
Asthma Updated Guidelines
Lina Serhan 📝
Dr Nada Abdelrahman
This Photo by Unknown Author is licensed under CC BY-SA-NC
3/4/2024
Learning objectives
BY THE END OF THIS SESSION, THE STUDENT SHOULD BE ABLE TO
- Diagnose different types of asthmatic attack
- Manage different types and stages of asthma.
SAMPLE FOOTER TEXT
3/4/2024
Aetiology
Imbalance in the immune response, (type 2 T-helper (Th2) cell-mediated response → increase cytokines (IL)-4, IL-5, and IL-13, IL 25, IL33 promoting eosinophilic inflammation, immunoglobulin E (IgE) production, and airway hyperresponsiveness.
Environmental Factors

Genetic Factors
Immunological Factors
3/4/2024
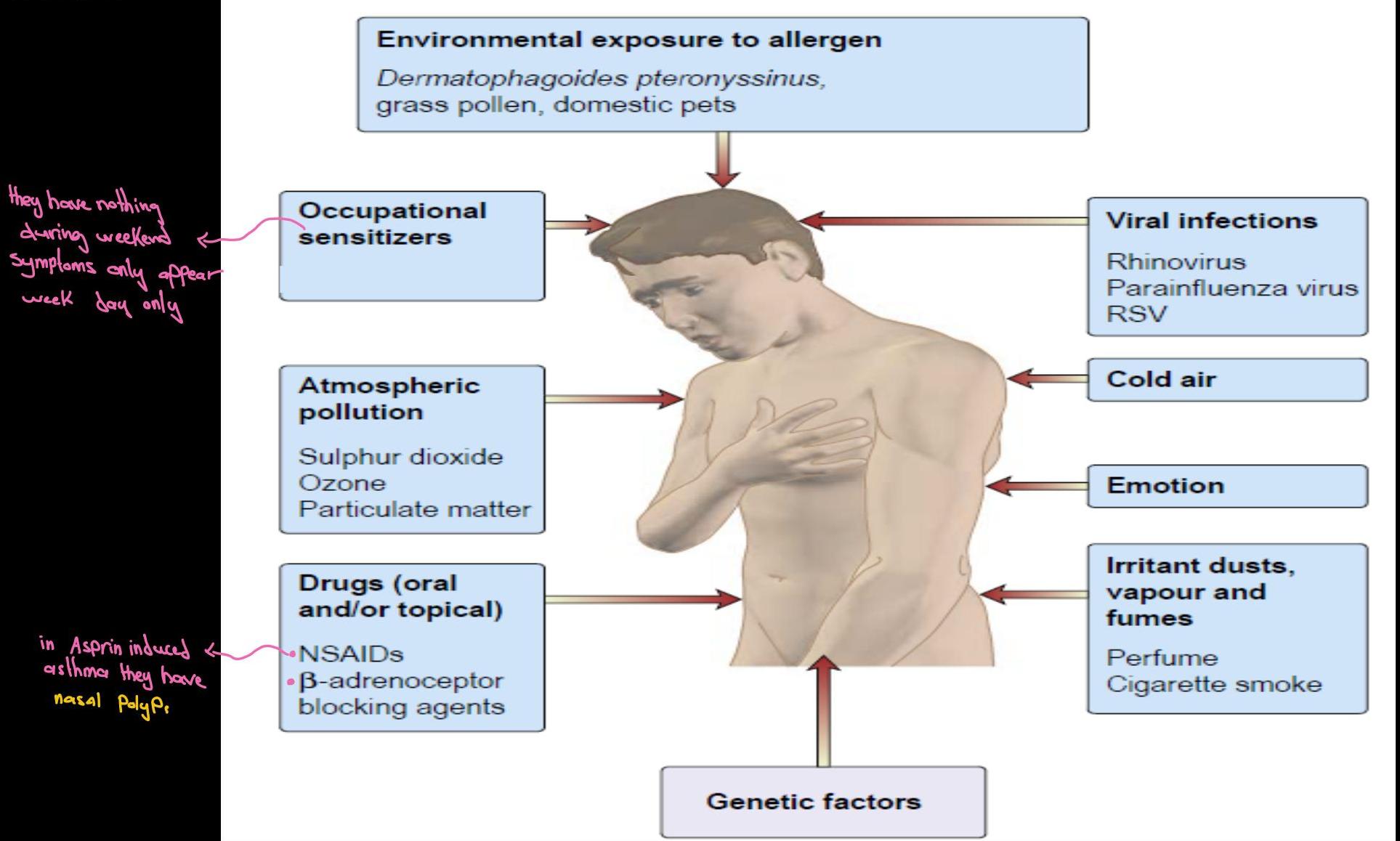 Environmental exposure to allergen
Dermatophagoides pteronyssinus, grass pollen, domestic pets
Environmental exposure to allergen
Dermatophagoides pteronyssinus, grass pollen, domestic pets
3/4/2024
Risk factors & associations
-
Personal or family history of atopy
-
IgE-mediated atopic
-
☑ atopic dermatitis (eczema)
-
☑ allergic rhinitis (hay fever)
-
Antenatal factors: maternal smoking, viral infection (RSV)
-
Low birth weight; not being breastfed baby at risk to get asthma.
-
Air pollution & exposure to allergens
-
‘hygiene hypothesis’: increased risk of asthma in developed countries → less exposure less Immunity
-
Sensitive to aspirin. Nasal polyps.
 This Photo by Unknown Author is licensed under CC BY-NC
This Photo by Unknown Author is licensed under CC BY-NC
3/4/2024
Pathophysiology of Asthma
Vides
6
3/4/2024
Investigations for asthma
-
Guidelines avoid subjective/clinical judgements and advocate objective tests. All patients >= 5 years should have objective tests.
-
☐ Fractional exhaled nitric oxide (FeNO). 3 types; inducible (iNOS) levels rise in inflammatory cells (eosinophils) & correlate with levels of inflammation. Positive: >= 40 parts per billion (ppb) Confirmatory with other tests
-
☐ Spirometry and peak flow variability Obstructive: FEV1/FVC ratio <70% obstructive pattern Could be with other diseases like: COPD
-
☐ Bronchodilator reversibility (BDR) test Positive test : by improvement in FEV1 of 12% or more (increase in volume of ≥200 ml)
-
☐ Exercise challenge test using histamine or methacholine Positive test : by reduction in FEV1 of >10-15% or more (decrease in volume of ≥200 ml)
3/4/2024
Video
Objectives
- The use of basic respiratory function tests:
- Spirometry
- Peak flow
- The interpretation of results.
Steps of investigation
- Measure FeNO
- DO Spirometry
- If obstruction BDR
- If negative– monitor Peak Flow variability (2-4 wk if there’s variability → this is asthma) if there’s no go to the next step
- If negative– histamine or methacholine challenge test
- If 5 unavailable; suspect and treat
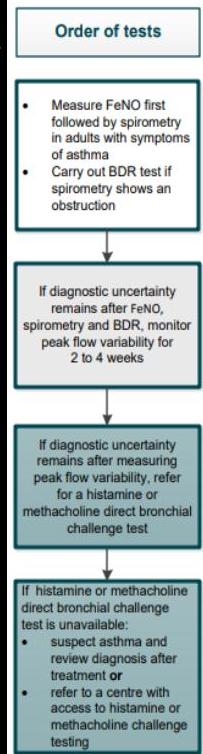
Algorithm C Objective tests for asthma in adults aged 17 and over
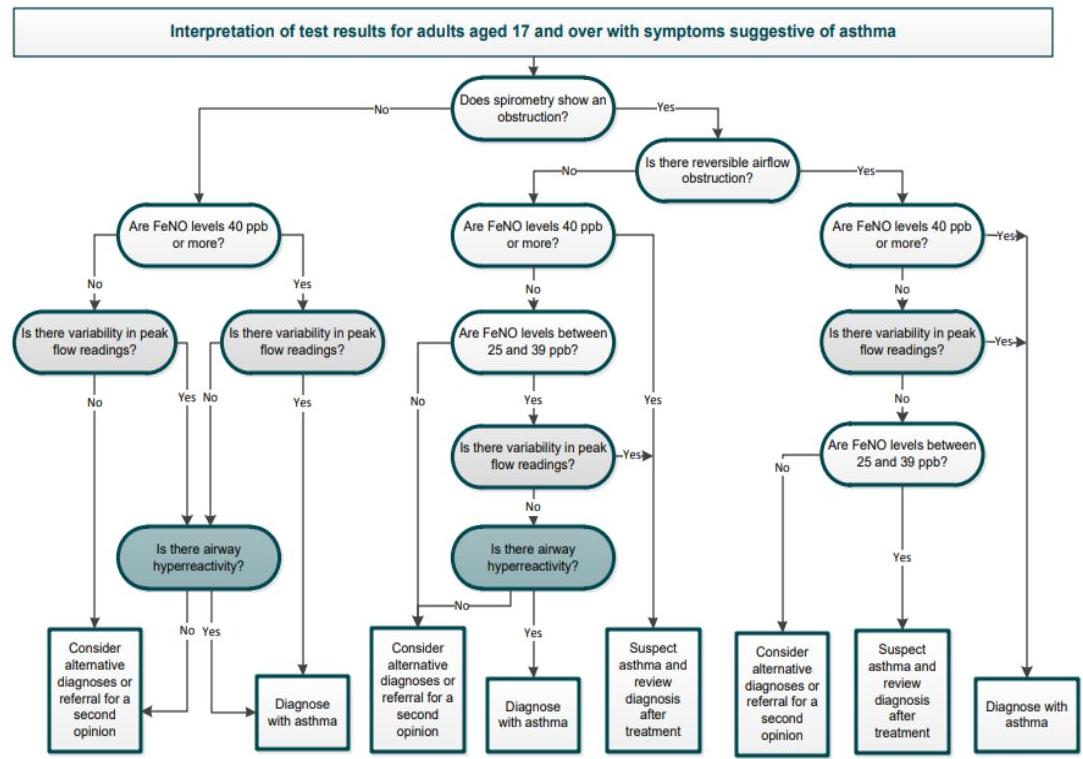
Interpretation of test results for adults aged 17 and over with symptoms suggestive of asthma
Abbreviations
FeNO, fractional exhaled nitric oxide BDR, bronchodilator reversibility
This algorithm is based on recommendations from NICE’s guideline on asthma, diagnosis, monitoring and chronic asthma management (2017)
Positive test thresholds
Obstructive spirometry: FEV1/FVC ratio less than 70% (or below the lower limit of normal if available) FV50: 40 ppb or more ACR, improvement in FEV1 of 12% or more and increase in volume of 200 ml or more T-1/4 flow variability: variability over 20% Direct bronchial challenge test with histamine or methacholine: FCO: of 8 mg/ml or less
NICE National Institute for Health and Care Excellence © NICE 2017. All rights reserved. Subject to Notice of rights
3/4/2024
Diagnosis should be based on objective tests
SAMPLE FOOTER TEXT 10
3/4/2024
Asthma classification
| Moderate | Severe | Life-threatening |
|---|---|---|
| • PEFR 50-75% best or predicted | ||
| • Speech normal | ||
| • RR < 25 / min | ||
| • Pulse < 110 bpm | • PEFR 33 - 50% best or predicted | |
| • Can’t complete sentences | ||
| • RR > 25/min | ||
| • Pulse > 110 bpm | • PEFR ≤ 33% best or predicted. | |
| • Oxygen sats < 92% | ||
| • ‘Normal’ pCO2 (4.6-6.0 kPa) due to Respiratory Fatigue | ||
| • Exhaustion, confusion or coma | ||
| • Silent chest, cyanosis or feeble respiratory effort | ||
| Bradycardia, dysrhythmia or hypotension. |
‘Near-fatal asthma’, is a raised pCO₂ and/or requiring mechanical ventilation with raised inflation pressures.
3/4/2024
Acute severe asthma
① ABC ② give oxygen ③ Iv Fluid and Steroid and if very severe and pit is able to swallow give oral prionstone ④ inhaler B agonist (salbutamol)
Management of acute severe asthma
Assess severity of attack
PEF, ability to speak, RR, pulse rate, O₂ sats Warn ICU if severe or life-threatening attack
Immediate treatment¹
Salbutamol 5mg (or terbutaline 10mg) nebulized with O₂ Hydrocortisone 100mg IV or prednisolone 40–50mg PO or both if very ill Start O₂ if saturations <92% (also check ABG), aim sats 94–98%
If life-threatening features present:
- Inform ICU and seniors
- Give salbutamol nebulizers every 15min, or 10mg continuously per hour. Monitor ECG; watch for arrhythmias
- Add in ipratropium 0.5mg to nebulizers
- Give single dose of magnesium sulfate (MgSO₄) 1.2–2g IV over 20min
in life-threatening differences clampola traume Dunt
If not improving:
Refer to ICU for consideration of ventilatory support and intensification of medical therapy, eg aminophylline, IV salbutamol if any of the following signs are present:
- Deteriorating PEF
- Persistent/worsening hypoxia
- Hypercapnia
- ABG showing low pH or high H’
- Exhaustion, feeble respiration
- Drowsiness, confusion, altered conscious level
- Respiratory arrest
If improving within 15–30 minutes:
- Nebulized salbutamol every 4 hours
- Prednisolone 40–50mg PO or 5–7 days
- Monitor peak flow and O₂ sats, aim 94–98% with supplemental if needed
3/4/2024
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of life-threatening asthma?
A Pulse > 110 bpm B RR < 25 / min C Pulse < 110 bpm D Speech normal E RR > 25/min F Oxygen sats < 92%
Case scenario
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of moderate asthma?
A Oxygen sats < 92% B Pulse > 110 bpm C RR > 25/min D PEFR 33 - 50% best or predicted E Speech normal F Can’t complete sentences
Case scenario
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of moderate asthma?
A RR > 25/min
B Can’t complete sentences
C Pulse > 110 bpm
D PEFR 50-75% best or predicted
E Exhaustion, confusion or coma
F PEFR 33 - 50% best or predicted
Case scenario
SAMPLE FOOTER TEXT 15
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of severe asthma?
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is not a feature of severe asthma?
A
- RR < 25 / min B
- PEFR 33 - 50% best or predicted C
- Oxygen sats < 92% D
- RR > 25/min E
- Can’t complete sentences
Case scenario
SAMPLE FOOTER TEXT
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of severe asthma?
When assessing a patient with acute asthma they are classified as being moderate, severe or life-threatening. Which one of the following is a feature of life-threatening asthma?
A PEFR 33 - 50% best or predicted B RR < 25 / min C Bradycardia, dysrhythmia or hypotension D Pulse < 110 bpm E Pulse > 110 bpm F Can’t complete sentences
Case scenario
3/4/2024
Management
Admission
- All patients with life-threatening
- Severe acute asthma admitted if they fail to respond to initial treatment.
- other admission criteria include
- ☑ a previous near-fatal asthma attack
- ☑ pregnancy
- ☑ an attack despite already using oral corticosteroid
- ☑ Presentation at night the incidence at night high
18
3/4/2024
Management
- Oxygen
- if patients are hypoxaemic, start supplemental oxygen therapy
- if patients are acutely unwell; started on 15 L of supplemental via a non-rebreathe mask, titrated down to a flow rate where they are able to maintain a 94-98%.
3/4/2024
Management

- Bronchodilation with short-acting beta₂-agonists (SABA)
- High-dose inhaled SABA e.g. salbutamol, terbutaline.
- If no feature of life-threatening or near-fatal asthma; standard pressurised metered-dose inhaler (pMDI) or by an oxygen-driven nebulizer.
- Life-threatening exacerbation of asthma; nebulised SABA is recommended
20
3/4/2024
Management
Corticosteroid
-
All patients: given 40-50mg of prednisolone orally (PO) daily, continued for at least 5 days or until recovery. If on inhaled steroid: continue
-
Ipratropium bromide: severe or life-threatening asthma, or if not response to beta₂-agonist and corticosteroid ttt, nebulised ipratropium bromide
-
IV magnesium sulphate; severe/life-threatening asthma
-
IV aminophylline; consultation; fail to respond require senior critical care support and should be treated in an appropriate ITU/HDU setting.
Treatment options include:
- intubation and ventilation
- extracorporeal membrane oxygenation (ECMO)

3/4/2024
Typical results in asthma
- FEV1 - significantly reduced
- FVC - normal
- FEV1% (FEV1/FVC) < 70%
22
3/4/2024
An asthmatic patient presented with this ABG finding; Comment
| pH | 7.37 | (7.35-7.45) |
|---|---|---|
| pO2 | 10.1 kPa | (>9 kPa) |
| pCO2 | 4.9 kPa | (4.7-6.0 kPa) normal |
| Base excess | 1.1 | (-2 to 2) |
| Lactate | 1.9 mmol/L | (<2 mmol/L) |
life threatening attack
SAMPLE FOOTER TEXT
3/4/2024
Criteria for discharge
☐ Stable on their discharge medication (i.e. no nebulisers or oxygen) for 12–24 hours
- Inhaler technique checked and recorded. ☑ PEF >75% of best or predicted

3/4/2024
| Drug | Mechanism of action | Notes |
|---|---|---|
| Salbutamol | Beta receptor agonist | • Short-acting inhaled bronchodilator. Relaxes bronchial smooth muscle through effects on beta 2 receptors |
| • Used in asthma and chronic obstructive pulmonary disease (COPD). | ||
| • Salmeterol has similar effects but is long-acting | ||
| Corticosteroids | Anti-inflammatory | • Inhaled corticosteroids are used as maintenance therapy |
| • Oral or intravenous corticosteroids are used following an acute exacerbation of asthma or COPD | ||
| Ipratropium | Blocks the muscarinic acetylcholine receptors | • Short-acting inhaled bronchodilator. Relaxes bronchial smooth muscle |
| • Used primarily in COPD | ||
| • Tiotropium has similar effects but is long-acting | ||
| Methylxanthines (e.g. theophylline) | Non-specific inhibitor of phosphodiesterase resulting in an increase in cAMP | • Given orally or intravenously |
| • Has a narrow therapeutic index | ||
| Monteleukast, zafirlukast | Blocks leukotriene receptors | • Usually taken orally |
| • Useful in aspirin-induced asthma |
3/4/2024
Quick facts
-
Which beta-2 adrenergic agonist is used to treat acute asthma?
-
Albuterol
-
Salbutamol
3/4/2024
Quick facts
- What is the MOA of Zileuton ?
Inhibit 5 lipoxygenase and leukotrin
SAMPLE FOOTER TEXT 27
3/4/2024
Quick facts
The muscarinic agonist …methacaline…is used in bronchial provocation challenges to diagnose asthma
28
3/4/2024
Quick facts
methacdin The muscarinic agonist is used in bronchial provocation challenges to diagnose asthma
3/4/2024
Quick facts
What is the MOA of Ipratropium?
Competitive inhibition of ACh Muscarinic receptors
30
3/4/2024
Quick facts
… is indicated for the treatment of asthma by preventing IgE from binding mast cells
31
3/4/2024
Quick facts
Omalizumab is indicated for the treatment of asthma by preventing IgE from binding mast cells
3/4/2024
Quick facts
Tremor and cardiac arrhythmias are side effects of long-acting beta2-adrenergic agonists such as formoterol or salmeterol
33
3/4/2024
| Asthma – suspected | Adult asthma – diagnosed | |||
|---|---|---|---|---|
| Diagnosis and assessment | Evaluation: • assess symptoms, measure lung function, check inhaler technique and adherence | |||
| • adjust dose • update self-management plan • move up and down as appropriate | ||||
| Consider monitored initiation of treatment with low-dose ICS | Infrequent, short-lived wheeze | Move down to find and maintain lowest controlling therapy | Move up to improve control as needed | Specialist therapies |
| Initial add-on therapy | ||||
| Add inhaled LABA to low-dose ICS (fixed dose or MART) | Additional controller therapies | |||
| Consider: | ||||
| Increasing ICS to medium dose | ||||
| or | ||||
| Adding LTRA | ||||
| If no response to LABA, consider stopping LABA | Refer patient for specialist care | |||
| Short acting β₂ agonists as required (unless using MART) – consider moving up if using three doses a week or more |
3/4/2024
Further explanation
Maintenance and reliever therapy (MART)
- a form of combined ICS and LABA treatment in which a single inhaler, containing both ICS and a fast-acting LABA, is used for both daily maintenance therapy and the relief of symptoms as required
- MART is only available for ICS and LABA combinations in which the LABA has a fast-acting component (e.g, formoterol)
Notes:
- Don’t changing treatment in patients who have well-controlled asthma simply to adhere to the latest guidance.
Inhaled corticosteroid doses
- ⇐ 400 micrograms budesonide or equivalent = low dose
- 400 micrograms - 800 micrograms budesonide or equivalent = moderate dose
- > 800 micrograms budesonide or equivalent = high dose.
SAMPLE FOOTER TEXT
Asthma: management in adults
| Step | Notes |
|---|---|
| 1 Newly-diagnosed asthma | Short-acting beta agonist (SABA) |
| 2 Not controlled on previous step OR | |
| Newly-diagnosed A with symptoms |
= 3 / week or night-time waking | SABA + low-dose inhaled corticosteroid (ICS) | | 3 | SABA + low-dose ICS + leukotriene receptor antagonist (LTRA) ext with Kan | | 4 | SABA + low-dose ICS + long-acting beta agonist (LABA) Continue LTRA depending on patient’s response to LTRA | | 5 | SABA +/- LTRA we can stop it & no response Switch ICS/LABA for a maintenance and reliever therapy (MART), that includes a low-dose ICS ext with sABA + ICS | | 6 | SABA +/- LTRA + medium-dose ICS MART OR consider changing back to a fixed-dose of a moderate-dose ICS and a separate LABA 400 - 800 | | 7 | SABA +/- LTRA + one of the following options: • increase ICS to high-dose (only as part of a fixed-dose regime, not as a MART) 800 • a trial of an additional drug (for example, a long-acting muscarinic receptor antagonist or theophylline) • seeking Expert advice |
What is the most appropriate next step in the following scenario: newly diagnosed adult with asthma (symptoms < 3 times/weeks)?
A Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers
B Add a low-dose ICS
C Stop LABA + increase ICS to medium-dose
D Add a SABA
E Switch ICS/LABA for a MART regime with a low-dose ICS
F Add a LABA
Case scenario
SAMPLE FOOTER TEXT 37
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA + low-dose ICS?
A Add a leukotriene receptor antagonist B Add a LABA C Stop LABA + increase ICS to medium-dose D Trial of either high-dose ICS as part of fixed-dose regime, additional drug (e.g. LAMA or theophylline) or referral E Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers F Add a SABA
Case scenario
SAMPLE FOOTER TEXT 38
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA + low-dose ICS +/- leukotriene receptor antagonist + LABA?
SAMPLE FOOTER TEXT 39
| A | Add daily oral prednisolone |
|---|---|
| B | Add a LABA |
| C | Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers |
| D | Stop LABA + increase ICS to medium-dose |
| E | Switch ICS/LABA for a MART regime with a low-dose ICS |
| F | Trial of either high-dose ICS as part of fixed-dose regime, additional drug (e.g. LAMA or theophylline) or referral |
Case scenario
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA +/- leukotriene receptor antagonist + MART regime with a low-dose ICS?
SAMPLE FOOTER TEXT 40
| A | Trial of either high-dose ICS as part of fixed-dose regime, additional drug (e.g. LAMA or theophylline) or referral |
|---|---|
| B | Add a low-dose ICS |
| C | Add a LABA |
| D | Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers |
| E | Stop LABA + increase ICS to medium-dose |
| F | Add a leukotriene receptor antagonist |
Case scenario
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA + low-dose ICS + leukotriene receptor antagonist?
A Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers
B Add a LABA
C Stop LABA + increase ICS to medium-dose
D Trial of either high-dose ICS as part of fixed-dose regime, additional drug (e.g. LAMA or theophylline) or referral
E Add daily oral prednisolone
F Add a low-dose ICS
SAMPLE FOOTER TEXT 41
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA?
A Add daily oral prednisolone B Add a LABA C Add a SABA D Add a low-dose ICS E Add a leukotriene receptor antagonist F Switch ICS/LABA for a MART regime with a low-dose ICS
Case scenario
SAMPLE FOOTER TEXT 42
What is the most appropriate next step in the following scenario: adult with asthma not controlled by a SABA +/- leukotriene receptor antagonist + MART regime with a moderate-dose ICS?
SAMPLE FOOTER TEXT 43
A Add daily oral prednisolone
B Stop LABA + increase ICS to medium-dose
C Add a LABA
D Switch ICS/LABA for a MART regime with a low-dose ICS
E Trial of either high-dose ICS as part of fixed-dose regime, additional drug (e.g. LAMA or theophylline) or referral
F Switch to either a MART regime with a moderate-dose ICS or to separate moderate-dose ICS and LABA inhalers
A 50-year-old man with late-onset asthma presents with malaise and weight loss. He also complains of recurrent bouts of sinusitis. Bloods show a marked eosinophilia is a stereotypical history of:
signs of upper Reip track
A Churg-Strauss syndrome
B Buerger’s disease
C Polyarteritis nodosa
D Takayasu’s arteritis
E Granulomatosis with polyangiitis
F Temporal arteritis
Case scenario
SAMPLE FOOTER TEXT 44
3/4/2024
An 18-year-old man is admitted to the emergency department with an episode of acute asthma. He is unable to complete sentences, tachycardic (118 beats per minute) and tachypnoeic (respiratory rate 30). He has received salbutamol, ipratropium bromide nebulisers and intravenous hydrocortisone through a large bore cannula in the right antecubital fossa. Despite another salbutamol nebuliser, there is no improvement in his condition. What medication would be most appropriate to add?
A. Beclamethasone B. Magnesium sulphate C. Amoxicillin D. Nifedipine E. Adrenaline
3/4/2024

Remember asthma is not only asthma, always consider other possible diagnosis
SAMPLE FOOTER TEXT 46
3/4/2024
Occupational Asthma
SAMPLE FOOTER TEXT 47
3/4/2024
Asthma: occupational
Exposure to the following chemicals is associated with occupational asthma:
- isocyanates - the most common cause
- Spray painting and foam moulding using adhesives
- platinum salts
- soldering flux resin
- glutaraldehyde
- flour
- epoxy resins
- proteolytic enzymes
Investigations
Serial measurements of peak expiratory flow are recommended at work and away from work. home
Referral ; respiratory specialist for suspected patients

Patients concerns: chemicals at work are worsening their asthma Doctor; history that symptoms seem better at weekends / when away from work.
SAMPLE FOOTER TEXT 49
Which one of the following is the best investigation for occupational asthma?
A Spirometry
B Serum IgE
C Schirmer’s test
D Serial peak flows at home and at work
E Overnight dexamethasone suppression test
F Serum tryptase
Case scenario
3/4/2024
Case scenario
- A 45-year-old man presents with a three-month history of wheezing and dyspnoea whilst at work. His symptoms improve significantly when at home and at weekends.
- What is the likely causative agent?
A. Simple coal worker’s lung B. Silica C. Cotton dust D. Asbestos E. Isocyanates
3/4/2024
Asthma & Pregnancy
- Reassure
- Guidelines: Good control of asthma during pregnancy.
- Drugs safe during pregnancy and breastfeeding’.
- ‘inhaled drugs, beclometasone and salmeterol
- Theophylline
- prednisolone

SAMPLE FOOTER TEXT 51
3/4/2024
A 28-year-old woman is attending her annual asthma review. She is currently prescribed a salbutamol inhaler 100μg and budesonide 400μg. Her asthma is well controlled and she hasn’t needed to use her ‘blue inhaler’ over the past year. She is currently trying for a baby and is concerned about taking her asthma medications during pregnancy.
What is the most appropriate change to her medications?
A. Add leukotriene receptor antagonist B. Reduce budesonide dose C. Reduce salbutamol dose D. Stop budesonide E. Stop salbutamol
In the step-down : aim for a reduction of 25-50% in the dose of inhaled corticosteroids
Thank You!

Kumar: 949-954