ACS: A Simple Way to an Updated Diagnosis & Management
By
Dr Nada Abdelrahman
Associate Professor of Medicine
AlMaarefa University

Lina Serhan
Learning Outcomes
By the end of this session, it is expected that the students will be able to:

- ☐ Diagnose different types of ACS
- ☐ Outline the steps in the management of different types of ACS
- ☐ Interpret and manage different ACS clinical scenarios
ESSENCE

CAD is the third leading cause of mortality worldwide and is associated with 17.8 million deaths annually.

Delay in seeking medical attention is common, and more often reported in:
- Women
- Older adults
- Patients with high chronic disease burden

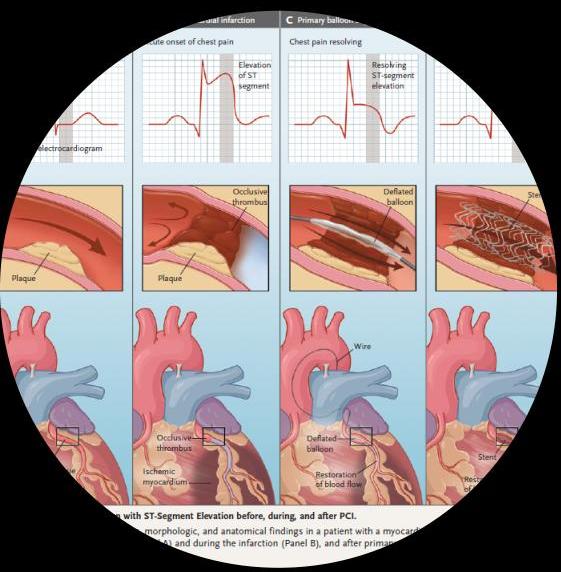
The management of ACS has evolved over recent years, with the development of new drugs and procedures such as percutaneous coronary intervention (PCI).
we All slent Cue the problem in stenosis
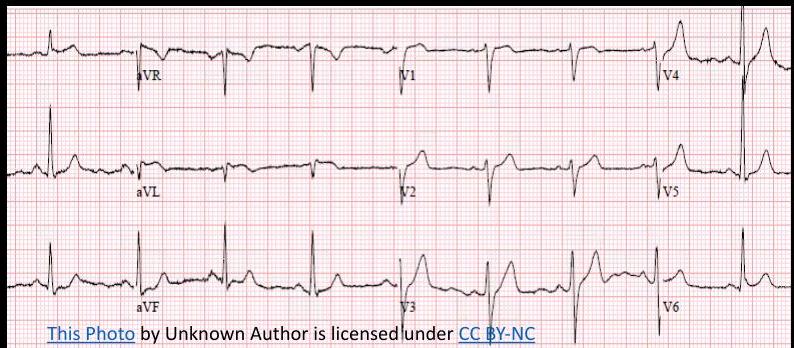
ECG Revision 1
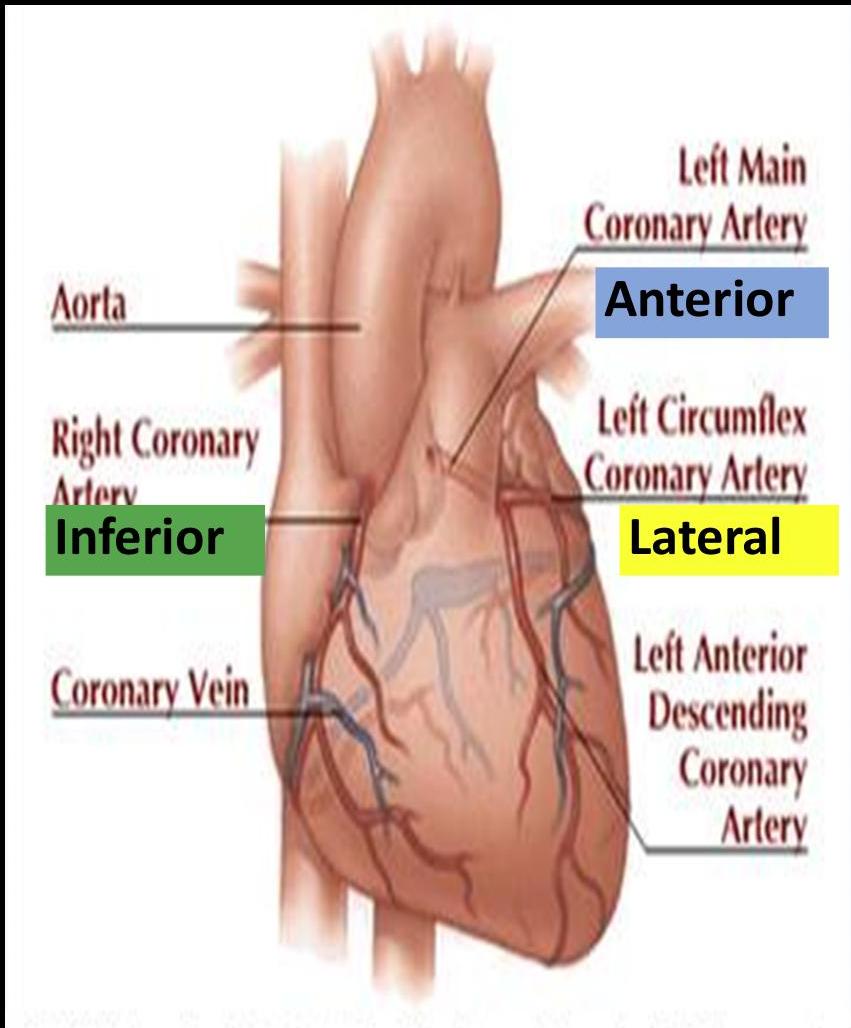
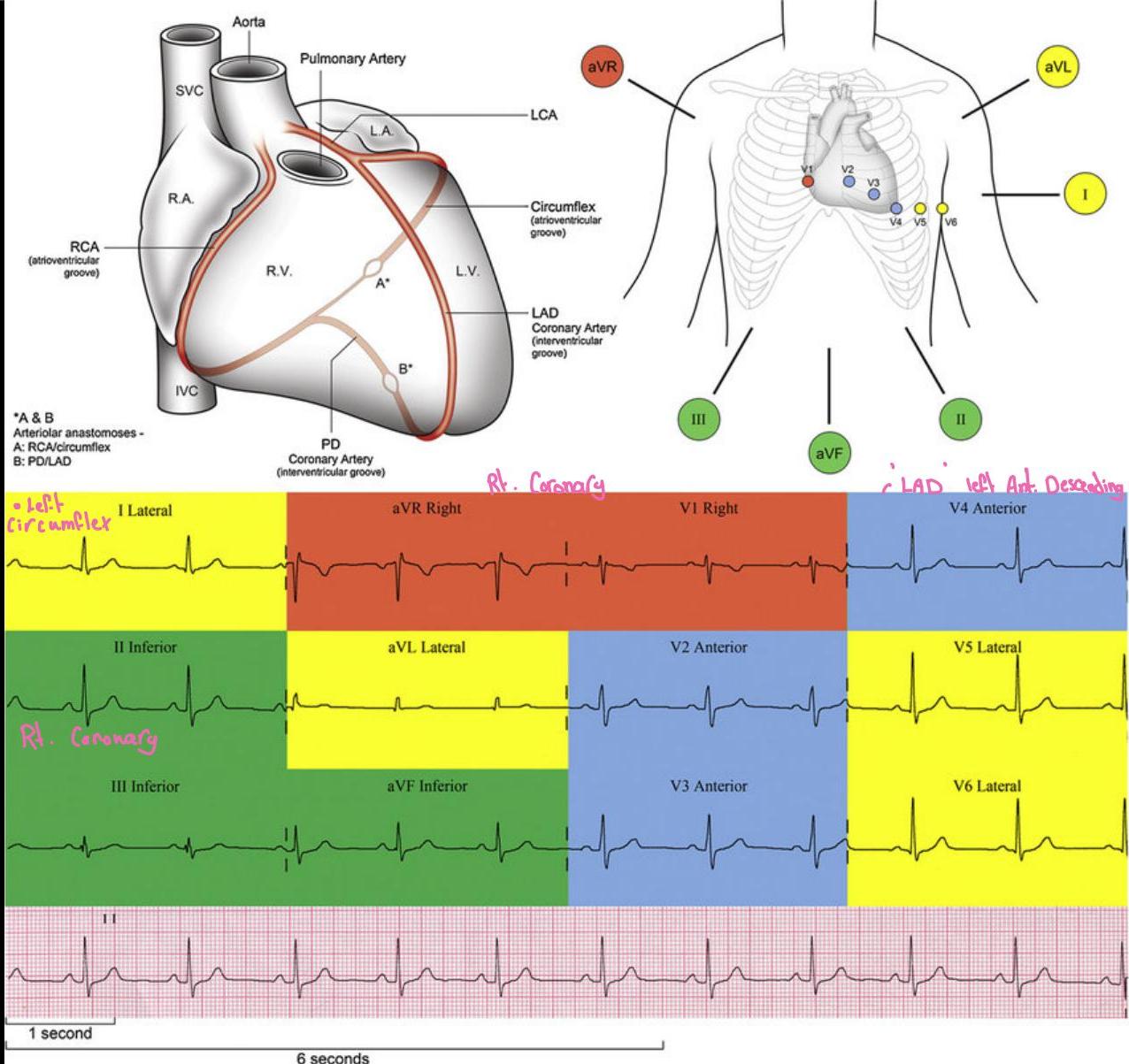
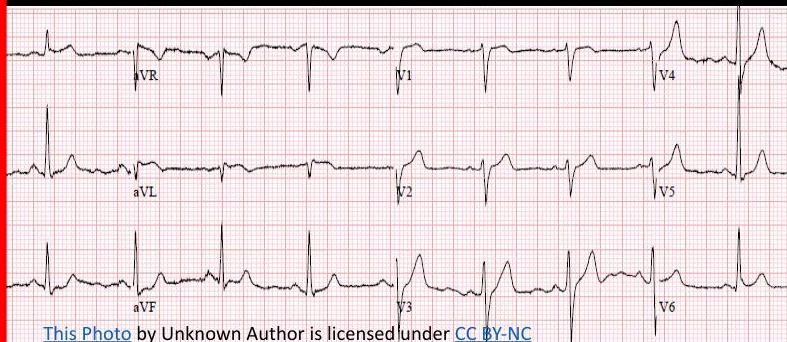
Case: A 57-year-old man presents to the Emergency Department with a 15-minute history of severe central chest pain radiating to his left arm.
ECG Findings: T-wave inversion in leads I, V5 and V6.
Question: Which coronary artery is most likely to be affected?
Answer: Lateral left — Lt. Circumflex
Quick Recap
Paper running at 25mm/second
Calibration: height 1cm = 1mV
ECG Case 2
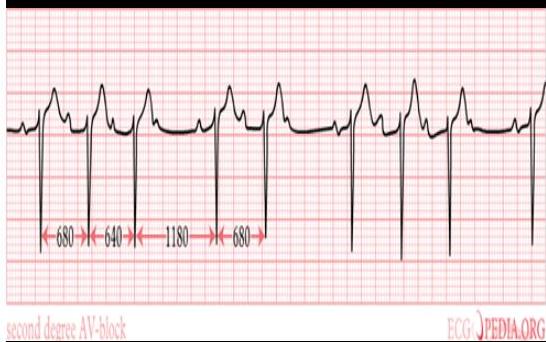
Case: A 72-year-old man is admitted to the Emergency Department with chest pain. On initial assessment he is noted to be:
- Pale
- Heart rate: 40/min (Bradycardia)
- Blood pressure: 90/60 mmHg
Question: Which one of the coronary arteries is most likely to be affected?
Answer: Inferior
Always gives you Bradycardia
( ) supply of ventricular
Treatment: Ht: Fluid
Initial Approach: What to Do!!!
ABC
add million
MONA
(don’t give it oxygen 94% or above)
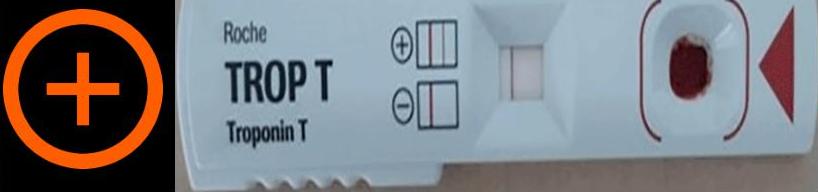
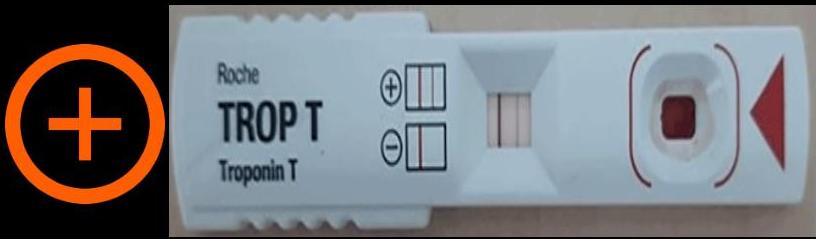
ECG, troponin

This Photo by Unknown Author is licensed under CC BY-SA NC
Initial Approach

This Photo by Unknown Author is licensed under CC BY-SA NC

CC BY-NC

This Photo by Unknown Author is licensed under CC BY SA
Case 3: Anginal Pain
Case: A 79-year-old lady presents to the low-risk chest pain clinic with intermittent substernal chest pains.
Characteristics:
- Pain typically comes on with exertion
- Improves with rest
- Trial of GTN given by her FP which helps with her pain
Risk Factors:
- Known ex-smoker: 30 pack-years
- No diabetes
- No hyperlipidaemia
- No hypertension
- No family history of coronary artery disease
Examination:
- Observations: Stable
- Auscultation: First and second heart sounds audible with no added sounds
- Lungs: Clear
Diagnosis: Anginal Pain
Question: What is the most important investigation to pursue given her risk for coronary artery disease?
Answer:
- Non-invasive approach
- 1st: CT angiography
- 2nd: Stress test
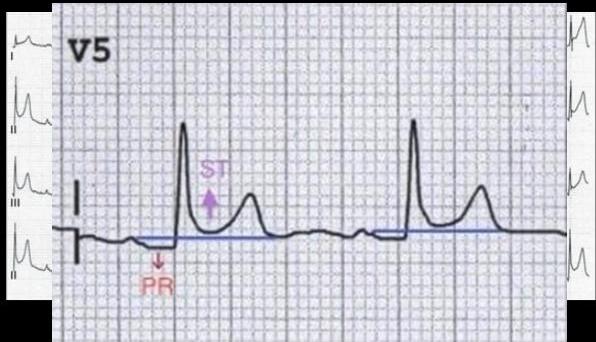
ECG Criteria for STEMI
New persistent ST elevation (>20 minutes) in ≥ 2 contiguous leads
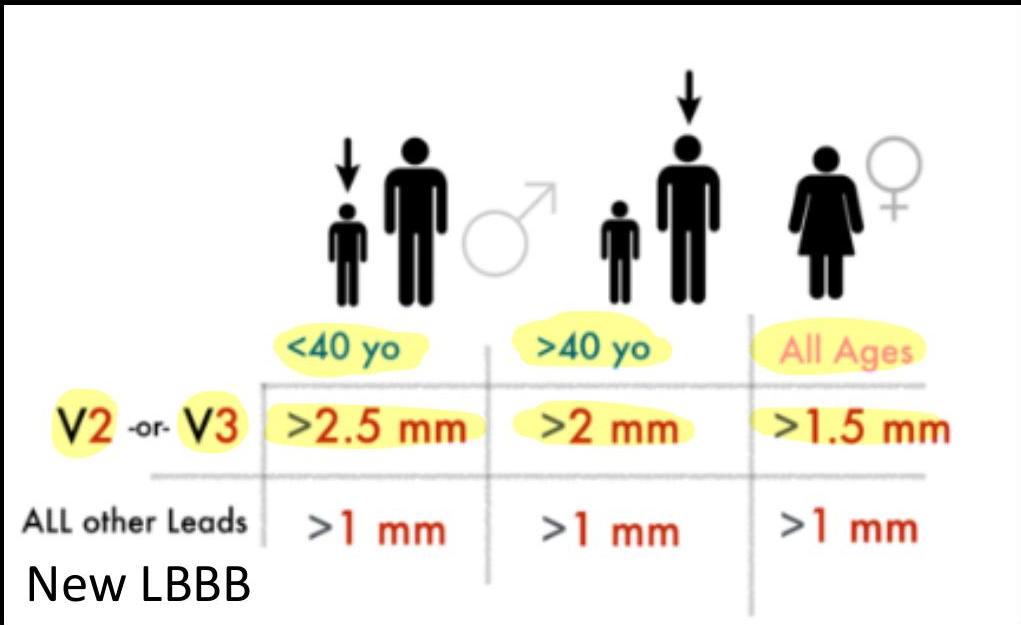


Measuring ST Deviation

- 4 small boxes = 4 mm ST elevation
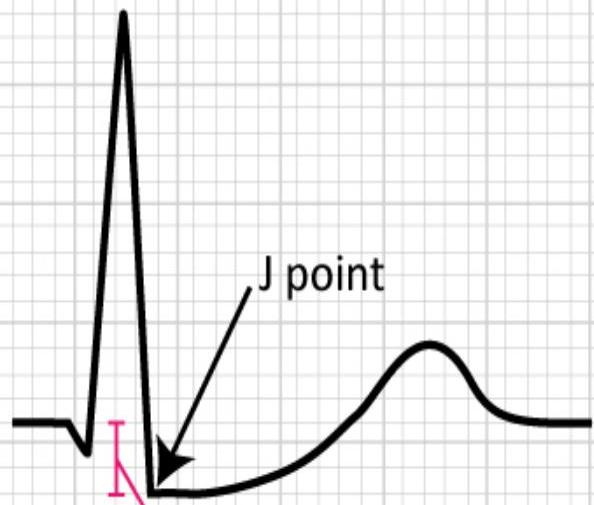
- 3 small boxes = 3 mm ST depression
50 mm/s

Figure 14. Example of measuring ST deviation (elevation and depression).
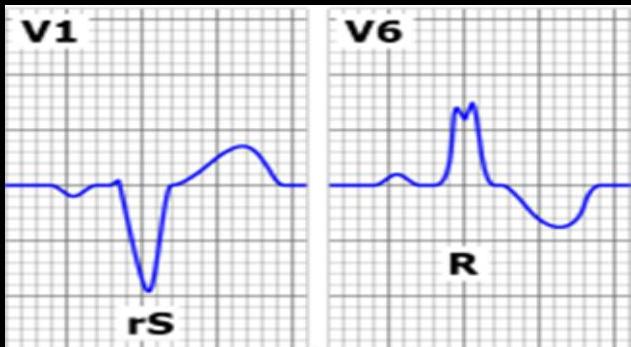
LBBB and RBBB: WiLLiaM MaRRoW Pattern
LBBB (Left Bundle Branch Block)
Required: PCI or thrombolytic therapy
WiLLiaM MaRRoW Mnemonic
In LBBB:
- V1: There is a ‘W’ shape
- V6: There is a ‘M’ shape
In RBBB:
- V6: There is a ‘W’ shape
- V1: There is a ‘M’ shape
Brand QR Shred
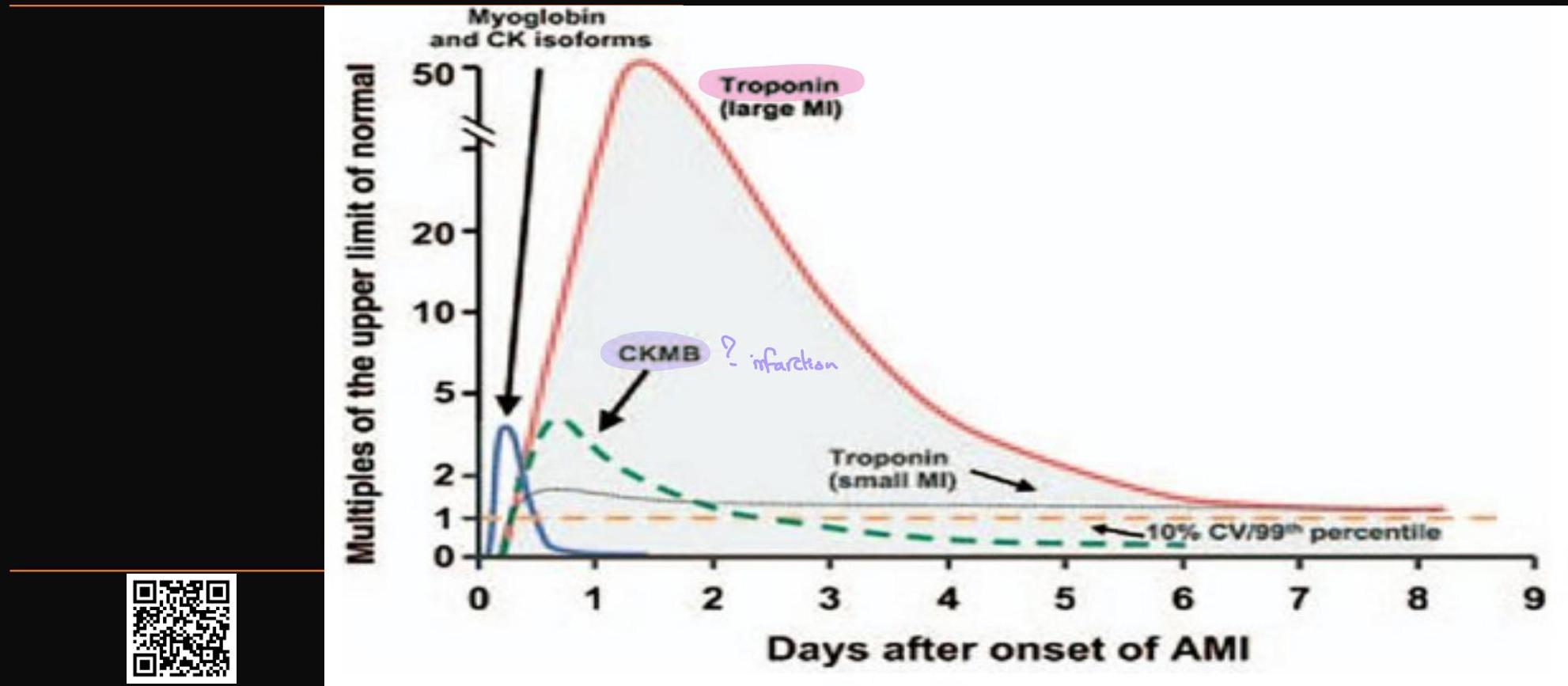
Cardiac Markers
Acute Coronary Syndrome
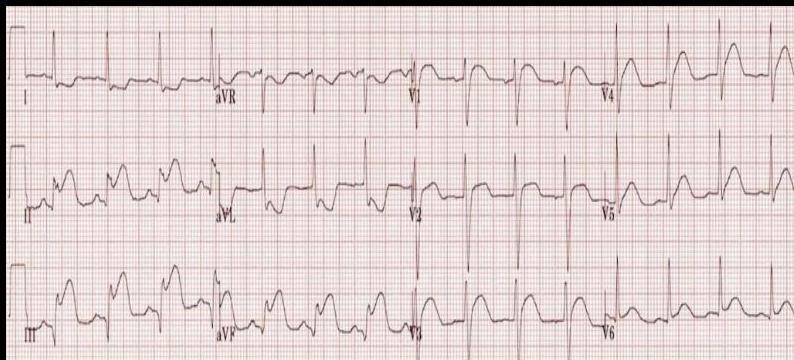


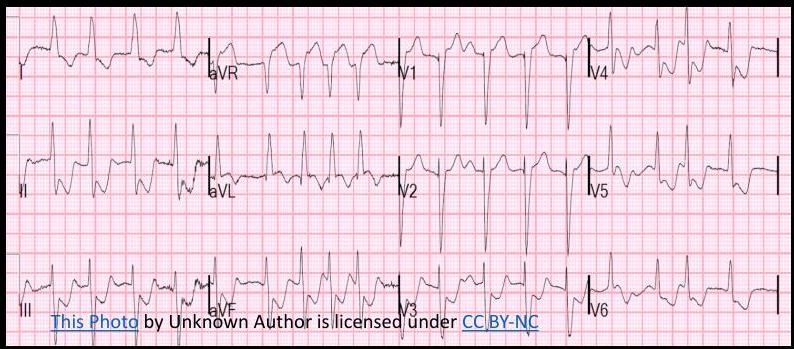



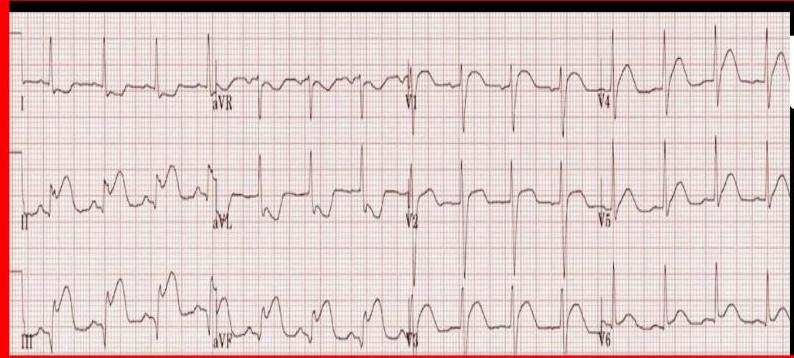


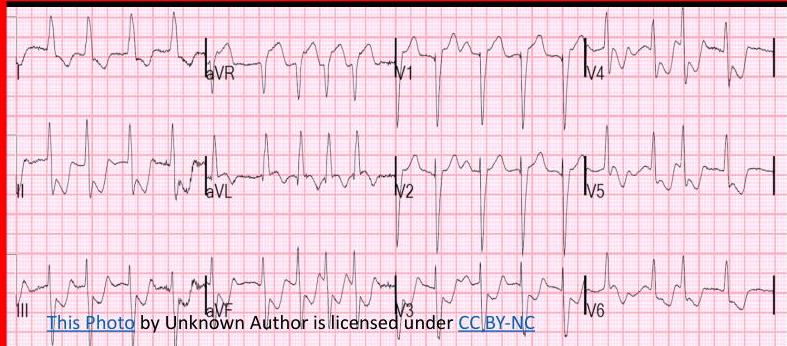


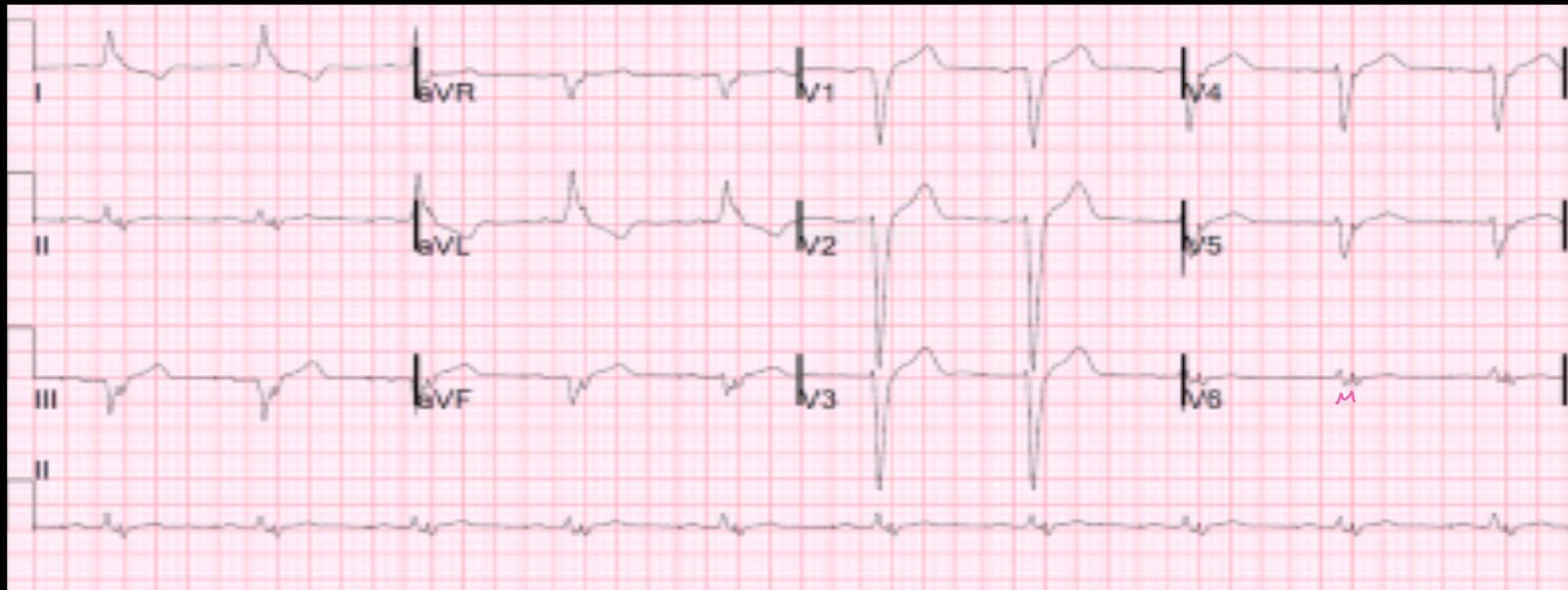
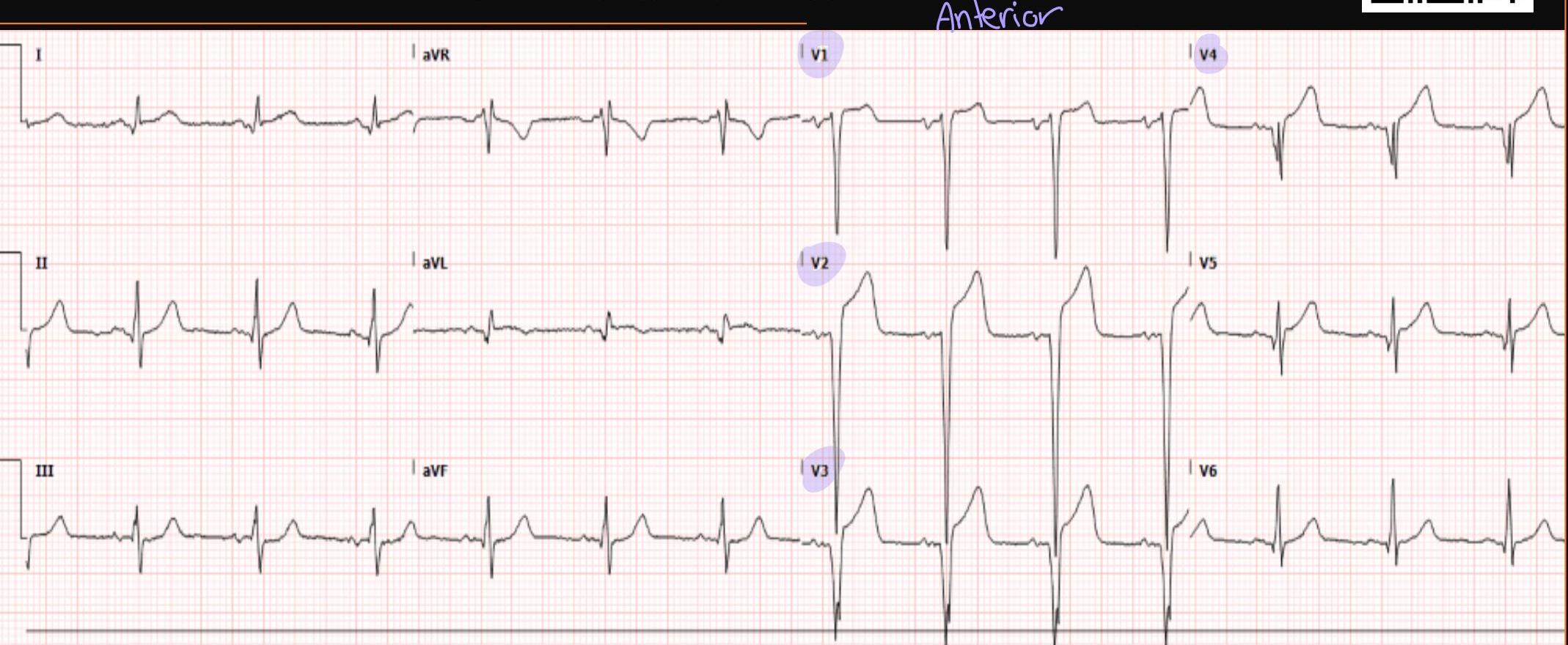
ECG Localization in STEMI
ECG shows:
- ST elevation in V1-5
- Deep QS waves in V2-V4
- Small Q waves in V5 and V6


STEMI Confirmed — What is the Next Step?
Immediately assess eligibility for coronary reperfusion therapy

Coronary Reperfusion Therapy

Reperfusion Options
| Therapy | Description |
|---|---|
| PCI | Percutaneous coronary intervention — Gold-standard treatment |
| Fibrinolysis | Thrombolytic therapy |
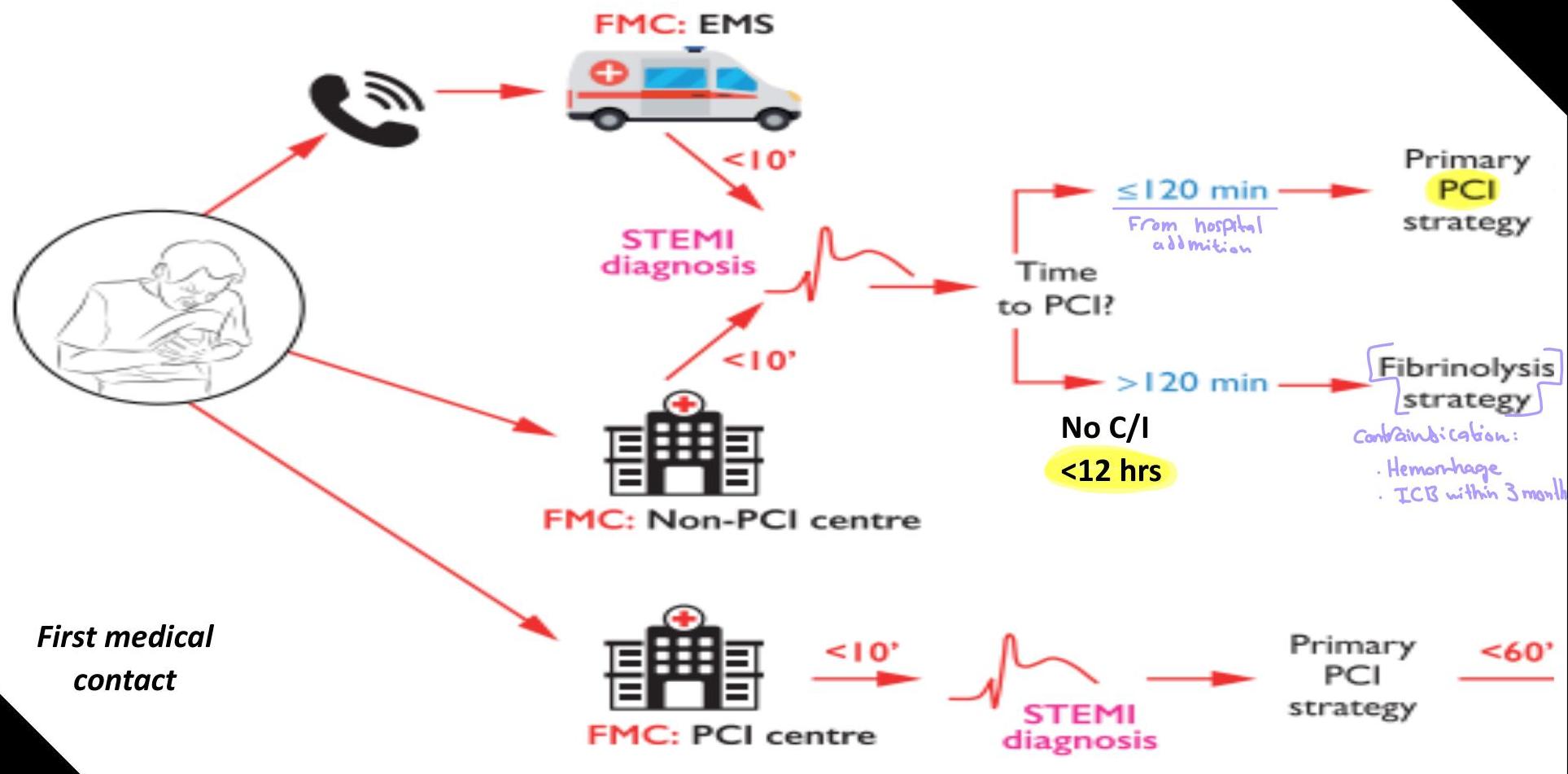
When Time is Muscle
Few minutes can save a life


Flowchart for STEMI
STEMI: Early Management (NICE Guidelines)
NICE — National Institute for Health and Care Excellence
Immediate Actions
- Offer a 300-mg loading dose of aspirin as soon as possible and continue aspirin indefinitely unless contraindicated
- Do NOT offer routine GPIs or fibrinolytic drugs before arrival at the catheter laboratory if primary PCI planned
- Immediately assess eligibility (irrespective of age, ethnicity, sex or level of consciousness) for reperfusion therapy
- If eligible, offer reperfusion therapy as soon as possible. Otherwise offer medical management
Medical Management
- Offer ticagrelor with aspirin unless high bleeding risk
- Consider clopidogrel with aspirin, or aspirin alone, for high bleeding risk
Cardiology Assessment
- Offer cardiology assessment
- Assess left ventricular function
Reperfusion Therapy (Primary PCI or Fibrinolysis)
Angiography with Follow-on Primary PCI
- Offer if:
- Presenting within 12 hours of symptoms AND PCI can be delivered in 120 mins
- Consider if:
- Presenting more than 12 hours after symptoms AND continuing myocardial ischaemia or cardiogenic shock
- Consider radial in preference to femoral access
Drug Therapy for Primary PCI
- Offer prasugrel* with aspirin if NOT already taking oral anticoagulant
- Offer clopidogrel with aspirin if taking an oral anticoagulant
- Offer unfractionated heparin with bailout GPI for radial access
- Consider bivalirudin with bailout GPI if femoral access needed
* For people aged 75 and over, think about whether risk of bleeding with prasugrel outweighs its effectiveness; if so offer ticagrelor or clopidogrel as alternatives
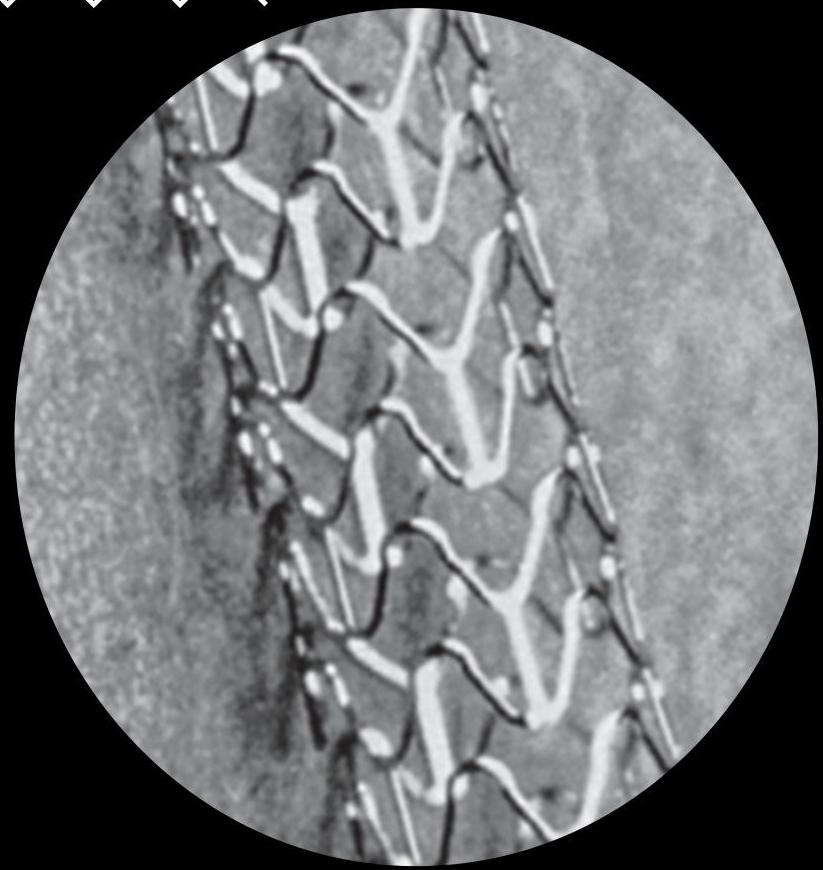
Stenting and Revascularisation
- If stenting indicated, offer a drug-eluting stent
- Offer complete revascularisation (consider doing this in the index admission) if:
- Multivessel coronary artery disease
- No cardiogenic shock
- Consider culprit only during the index procedure for cardiogenic shock
Fibrinolysis
- Offer if:
- Presenting within 12 hours of symptoms
- PCI not possible in 120 mins
- Give an antithrombin at the same time
- Offer ECG 60-90 mins after fibrinolysis
- Offer ticagrelor with aspirin unless high bleeding risk
- Consider clopidogrel with aspirin, or aspirin alone, for high bleeding risk
- Do NOT repeat fibrinolysis; offer immediate angiography with follow-on PCI if indicated by ECG
- Seek specialist advice for recurrent myocardial ischaemia and offer angiography with follow-on PCI if appropriate
- Consider angiography during same admission if stable after successful fibrinolysis
- Assess left ventricular function
Cardiac Rehabilitation and Secondary Prevention
This is a summary of the recommendations on early management of STEMI from NICE’s guideline on acute coronary syndromes. See the guideline at NG183.
© NICE 2020. All rights reserved. Subject to Notice of rights.

Simplified Management of STEMI

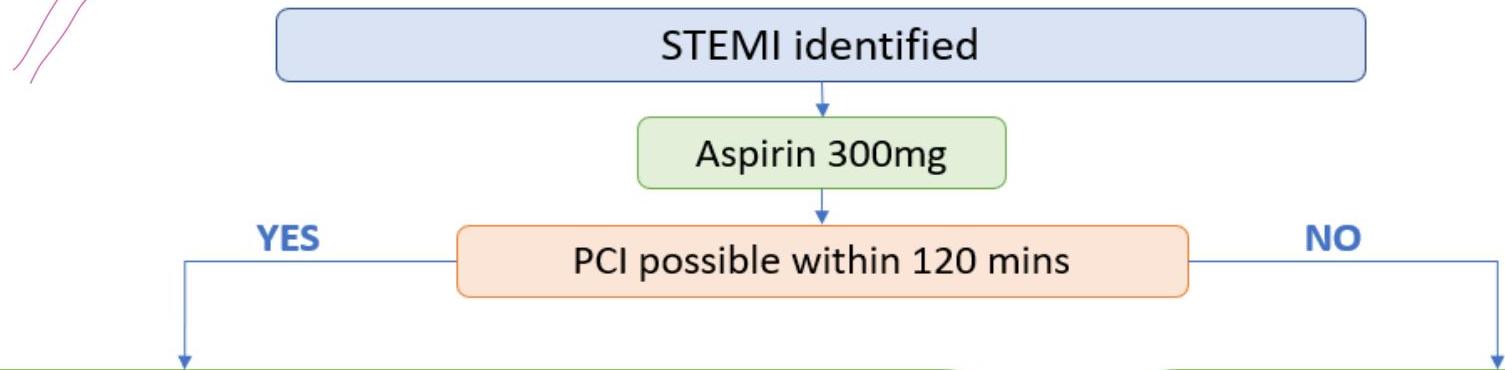
Flowchart Overview
STEMI identified
↓
Aspirin 300mg
↓
Can PCI be done within 120 mins?
- YES → Proceed to PCI
- NO → Proceed to Fibrinolysis
PCI Pathway
- Give prasugrel
- Radial access is preferred
- Give unfractionated heparin + bailout glycoprotein IIb/IIIa inhibitor
- Drug-eluting stents should be used in preference
Fibrinolysis Pathway
- Give an antithrombin at the same time
- Following procedure give ticagrelor
- For ongoing myocardial ischaemia consider PCI
Assumptions
- Patient presents within 12 hours of symptom onset
- If patient presents after 12 hours consider PCI if ongoing myocardial ischaemia or cardiogenic shock
- Patient is NOT a high bleeding risk
- If high bleeding risk: consider swapping prasugrel for ticagrelor / swapping ticagrelor for clopidogrel
- Patient is NOT on oral anticoagulants
- If on oral anticoagulants: swap prasugrel for clopidogrel
PassMedicine
STEMI PCI: Detailed Steps
| Step | Action |
|---|---|
| Step 1 | STEMI identified |
| Step 2 | Aspirin 300mg |
| Step 3 | PCI |
Prior PCI (Dual Antiplatelet Therapy)
| Patient Status | Antiplatelet Regimen |
|---|---|
| NOT on oral anticoagulant | Aspirin + prasugrel |
| ON oral anticoagulant | Aspirin + clopidogrel |
Drug Therapy During PCI
| Access Route | Anticoagulant Strategy |
|---|---|
| Radial access | • Unfractionated heparin with bailout glycoprotein IIb/IIIa inhibitor (GPI) |
| Femoral access | • Bivalirudin with bailout GPI |
Other Procedures
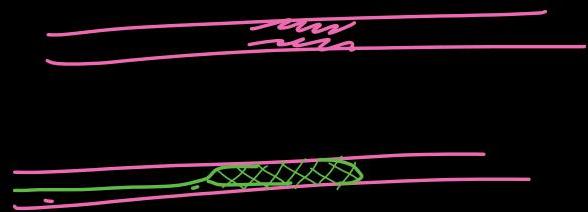
- Thrombus aspiration — Not mechanical extraction
- Drug-eluting stents
What is PCI?
PCI Timeframe
- A primary PCI strategy is recommended over fibrinolysis; if the presentation is within 12 hrs of onset of symptoms AND PCI can be delivered within 120 mins
- Consider PCI if fail fibrinolysis evident by ECG at 90 minutes showing non-resolution of the ST elevation
- If patients present after 12 hrs and evidence of ongoing ischaemia → rescue PCI
- Radial access is preferred to femoral access
PCI Complications
Periprocedural Complications
- Minor bleeding/haematoma
- Retroperitoneal haematoma
- Cholesterol embolization
- oligouria – short down at kidney – perforic rash
- Cardiac tamponade
Longer Term Complications
- Restenosis — first 3-6 months (5-20%)
- Stent thrombosis — First month (1-2%)
Fibrinolysis (When PCI Not Available)
If patient NOT for PCI
- If primary PCI cannot be delivered within 120 mins
- Thrombolytic drugs activate plasminogen to form plasmin “Actilyse”
- Tissue plasminogen activator (tPA) shown clear mortality benefits over streptokinase
Disadvantages:
- Hypotension
- Allergic reaction
Dosing:
- 100 mg total dose infused over 1.5 hr
- 15 mg IVP bolus over 1-2 minutes, remaining as an IV infusion



Contraindications for Fibrinolysis
| Category | Contraindications |
|---|---|
| Active Bleeding | Bleeding disorder; coagulopathy, Any prior intracranial bleeding, Not menses |
| Prior Surgery | Intracranial or intraspinal (2 months), Head trauma (3 months) |
| Intracranial Conditions | Ischemic stroke (3 months), AV malformation, Malignancy |
| Others | Suspected Aortic dissection, Unresponsive severe hypertension, Previous use of streptokinase (6 months) |
Fibrinolysis Steps
| Step | Action |
|---|---|
| Step 1 | STEMI identified |
| Step 2 | Aspirin 300mg |
| Step 3 | PCI not possible within 120 minutes → Fibrinolysis |
| Step 4 | Give antithrombin |
| Step 5 | After procedure → give ticagrelor |
| Step 6 | Repeat ECG after 60-90 minutes |
| Step 7 | Fail to resolve → Rescue PCI |
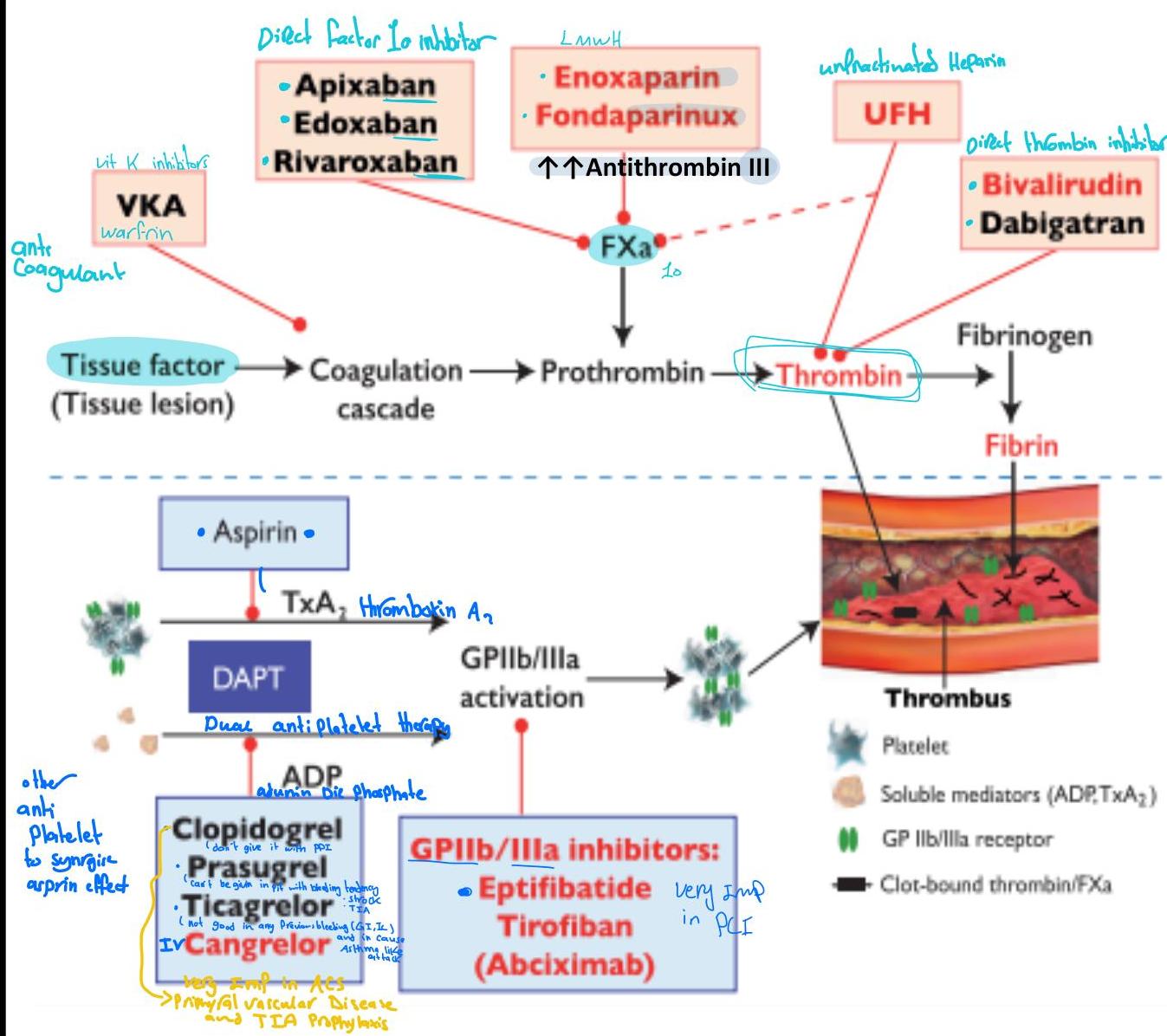
Antithrombotic Treatments

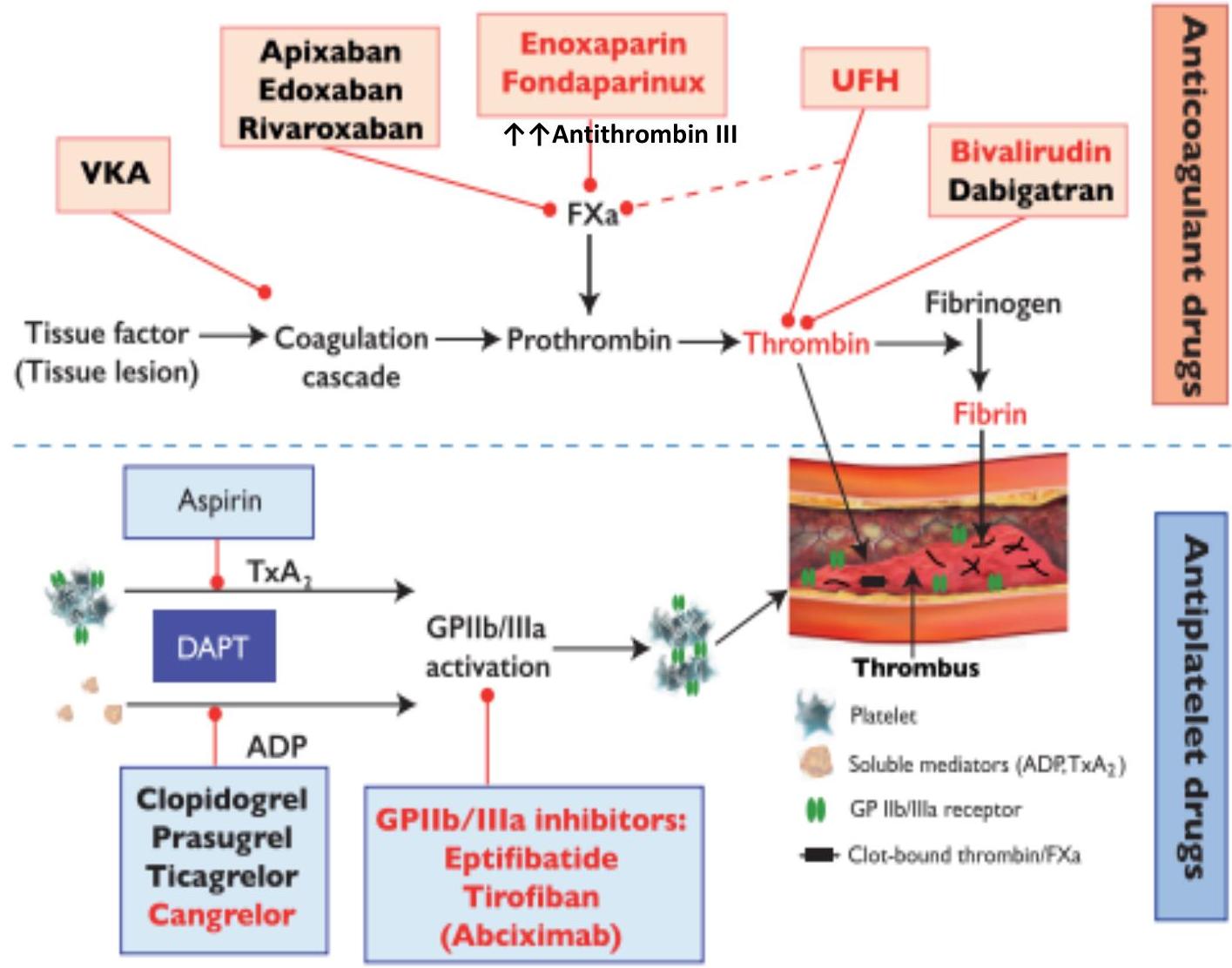
Antithrombotic treatments include:
- Anticoagulant drugs
- Antiplatelet drugs
Drugs Used for Management of ACS
| Drug Name | Mechanism of Action (MOA) |
|---|---|
| Heparin | Activates anti-thrombin III |
| Clopidogrel, Ticagrelor, Prasugrel | P2Y12 inhibitor |
| Abciximab | Glycoprotein IIb/IIIa inhibitor |
| Dabigatran | Direct thrombin inhibitor |
| Rivaroxaban | Direct factor X inhibitor |
| Fondaparinux | Activates antithrombin III, which in turn potentiates the inhibition of coagulation factors Xa |
| Bivalirudin | Reversible direct thrombin inhibitor |
Dual Antiplatelet Treatment (DAPT)
Drug Selection Guide
- Ticagrelor → In anti-thrombolytic therapy
- Prasugrel → PCI
- If bleeding tendency: “give Ticagrelor”
- If patient on anticoagulant: “give Clopidogrel”
Rationale for DAPT
- Aspirin and ADP inhibitors work by blocking different platelet aggregation pathways (potential synergy)
- Clopidogrel: ADP inhibitor; due to its interindividual variability in antiplatelet effects, newer agents (prasugrel and ticagrelor) were developed
NICE Guidelines Recommendations
- Marked reduction in short- and long-term ischaemic events when using prasugrel and aspirin, compared to clopidogrel and aspirin in moderate- to high-risk ACS patients
- Starting DAPT with Aspirin and Ticagrelor for 12 months, as a secondary prevention strategy
NSTEMI/Unstable Angina: Simplified Management
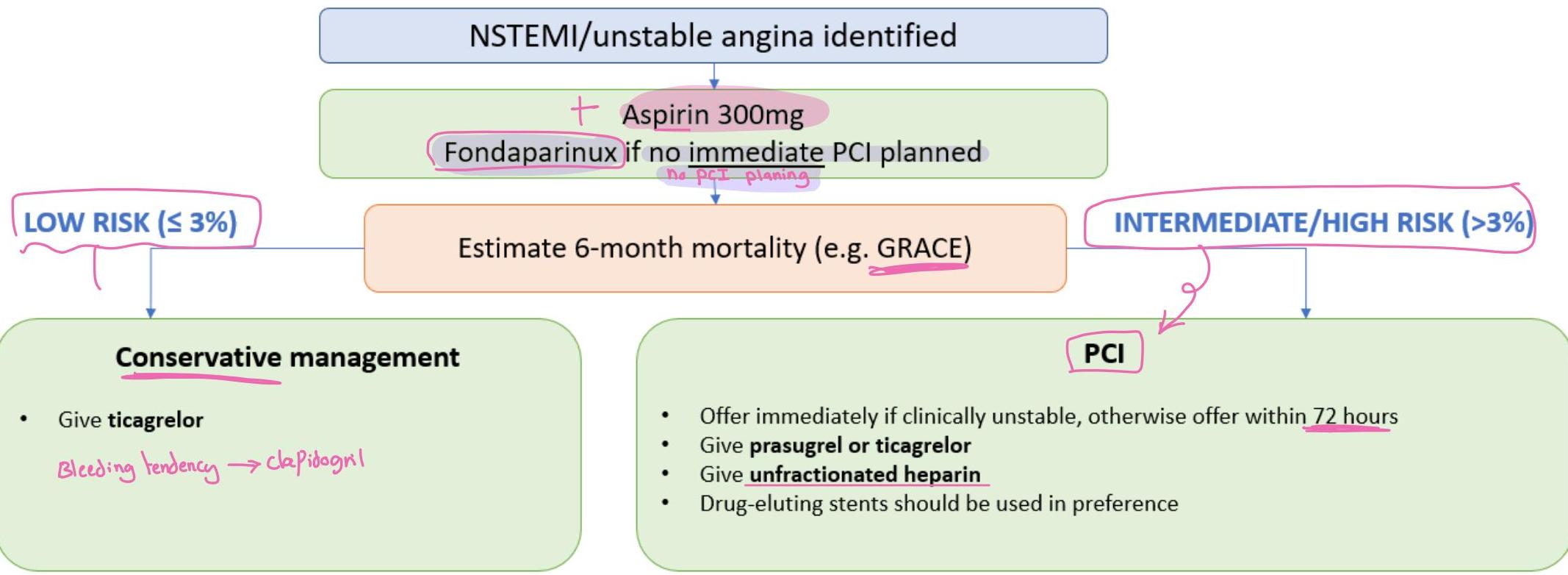
Conservative Management
- Give ticagrelor
- Bleeding tendency → clopidogrel
PCI for NSTEMI
- Offer immediately if clinically unstable
- Otherwise offer within 72 hours
- Give prasugrel or ticagrelor
- Give unfractionated heparin
- Drug-eluting stents should be used in preference
Assumptions
- Patient is NOT a high bleeding risk
- If high bleeding risk consider:
- Swapping fondaparinux for an alternative antithrombin/dose
- Swapping prasugrel for ticagrelor / swapping ticagrelor for clopidogrel
- If high bleeding risk consider:
- Patient is NOT on oral anticoagulants
- If on oral anticoagulants: swap prasugrel/ticagrelor for clopidogrel
PassMedicine
NSTEMI High Risk Group: Management Steps
| Step | Action |
|---|---|
| Step 1 | NSTEMI identified |
| Step 2 | Aspirin 300mg |
| Step 3 | Fondaparinux (if no risk of bleeding & no immediate PCI) |
| OR Unfractionated heparin: if immediate PCI planned or creatinine is > 265 μmol/L | |
| Step 4 | Risk assessment using GRACE score (The Global Registry of Acute Coronary Events) |
| Step 5 | Immediate PCI (if unstable) |
| OR PCI after 72 hours (if stable patient) | |
| Step 6 | Prior PCI (Dual AP therapy): |
| • Aspirin + Prasugrel or ticagrelor (if NOT on oral anticoagulant) | |
| • Clopidogrel (if on oral anticoagulant) | |
| • Change ticagrelor to Prasugrel | |
| • Change Prasugrel to clopidogrel (if high bleeding risk) | |
| Step 7 | Unfractionated heparin should be given regardless of fondaparinux or not |
NSTEMI Low Risk Group: Management Steps
| Step | Action |
|---|---|
| Step 1 | NSTEMI identified |
| Step 2 | Aspirin 300mg |
| Step 3 | Fondaparinux (if no risk of bleeding & no immediate PCI) |
| OR Unfractionated heparin: if immediate PCI planned or creatinine is > 265 μmol/L | |
| Step 4 | Risk assessment using GRACE score (The Global Registry of Acute Coronary Events) |
| Step 5 | Conservative management with ticagrelor (no risk of bleeding) |
| OR Conservative management with clopidogrel (no risk of bleeding) |
GRACE Score: The Global Registry of Acute Coronary Events
GRACE Score Components:
- Heart rate, blood pressure
- Cardiac (Killip class) and renal function (serum creatinine)
- Cardiac arrest on presentation
- ECG findings
- Troponin levels

GRACE ACS Risk and Mortality Calculator
Estimates admission-6 month mortality for patients with acute coronary syndrome.
| Parameter | Normal Range | Unit |
|---|---|---|
| Age | 0 - 0 | years |
| Heart rate/pulse | 60 - 100 | beats/min |
| Systolic BP | 100 - 120 | mm Hg |
| Creatinine | 62 - 115 | μmol/L |
| Cardiac arrest at admission | No / Yes | |
| ST segment deviation on EKG? | No / Yes | |
| Abnormal cardiac enzymes | No / Yes | |
| Killip class (signs/symptoms) | ||
| • No CHF | ||
| • Rales and/or JVD | ||
| • Pulmonary edema |
Antiplatelet Therapy by Diagnosis
| Diagnosis | 1st Line | 2nd Line |
|---|---|---|
| Acute coronary syndrome (medically treated) | Aspirin (lifelong) + Ticagrelor (12 months) | If aspirin contraindicated: Clopidogrel (lifelong) |
| Percutaneous coronary intervention | Aspirin (lifelong) + Prasugrel or Ticagrelor (12 months) | If aspirin contraindicated: Clopidogrel (lifelong) |
| TIA | Clopidogrel (lifelong) | Aspirin (lifelong) + Dipyridamole (lifelong) |
| Ischaemic stroke | Clopidogrel (lifelong) | Aspirin (lifelong) + Dipyridamole (lifelong) |
| Peripheral arterial disease | Clopidogrel (lifelong) | Aspirin (lifelong) |
ACS Complications
This Photo — CC BY-SA
Cardiogenic Shock
Heart Failure
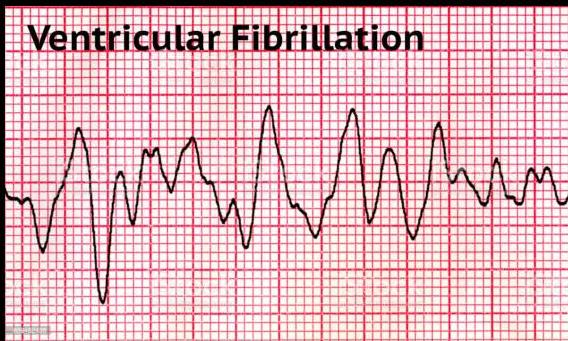
Ventricular Tachycardia
This Photo — CC BY-SA
Acute MR, VSD
CC BY-SA
This Photo — CC BY-SA
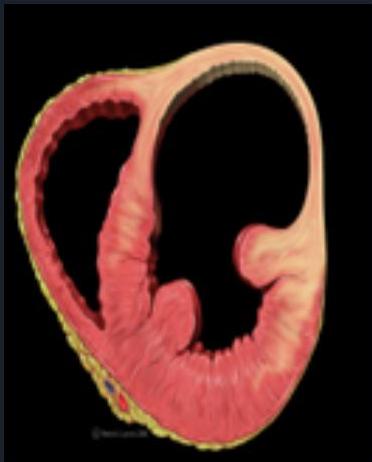
Left Ventricular Aneurysm
Persistent ST elevation

ACS: Poor Prognostic Factors
| Factor Category | Specific Factors |
|---|---|
| Demographics | Age |
| Cardiac History | Development (or history) of heart failure, Killip class* |
| Vascular | Peripheral vascular disease |
| Hemodynamics | Reduced systolic blood pressure |
| Renal | Initial serum creatinine concentration |
| Biomarkers | Elevated initial cardiac markers |
| Events | Cardiac arrest on admission |
* Stable angina: β-blocker / CCB if patient on 2 anti-anginal medications and still symptomatic PCI if one vessel NOT LAD CABG in triple vessel CAD or LAD
ST segment elevation
Myocardial Infarction: Secondary Prevention
Case Study
Patient: 65 y/o with chest tightness after walking, stops when he rests.
Current Medications:
- Aspirin
- Statin
- CCB
Comorbidity: Asthma
Question: What to give to control his symptoms? (Angina)
Answer:
- Cannot give β-blocker — Patient is asthmatic
- Cannot combine 2 CCBs
- Best to give Ranolazine
Lifestyle Modifications
- Diet
- Exercise: advise 20-30 mins a day
Special Considerations
- PDE5 inhibitors (e.g., sildenafil) — use 6 months after MI
- DVLA:
- ACS → 4 weeks off driving
- 1 week if successfully treated by angioplasty
Standard Drug Therapy
All patients should be offered the following drugs:
☑ Dual antiplatelet therapy (aspirin plus a second antiplatelet agent)
- Post ACS (medically managed): add ticagrelor to aspirin, stop ticagrelor after 12 months
- Post PCI: add prasugrel or ticagrelor to aspirin, stop the second antiplatelet after 12 months
☑ ACE inhibitor
☑ Beta-blocker
☑ Statin
☑ If patient came with episode of Heart Failure:
- Aldosterone antagonists (e.g., eplerenone) — initiated within 3-14 days if HF
Additional Case Example
Patient: Has chest tightness after walking approximately 180 meters. Stops when he rests.
PMH:
- Hypertension
- Asthma
Medications:
- Aspirin
- Atorvastatin
- Naltrexone
- Regular inhaler
Examination: Uncomfortable
BP: 154/42 mmHg
Question: What is the most appropriate choice of medication to control his symptoms?
Options:
- A. Atenolol
- B. Bisoprolol
- C. Diltiazem
- D. Venlafaxine

This Photo by Unknown Author is licensed under CC BY-NC-ND
Clinical Cases: Multiple Choice Questions
Case 1: STEMI Identified — Next Step?
Scenario: STEMI identified — what is the best next step in the management of this patient with an ACS? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give aspirin 300mg + fondaparinux (NSTEMI)
- B. Conservative management — give ticagrelor
- C. PCI within 72 hours
- D. Femoral access, give unfractionated heparin, use drug-eluting stent
- E. Give aspirin 300mg ✓
- F. Radial access, give unfractionated heparin, use drug-eluting stent
Case 2: STEMI — Aspirin Given, Having PCI
Scenario: STEMI identified, aspirin given, having PCI — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give prasugrel ✓
- B. PCI within 72 hours
- C. Give clopidogrel 300mg
- D. Radial access, give unfractionated heparin, use drug-eluting stent
- E. Give clopidogrel 75mg
- F. Femoral access, give unfractionated heparin, use drug-eluting stent
Case 3: STEMI — Aspirin Given, Next Step?
Scenario: STEMI identified, aspirin given, what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Assess 6-month mortality using a tool such as GRACE
- B. Assess whether PCI possible within 120 minutes ✓
- C. PCI within 72 hours
- D. Femoral access, give unfractionated heparin, use drug-eluting stent
- E. Give ticagrelor
- F. Give prasugrel
Case 4: 70-Year-Old with STEMI
Scenario: 70-year-old man with chest pain, STEMI changes on ECG, pulse 102/min, BP 160/90 mmHg, sats 93%
Question: What is the most appropriate immediate management?
Options:
- A. Aspirin, nitrates, morphine, clopidogrel, contact cardiothoracic surgeon for immediate CABG
- B. Aspirin, nitrates, morphine, clopidogrel, calculate GRACE score
- C. Aspirin, nitrates, morphine, prasugrel, arrange immediate PCI
- D. Aspirin, nitrates, morphine, oxygen, prasugrel, arrange immediate PCI ✓
- E. Aspirin, nitrates, morphine, clopidogrel, arrange immediate thrombolysis
Case 5: STEMI — PCI Done, Prasugrel Given
Scenario: STEMI identified, aspirin given, PCI done, prasugrel given — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give abciximab
- B. Assess 6-month mortality using a tool such as GRACE ✓
- C. Give clopidogrel 300mg
- D. Give prasugrel or ticagrelor
- E. Radial access, give unfractionated heparin, use drug-eluting stent
- F. Femoral access, give unfractionated heparin, use drug-eluting stent
Case 6: STEMI — Fibrinolysis + Antithrombin Given
Scenario: STEMI identified, aspirin given, has had fibrinolysis + antithrombin given — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. PCI within 72 hours
- B. Give clopidogrel 300mg
- C. Give ticagrelor ✓
- D. Femoral access, give unfractionated heparin, use drug-eluting stent
- E. Give aspirin 300mg + fondaparinux
- F. Assess 6-month mortality using a tool such as GRACE
Case 7: 60-Year-Old with NSTEMI
Scenario: 60-year-old man with chest pain, NSTEMI changes on ECG, pulse 66/min, BP 130/82 mmHg, sats 98%
Question: What is the most appropriate immediate management?
Options:
- A. Aspirin, nitrates, morphine, prasugrel, arrange immediate PCI
- B. Aspirin, nitrates, morphine, oxygen, prasugrel, arrange immediate PCI
- C. Aspirin, nitrates, morphine, clopidogrel, arrange immediate thrombolysis
- D. Aspirin, nitrates, morphine, clopidogrel, contact cardiothoracic surgeon for immediate CABG
- E. Aspirin, nitrates, morphine, prasugrel, arrange transvenous pacing wire
- F. Aspirin, nitrates, morphine, clopidogrel, calculate GRACE score ✓
Case 8: NSTEMI — Aspirin Given, Next Step?
Scenario: NSTEMI identified, aspirin given, what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give prasugrel or ticagrelor
- B. Give ticagrelor
- C. Give aspirin 75mg
- D. Assess 6-month mortality using a tool such as GRACE ✓
- E. Radial access, give unfractionated heparin, use drug-eluting stent
- F. Conservative management — give ticagrelor
Case 9: NSTEMI — Intermediate/High Risk
Scenario: NSTEMI identified, aspirin given, 6-month mortality intermediate/high (>3%) — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Femoral access, give unfractionated heparin, use drug-eluting stent
- B. Give prasugrel or ticagrelor
- C. Radial access, give unfractionated heparin, use drug-eluting stent
- D. PCI within 72 hours ✓
- E. Give prasugrel
- F. Give aspirin 75mg
Case 10: NSTEMI — Having PCI Within 72 Hours
Scenario: NSTEMI identified, aspirin given, intermediate/high risk, having PCI within 72 hours — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give an antithrombin ✓
- B. Give clopidogrel 75mg
- C. Give aspirin 300mg + fondaparinux
- D. Give clopidogrel 300mg
- E. Assess whether PCI possible within 120 minutes
- F. Give prasugrel or ticagrelor
Case 11: NSTEMI — Initial Step
Scenario: NSTEMI identified — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give clopidogrel 300mg
- B. Assess 6-month mortality using a tool such as GRACE ✓
- C. Conservative management — give ticagrelor
- D. Give aspirin 75mg
- E. PCI within 72 hours
- F. Give aspirin 300mg + fondaparinux
Case 12: STEMI — Having Fibrinolysis
Scenario: STEMI identified, aspirin given, having fibrinolysis — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give an antithrombin ✓
- B. Radial access, give unfractionated heparin, use drug-eluting stent
- C. PCI within 72 hours
- D. Give ticagrelor
- E. Give aspirin 75mg
- F. Give abciximab
Case 13: NSTEMI — Low Risk
Scenario: NSTEMI identified, aspirin given, 6-month mortality low (<3%) — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Assess whether PCI possible within 120 minutes
- B. Conservative management — give ticagrelor ✓
- C. Radial access, give unfractionated heparin, use drug-eluting stent
- D. Give prasugrel
- E. PCI within 72 hours
- F. Give prasugrel or ticagrelor
Case 14: NSTEMI — Ticagrelor Given, Having PCI
Scenario: NSTEMI identified, aspirin given, intermediate/high risk, ticagrelor given, having PCI — what is the best next step? (assume normal bleeding risk and NOT on anticoagulants)
Options:
- A. Give clopidogrel 75mg
- B. Radial access, give unfractionated heparin, use drug-eluting stent ✓
- C. Assess 6-month mortality using a tool such as GRACE
- D. Give prasugrel or ticagrelor
- E. Give abciximab
- F. Femoral access, give low-molecular weight heparin, use bare-metal stent
Take Away Messages
-
Great attention — Not to miss ACS among:
- Elderly patients
- Women
- Diabetic patients
-
PCI has revolutionized ACS management
-
DUAL platelet therapy is the recommended preventive medication
-
Risk stratification of patient is important for ACS management
Summary Images



Quiz Time
READY FOR A QUIZ?

