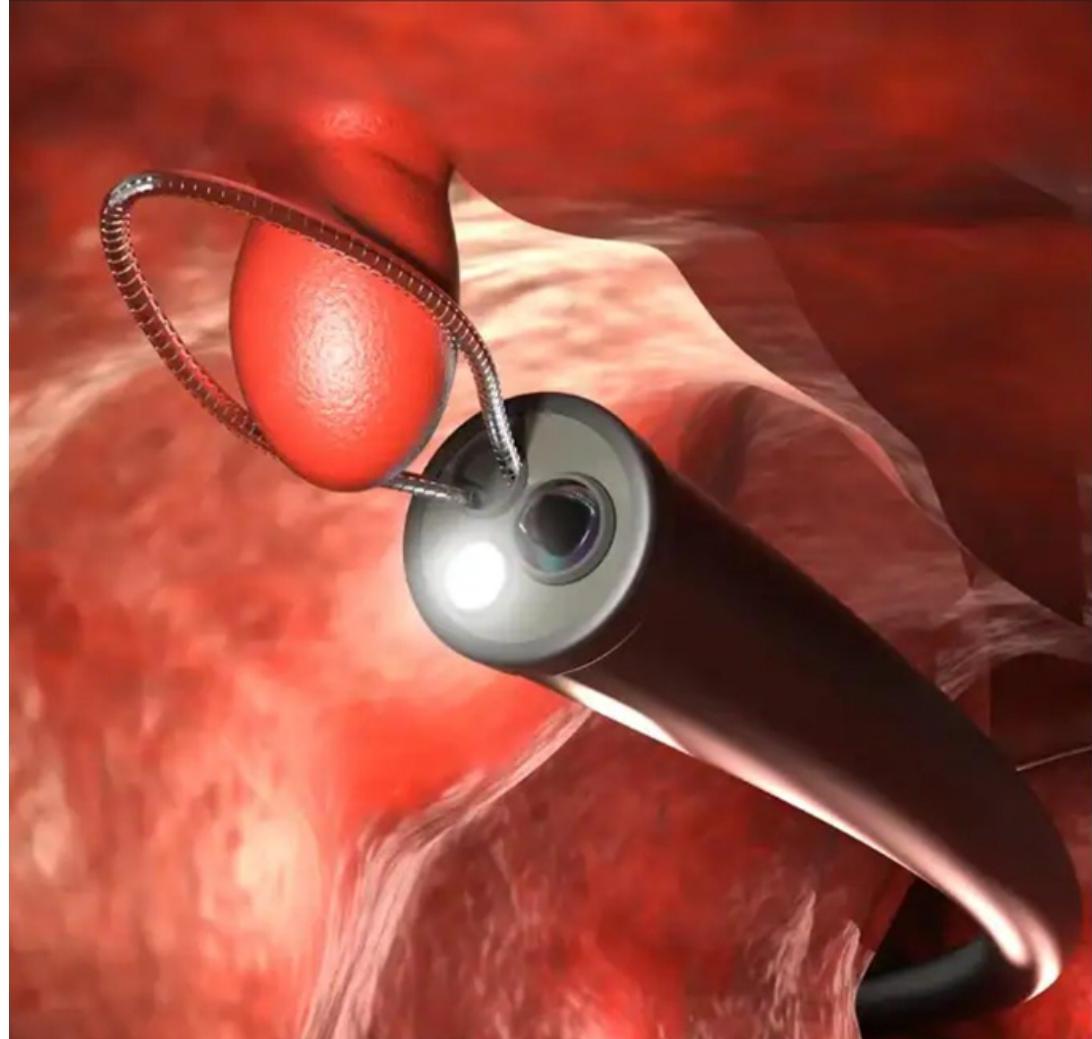
Esophageal Varices
- Treatment of choice: Endoscopic variceal ligation (EVL)
- Alternative: Sclerotherapy
- Gastric varices: Cyanoacrylate injection
- Add vasoactive drugs + antibiotics
- Transjugular Intrahepatic Portosystemic Shunt TIPS if refractory

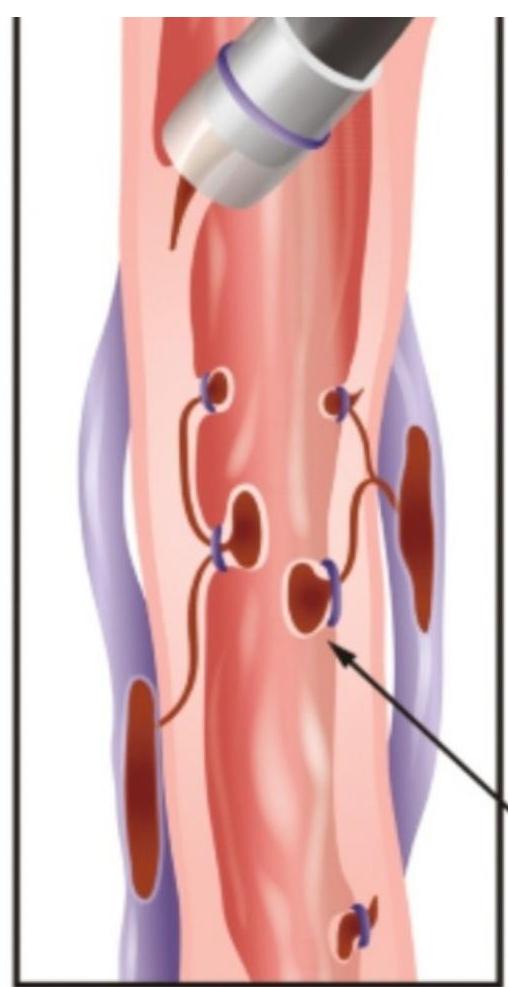
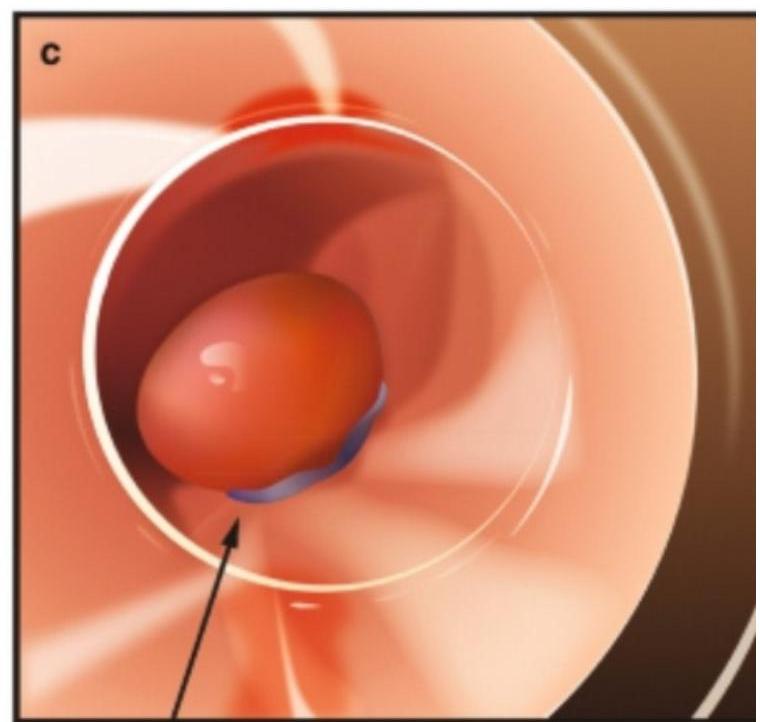
Banded varices
Lower GI Bleeding – Etiology
- Anorectal conditions
- hemorrhoids, anal fissure
- Inflammatory bowel disease
- Ulcerative Colitis
- Meckel’s diverticulum
- Diverticulosis (most common)
- Angiodysplasia
- Colorectal cancer
- Ischemic colitis
Management of lower GITBleeding
- Initial assessment (ABCDE)
- Resuscitation
- Investigations
- Colonoscopy (investigation of choice)
- CT angiography if ongoing brisk bleed
- Radionuclide scan if intermittent bleeding
- Definitive management (cause-specific):
- Endoscopic therapy (clipping, cautery, injection)
- Surgery for massive or refractory bleeding
Complications
- Hypovolemic shock
- Acute kidney injury
- Rebleeding
- Aspiration pneumonia
- Death (especially in elderly/comorbid patients)
Case scenario 1
A 48-year-old male presents to the emergency department with two episodes of hematemesis, approximately 200–300 mL each, followed by black tarry stools. He reports a burning epigastric pain for the past month, worse on an empty stomach and partially relieved by food. There is associated dizziness and generalized weakness.
Case scenario 2
A 52-year-old male presents with sudden onset of large-volume hematemesis, about 500 mL, associated with black stools and dizziness. There is no history of abdominal pain. The patient gives a history of progressive abdominal distension and swelling of feet over the past 6 months.