ASCITES
DR WAQAR MBBS, MRCP, Int. Medicine (London) Specialist cert. exam, Endocrinology & DM (London) ASST. PROFESSOR
Leenah Turjoman ♥
DEFINITION
- Accumulation of more than 25 cc of fluid in the peritoneal cavity is called ascites.
(normally, only about 25 cc fluid in the cavity)
(little amount of fluid is needed in the cavity so there is no friction among intestines)
At least 1.5 L fluid should be present in the abdomen so as to be detected by examination. If less than this, shifting dullness and fluid thrill will be negative.
So, how will you confirm?
25cc - 1.5L of fluid can be detected by US
ETIOLOGIES OF ASCITES
-
Liver disease (cirrhosis) → Cancer → lead to lack of albumin → so fluid go out in interstitial spaces → ascites normally keeps fluid in bed by oncotic pressure
-
Portal HTN → could be due to blood clot or pancreatitis
-
Low serum albumin due to any cause (cirrhosis, low protein diet, protein malabsorption, urinary albumin loss) → e.g. nephrotic syndrome
-
Heart failure (due to backpressure) → on the rt side → hepatomegaly → fluid comes out
-
Renal failure (due to fluid retention) → so fluid accumulation, leading to:
- ascites
- pleural effusion
- pulmonary edema
- pedal edema
-
Peritonitis → infection so all fluid comes out into peritoneal cavity
-
Mets to the peritoneum → so peritoneum becomes inflamed and fluid comes out in the cavity
STEP WISE APPROACH
- Take a detailed history, (keeping in view all the etiologies)
- Physical examination, (keeping in view all the etiologies)
- CBC, LFTs, Electrolytes, creatinine
- Ascitic fluid analysis
- Imaging studies, (keeping in view all the etiologies)
CLASSIFICATION
Ascites can be divided into 2 main types according to the protein concentration of the fluid
- TRANSUDATE: Protein less than 30g/L in the ascitic fluid.
- EXUDATE: Protein more than 30 g/L A better way of classification is the SAAG ratio (Serum to Ascites Albumin Gradient)
(difference)
WHAT IS SAAG?
- Serum albumin minus ascitic fluid albumin (albumin difference)
- This difference can be more than 1.1g/100cc or less than 1.1g/100cc
So,
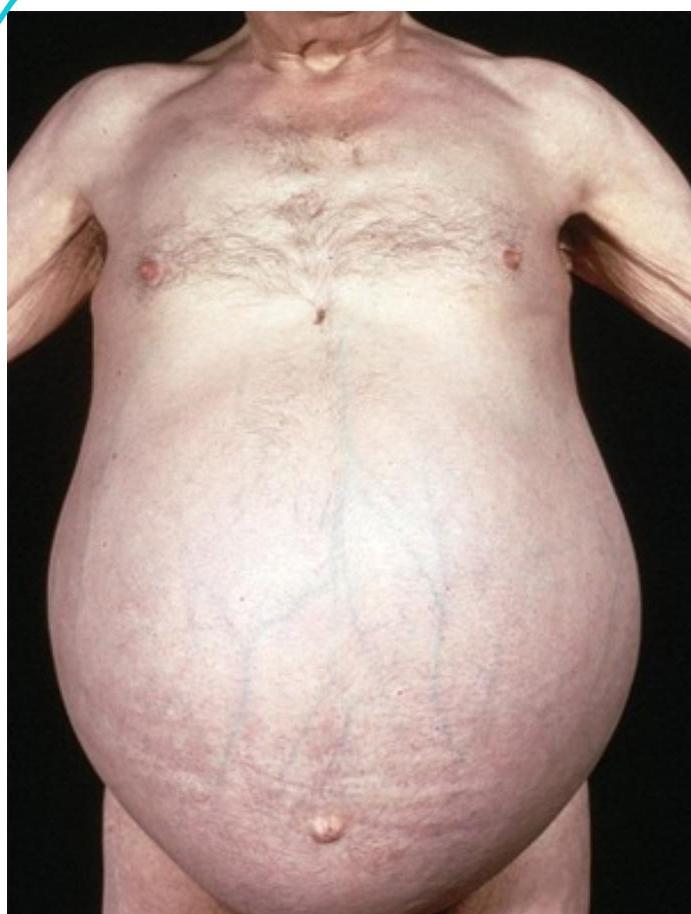
ASCITES
SAAG > 1.1
SAAG < 1.1
CAUSES OF ASCITES
SAAG > 1.1
a) Cirrhosis with/portal HTN b) Portal HTN due to any other cause c) Heart failure d) Renal failure
SAAG < 1.1
a) Bacterial & fungal peritonitis b) Tuberculous peritonitis d) Nephrotic syndrome e) Pancreatitis f) Low serum albumin g) Mets to the peritoneum
Some other types of Ascites
-
Hemorrhagic ascites: due to malignancy either mets or malignancy of Peritoneum
-
Chylous ascites: Collection of lymph in the abdominal cavity. Rich in fats milky appearance. (eg in lymphomas, TB peritonitis) These conditions cause damage to lymphatic channels so lymph comes out into peritoneal cavity
Triglycerides are carried with proteins in the blood, they are not water soluble
(Chilomicrons = Triglycerides = Fat)
ASCITES
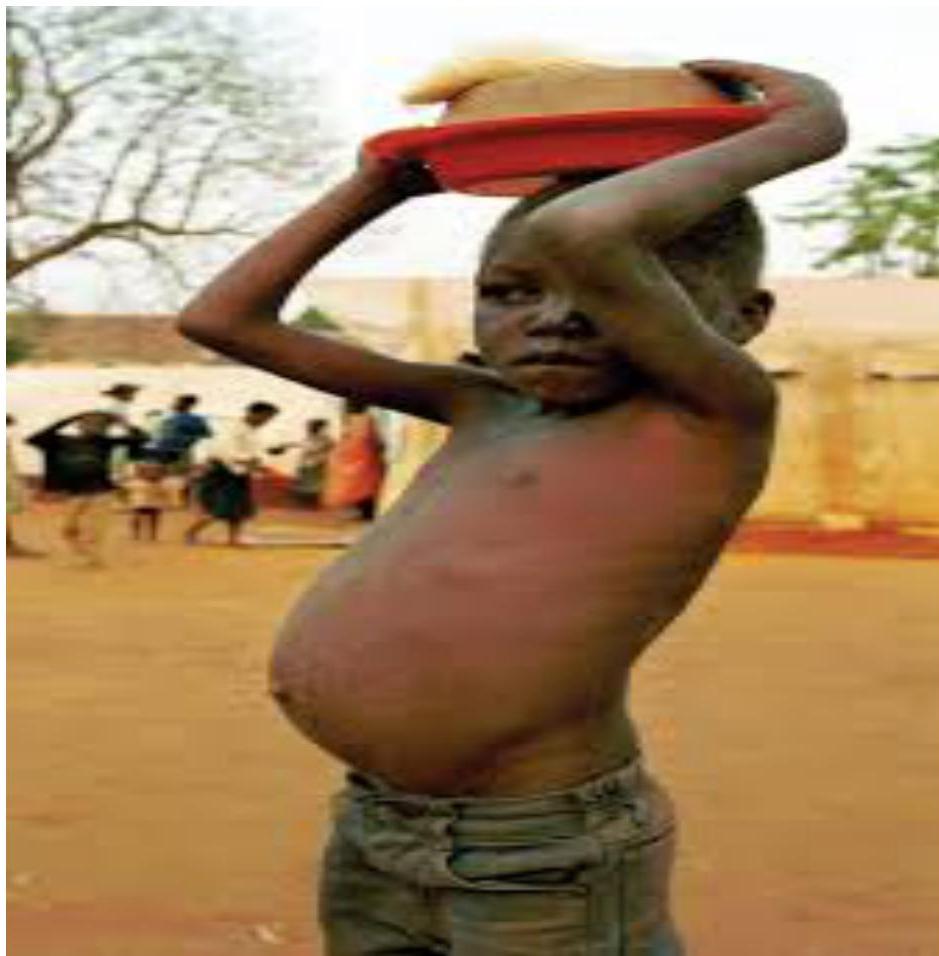
ASCITES DUE TO KWASHIORKOR
INVESTIGATIONS IN ASCITES
- Paracentesis(ascitic tap). Every new patient with ascites should get a “diagnostic” tap:
- Take out 10-20 cc fluid
- Check albumin (to calculate SAAG), neutrophils (to see infection), RBC, Gram stain & culture, cytology (malignant cells), amylase levels (in suspected pancreatic ascites) → not routinely done
MANAGEMENT OF ASCITES
Low salt & Diuretics Paracentesis water intake (because salt retains water in the body)
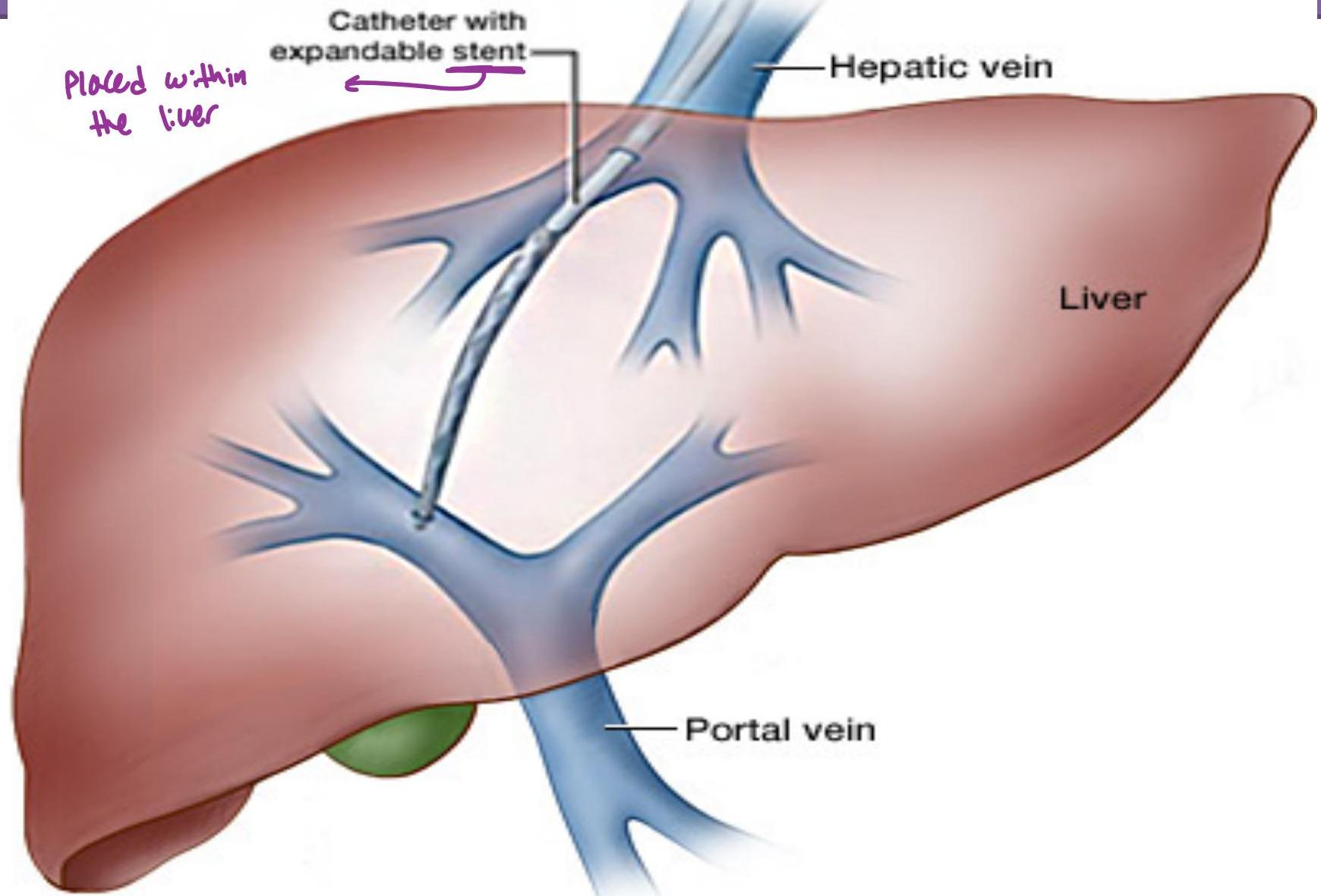
In very resistant ascites, a procedure called TIPS is sometimes used. (transjugular intrahepatic porto-systemic shunt).
> Joining Portal with hepatic circulation so pressure in Portal vein is diverted to hepatic system > (reducing pressure in Portal vein)
TIPS
MANAGEMENT OF ASCITES
- Low salt & water: < 2 g/d of salt (less than ½ tea spoon)
- Diuretics:
- Spironolactone (aldactone). 1st choice. → in liver disease
- side effects: gynecomastia, hyperkalemia
- Can add lasix (furosemide) if needed
- Reduce ascites gradually (0.5 to 1 kg wt. loss daily). Too much wt. loss “suddenly” is not good! In 95% of cases, ascites can be controlled by 1) & 2)
Management contd.
- “Therapeutic Paracentesis”
- It is done if medicines don’t help (resistant ascites) or very big ascites causing respiratory difficulty.
- Upto 7 L can be removed at one time.
- Removal of more than 7L can cause problems like hypotension, renal failure, encephalopathy → Can also occur if rapidly reduce ascites by diuretics
- i.v. albumin given at the time of paracentesis can prevent these complications
Therapeutic Paracentesis
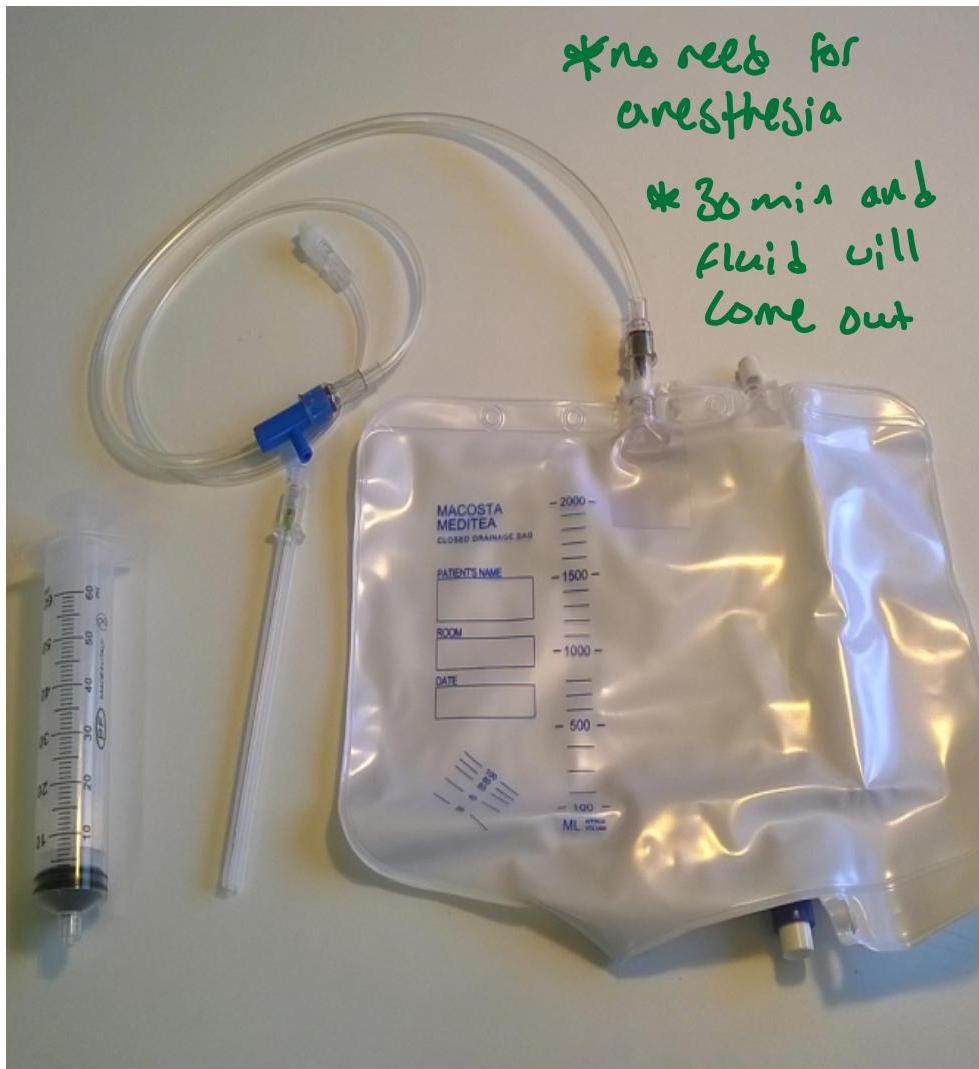
no need for anesthesia 30 min and fluid will come out

Complications of Ascites (contd)
Patient with liver cirrhosis, albumin is not synthesized, leading to ascites, but albumin is not given as treatment because albumin has very short half life, so practically can’t be given for life
- albumin not given for nephrotic syndrome because if give it, more albumin will be filtered through kidney and more damaging to kidney
So, remember 3 complications of ascites:
- SBP (Spontaneous bacterial peritonitis)
- Respiratory distress
- Umbilical hernia
How to Approach the patient
- Take a detailed history (keeping in view the causes of ascites)
- Do appropriate examination
- Order investigations
- Give treatment to remove the ascitic fluid
- Treat the cause
LAST SLIDE IS VERY IMPORTANT
TRY TO DO 1 SMALL GOOD THING EVERY DAY
- Greet people with a smile
- Give way to another car on the road.
- Talk nicely to a person who is lower than you financially or in position
Merci
