(ALS or Lou Gehrig’s disease)
Motor
Neurone
Disease
Associate Professor
Dr Nada Abdelrahman
Lina Sethian
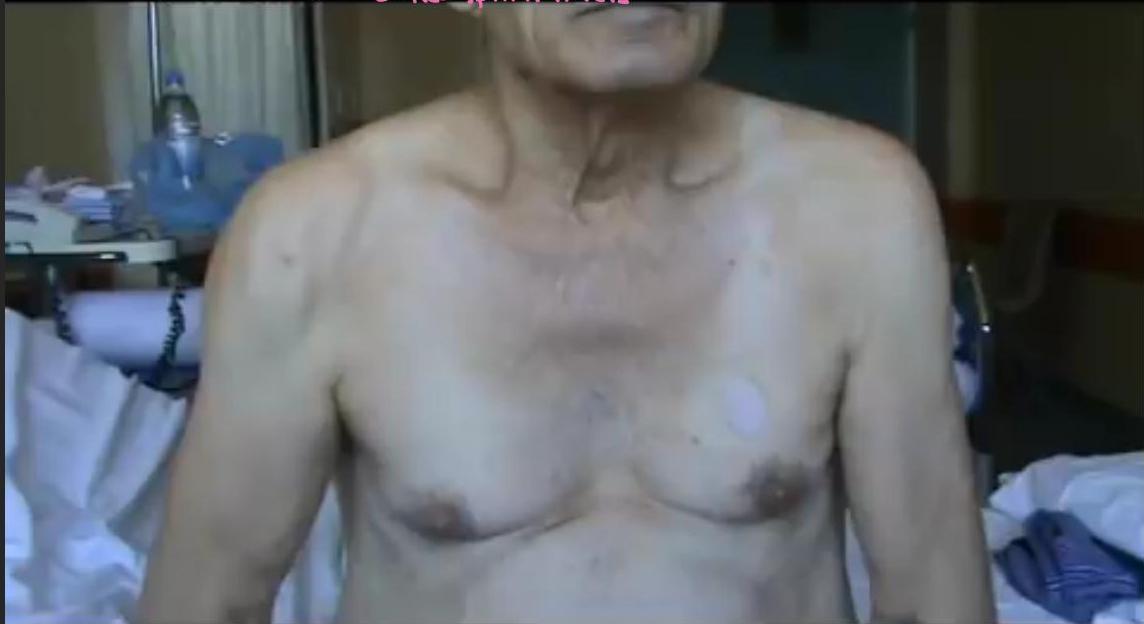
A man with progressive weakness of upper and lower limbs
Faciculation and upper limb weakness in a young male → no diagnosis is ALS

HENRY LOUIS GEHRIG
JUNE 19TH 1903 — JUNE 2ND 1941
A MAN, A GENTLEMAN AND A GREAT BALL PLAYER WHOSE AMAZING RECORD OF 2130 CONSECUTIVE GAMES SHOULD STAND FOR ALL TIME.
THIS MEMORIAL IS A TRIBUTE FROM THE YANKEE PLAYERS TO THEIR BELOVED CAPTAIN AND TEAM MATE
This Photo JULY THE FOURTH BY-SA 1941
Learning Objectives
- By the end of this lecture, the student should be able
- Define and identify possible causes of MND
- Explain the pathology and epidemiology of MND
- Identify and describe types of MND
- Diagnose a case of MND
- Manage a case of MND
Definition
- It is a degenerative disease of a gradual onset and progressive course, affecting the motor system only in which selective loss of function of upper motor neurons, lower motor neurons, or both results in impairment of the nervous system’s control of voluntary movement.
GR. 4546 LECTURES 08 THE DISEASES OF THE NERVOUS SYSTEM. DELIVERED AT LA SALPETRIÈRE J. M. CHARCOT, (296-1855) (PUBLISHED IN THE PATIENT OF MORNING OF FUND, PRINCIPAL MAIL CERTIFICATION, SUBJECT OF THE CHARGES OF MORNING, OR THE MORNING AGENCY OF FUND, OR THE CLINICAL AGENCY OF EMPLOYMENT, OR THE MORNING AGENCY OF NERVOUS SYSTEMS OF NERVOUS, PRESIDENT OF THE ASSOCIATED BRANCH, AND SECTOR-DEMOCRAT OF THE BIOLOGICAL SOCIETY OF PARIS, INC.) SECOND SERIES. TRANSLATED AND EDITED BY GEORGE SIGERSON, M.D., C.R.M., (PUBLISHED IN THE RIMS AND GRAPHIC VERSION OF DEMOCRATS OF ORALS, 1924, 20 THE SURVEYS OF MORNING, I.E.I., SUBJECT OF THE RISKS (RISK ANALYSIS), REVIEW OF THE GENERAL EXAMINATION OF ANIMAL, SUBJECT OF THE ACHIEVING MOTOR OF NERVOUS); (PUBLISHED IN THE ACHIEVING AND ADVERTISING, SUBJECT OF THE ACHIEVING AND ADVERTISING, SUBJECT OF THE ACHIEVING AND ADVERTISING, SUBJECT OF THE ACHIEVING AND ADVERTISING).
Basic Facts
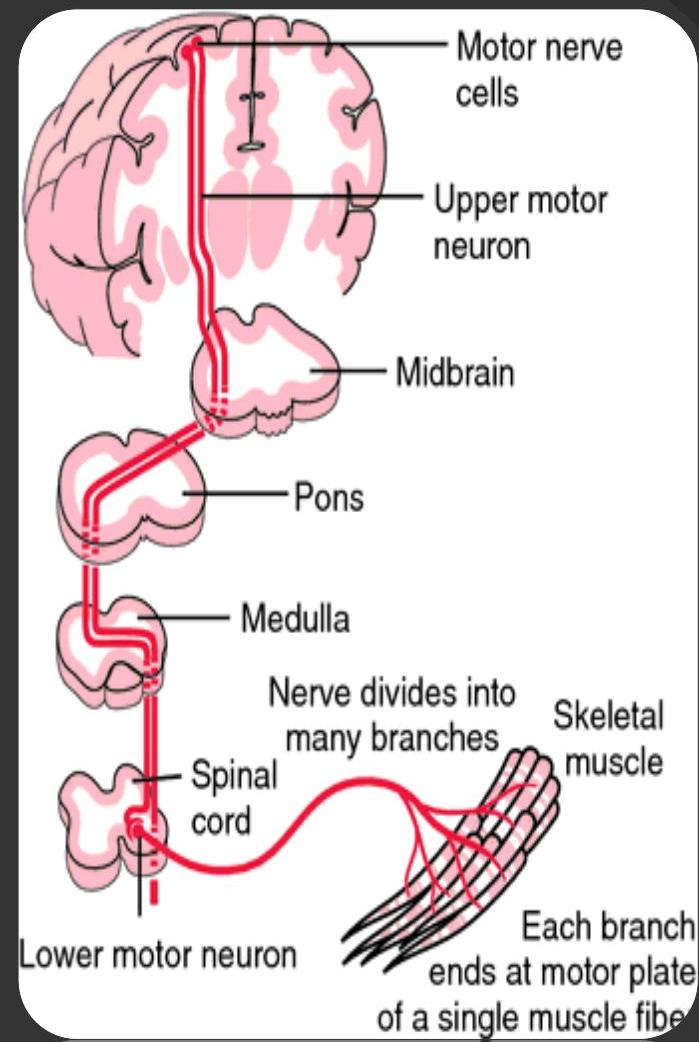
What is the motor system?
Epidemiology
Every person develops disease in a different Symptoms : depends on area of NS system 90% - 95% : sporadic form. 5-10% Familial. Adult Illness – C > 50 male Average survival 2-5 yrs from first symptoms. From diagnosis 14 months average. No cure but symptomatic ttt that may improve quality or prolong life. Onset and progression is variable.
Aetiology and Risk factors
Idiopathic Familial tendency Mechanical/electrical trauma Military service, Exercises Agricultural chemicals and heavy metals Research : genetic SOD 1 (Familial Chromosome 21: Ubiquitin protein gene
Pathology
- Loss of cortical pyramidal motor neurons and gliosis
Hyper-reflexia Babinski +ve Sparticity
- Corticospinal tracts with variable patterns of degeneration
Paralysis Paresis “weakness” hyper-tonia
- Sclerosis and pallor of the corticospinal tract
- Precentral gyrus atrophy

Types of Motor Neurone Disease
- Amyotrophic lateral sclerosis (ALS) mixed
- Progressive bulbar palsy up to lower
- Progressive muscular atrophy pure
- Primary lateral sclerosis pure upper
Overlap is common
Classified:
- In terms of the motor neurones affected
- Symptoms
Bulbar—refers to face/speech/swallowing
Amyotrophic Lateral Sclerosis (ALS)
Amyotrophic Lateral Sclerosis → affect Lateral Cortico-spinal tracts
in ALS Pit has mixture of symptoms weakness, Fasciculation but high reflexes mixed sign → ALS
Involves UMNs and LMNs: combined signs and symptoms of lower and upper motor neuron lesions
→ 2 cells or Anterior horn cells
- 65% of cases Commonest type
- Muscle weakness – often
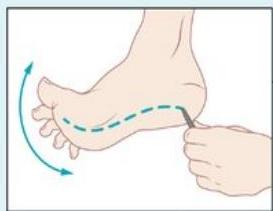
- Develops in hands and feet first, spasticity. (50% of cases are in hand)
- Hyperactive reflexes: a brisk reflex in a wasted muscle is a classic sign, extensor plantar responses and spasticity
Progressive Muscular Atrophy (PMA)
ALS-amyotrophic lateral sclerosis
7.5%-10% of cases
- Predominantly LMNs: affected (may start in small muscles of hand)
- Muscle wasting, Atrophy
- Weakness
- Fasciculation
- negative Papnecki sign
- (in time develop UMN involvement and may have some speech problems)
inspection: less muscle wasting
Tone: Hypertonia, Hyperreflexia, Clonias
Positive Papnecki sign
absent abdominal reflex
Progressive Bulbar Palsy (PBP)

20% of cases
- Involves UMNs and LMNs
- Dysarthria
- Dysphagia
- Emotional lability
- Progressive weakness in upper limbs, neck and shoulders.
- The a bag of warm *
A fasciculating tongue with slow movements is the classic finding in a mixed bulbar palsy.
Primary Lateral Sclerosis (PLS)
2% of cases
- Rare
- UMNs only
- Muscle weakness
- Pit is stiff more than anything.
- Stiffness
- Dysarthria
- Tetraparesis and pseudobulbar palsy.
- Does not shorten the survival life span
Pseudobulbar palsy: UMN palsy of corticobulbar tracts of cranial nerves V, VII, IX, X, XI, and XII..
Upper motor neuron dysfunction
Lower motor neuron dysfunction
Pseudobulbar palsy
Mood-incongruent laughing/crying Dysphagia, dysarthria
Spasticity, stiffness
Hyperreflexia
 Pyramidal signs (e.g., Babinski sign)
Pyramidal signs (e.g., Babinski sign)
Bulbar palsy
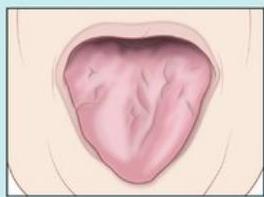 Tongue atrophy
Dysphagia, dysarthria
Tongue atrophy
Dysphagia, dysarthria
Flaccid weakness (initially asymmetrical), muscle atrophy
Respiratory insufficiency
Fasciculations, cramps
Pathophysiology of ALS: degeneration of UMN and LMN
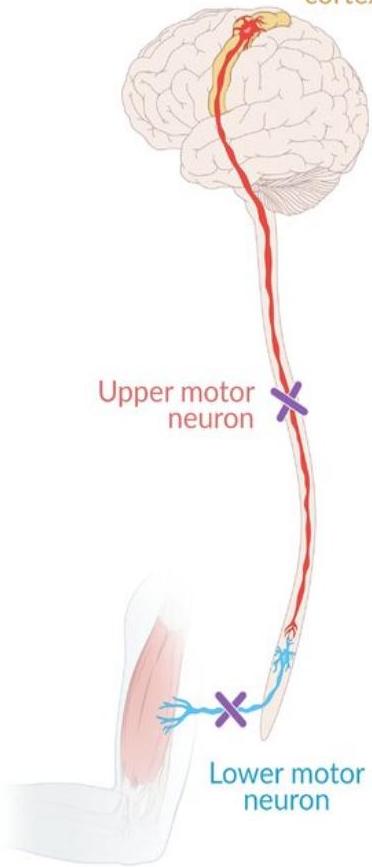 Primary motor cortex
Primary motor cortex
Site of Onset
- Limbs (usually distal)
- Bulbar
- Respiratory Failure
Early Symptoms
Case: Surgeon can’t handle his scalper after months he shot to have weakness in his lower limb his 4 limbs become weak and his mental state is good.
| Stumbling | Foot drop | loss of dexterity | Weakened grip | Cramps |
|---|---|---|---|---|
| Change of voice quality | Slurred speech | Early swallowing difficulties | Muscle wasting | Fatigue |
Course of Disease
- Onset and progression variable
- Is always progressive with no remissions
- Usually affects both the upper and lower motor neurons
- 90% develop some bulbar symptoms
- Death often through respiratory failure
Diagnosis Clinical
On average, it takes 14 months from first

Symptoms to diagnose MND
First signs and symptoms often subtle and

non-specific, similar to other diseases
Person often not referred to a neurologist directly
No definitive diagnostic test
How is MND diagnosed
- Interpretation of clinical symptoms and signs
- Investigations to exclude other causes
- MRI
- Lumbar puncture
- typical Calene … Patching
Tests
Raised CPK – in MND but not diagnostic
- EMG: Each limbs-abnormal in MND as the electrical activity of the muscles is changed
- Nerve conduction tests: normal
MRI: Eliminates other diseases
- Lumbar puncture or muscle biopsy
Effects of MND
| Progressive muscle weakness and wasting | Loss of weight | Fasciculation, cramp and spasticity | Dysarthria-slurred effortful speech |
|---|---|---|---|
| Dysphagia - poor swallow due to weakness and paralysis of bulbar muscles | Saliva and Mucus Problems | Respiratory muscle weakness | Emotional liability |
| UMWL, Bulbar |
Cognitive changes
Clues to respiratory muscle involvement in MND
- Breathlessness
- on minimal exertion
- on lying flat
- ☐ Poor sleep obstructive sleep apnea
- ☐ Excessive daytime sleepiness
- ☐ Headaches on awakening
- ☐ Excessive Nocturnal sweating
Differentia / diagnosis
First you have to exclude
- Cervical mylopathy
- upper limb wasting
- Lower limb spastic
Multifocal motor neuropathy (MMN): Slowly progressing asymmetrical weakness, esp. muscles of distal extremities, No muscle atrophy
Myasthenia gravis
Lambert-Eaton myasthenic syndrome
Cervical spondylosis: Sensory symptoms.
Thyrotoxicosis → Here’s Fasciculation
Poliomyelitis: asymmetric flaccid paralysis
different age group

Psychosocial Impact
- Multiple losses: physical loss, loss of control, and independence. Self-image and confidence.
- Financial.
- Home environment.
- Communication difficulties.
- Increasing isolation and dependence on carers.
- Anxiety, Fear and Anger.
- Knowledge of own impending deterioration and death.
Cognitive changes
MND has been traditionally viewed at a disease affecting the motor system
Compromise of cognitive abilities
Recent research shows that 25% Show some cognitive changes
- 3-5% will have Fronto-temporal dementia
What isn’t affected by MND
- Senses: touch, taste, sight, smell and hearing
- Bowel and bladder function
- Sexual function and sexuality
- Eye Muscles
- Heart muscles
- Cerebellar signs
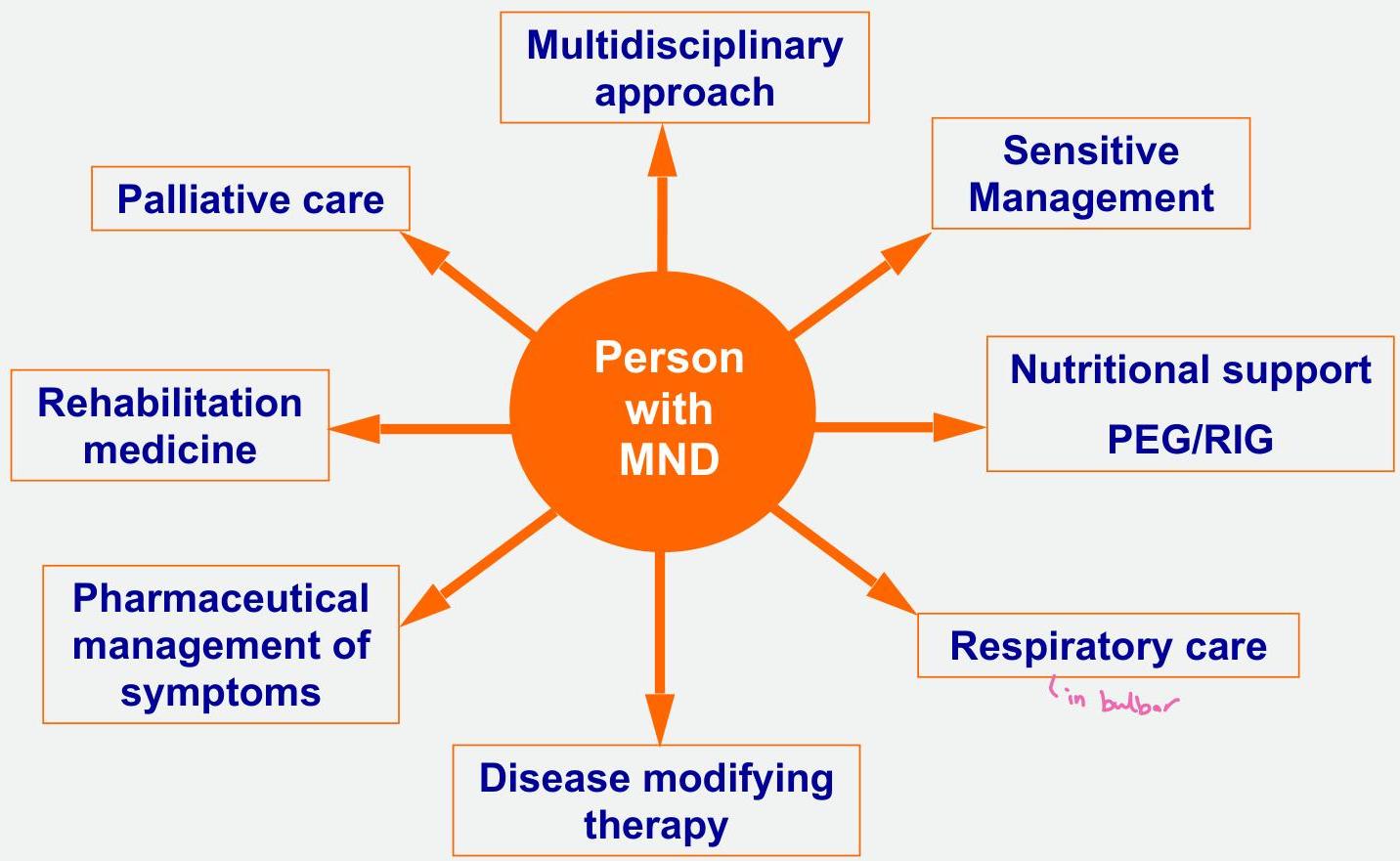
Aims of Management
- Control of symptoms.
- Promote independence
- Support at home as much as possible.
- Plan appropriate interventions.
Treatments/interventions in MND
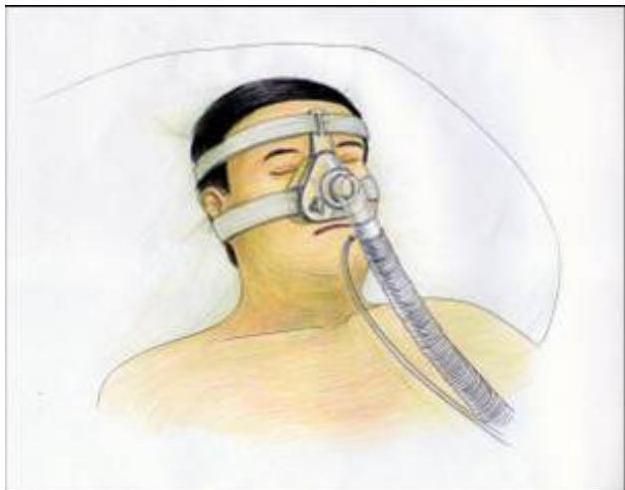
Life Prolonging Intervention
- Riluzole (glutamate antagonist) drug to have beneficial effect on survival: 3-4 months.
- Edaravone (free radical scavenger): slow functional decline.
- Non-invasive ventilatory support and feeding via a gastrostomy prolong survival.
- Median survival extended 205 days (Miller et all 2009).
MEDICATIO N
Medications for symptoms
- Muscle cramps: (Carbamazepine & Phenytoin)
- Muscle Stiffness (Muscle relaxants): Botox and intrathecal baclofen — muscle relaxant
- Drooling: (Hyosine and Atropin)
Pain → analgesic | Gabapentin

Prognosis
- Most patients die 3–5 years
- 5-year-survival: 30%
- 10-year-survival: 10–20%
- Early bulbar and/or respiratory symptoms are associated with a worse prognosis
End of Life Decisions
| Advanced Care Planning. |
|---|
| Advanced decision to refuse treatment (ADART). |
| Advanced Statement of wishes and preferences. |
| Preferred Priorities of Care (PPC). |
| Withdrawal of treatments. |
| Tissue donations. |
Case scenario
A. Demyelination of the dorsal columns, spinocerebellar tracts, and lateral corticospinal tracts Fredrix olfatia B. Lower motor neuron lesion due to destruction on anterior horns in pilians C. Death of both upper and lower motor neurons in the motor cortex, the brain stem, and the spinal cord MND D. Damage to anterior white commissure E. Degeneration of dorsal roots and dorsal columns
- A 9-year-old boy presented with increasing fevers, fatigability and urinary incontinence for the past 2 days. His temperature is 39.2°C, pulse is 120/min, and blood pressure is 120/82mmHg.
- Physical examination shows neck stiffness, and weakness in his lower extremities, more pronounced on the right than the left. The tone and reflexes in both legs are reduced. The sensory examination is normal. Which of the following is the most likely cause of the patient’s symptoms?
Case scenario
A. Baclofen B. Sildenafil C. Donepezil D. Acetaminophen E. Propanolol
- A 29-year-old lady presented with intermittent muscle cramps and weakness of her left leg for 3 months. She says these episodes usually last a week, and then completely resolve.
- Other symptoms she has intermittently experienced are blurred vision, difficulty in maintaining balance, as well as urinary urgency and incontinence. Visual examination is normal.
- There is decreased muscular power in her left leg, and an up-going left-sided plantar reflex. Which of the following medications would most likely reduce this patient’s muscle cramps?
Home messages
Kumar and Clark: 885
USEFUL CLUES
- Progressive
- Incurable
- rare
- Group of related diseases
- Motor neurones are affected
- Upper and lower limb weakness
- Speech and swallowing difficulties
- Breathing difficulties