SEXUALLY TRANSMITTED DISEASES (STD)
PROFESSOR SALIH BIN SALIH CHAIRMAN, DEPARTMENT OF MEDICINE KING ABDULAZIZ MEDICAL CITY PROFESSOR OF MEDICINE, COLLEGE OF MEDICINE KING SAUD BIN ABDULAZIZ UNIVERSITY FOR HEALTH SCIENCE (KSAU-HS)
Lina Serhan
STD 2
- STD are most common cause of illness in the world
- Those who acquire STD are usually young people, Homosexual and bisexual men.
- Increased travel within and between countries recreational drug use, alcohol, frequent use of partners are also the cause.
STD 3
Three most common complaints are
- Vaginal discharge
- Urethral discharge
- Genital ulceration
STD
majorities in infectious
4
| Table 4.45 | Causes of vaginal discharge |
|---|---|
| Infective | Non-infective |
| Candida albicans | · Cervical polyps |
| Trichomonas vaginalis | · Neoplasms |
| Bacterial vaginosis | · Retained products (e.g. tampons) |
| Neisseria gonorrhoeae | · Chemical irritation |
| Chlamydia trachomatis | |
| Herpes simplex virus | |
| Table 4.46 | Causes of urethral discharge |
| --- | --- |
| Infective | Non-infective |
| Neisseria gonorrhoeae | Physical or chemical trauma |
| Chlamydia trachomatis | Urethral stricture |
| Mycoplasma genitilium | Non-specific (aetiology unknown) |
| Ureaplasma urealyticum | |
| Trichomonas vaginalis | |
| Herpes simplex virus | |
| Human papillomavirus (meatal warts) | |
| Urinary tract infection (rare) | |
| Treponema pallidum (meatal chancre) | |
| Table 4.47 | Causes of genital ulceration |
| --- | --- |
| Infective | Non-infective |
| Syphilis: | · Behçet’s syndrome |
| Primary chancre | · Toxic epidermal necrolysis |
| Secondary mucous patches | · Stevens-Johnson syndrome |
| Tertiary gumma | · Carcinoma |
| Chancroid | · Trauma |
| Lymphogranuloma venereum | |
| Donovanosis | |
| Herpes simplex: | |
| Primary | |
| Recurrent | |
| Herpes zoster |
STD 5
Detailed history is taken and includes
- Number and types of sexual contacts
- Use of condoms or other form of contraception
- Travel abroad
STD 6
- Examination
- General Examination
- Look at mouth, throat, skin, lymph nodes
- Signs of HIV infection- Candidiasis, Herpes simplex, CMV retinitis, Kaposis sarcoma, TB
- Exam of Genitala, perianal region, Inguinal region for lymphadenopathy.
and they were healthy before
STD 7
Investigations
- Asymptomatic Patient STI screening
- HIV antibody test (optional), if declined by patient, reason should be documented
- Hepatitis B, Hepatitis C screening
- Urine test
- Urethral swab for gonococcus
- Throat swab
- Rectal swab
- WOMEN – Vulvo-vaginal swab
- Pregnancy test if indicated
STD
8
Investigations for Symptomatic patients:
Men
- urethral swab for microscopic examination eg. Gonococal Infection, Chlamydia
- Rectal swab, oropharyngeal swab
- HIV Antibody
- Hepatitis B & C Serology if indicated
Women
- Cervical swab for Gonococal infection, Chlamydia (usually uping not affected due to a.c.d.i.c. medial)
- Vaginal swab – microscopy, culture for candidia, trichomoniasis and Bacteri,al vaginosis
- Rectal and Oropharyngeal swab
9
LIST OF STD
Main Sexually transmitted Infections:
-
Gonorrhea
-
Syphilis
-
Chlamydia
-
Lymphogranuloma Venereum (LGV)
-
Genital Herpes
-
Genital Warts -Human Papillomavirus
-
HIV & AIDS
-
Hepatitis B
-
Hepatitis C
-
Trichomoniasis
most common
GONORRHOEA (GC)
10
- Neisseria gonorrhoea (Gonococci, GC) is gram negative intracellular diplococcus which infects epithelium of urogenital tract, rectum, pharynx and conjunctiva
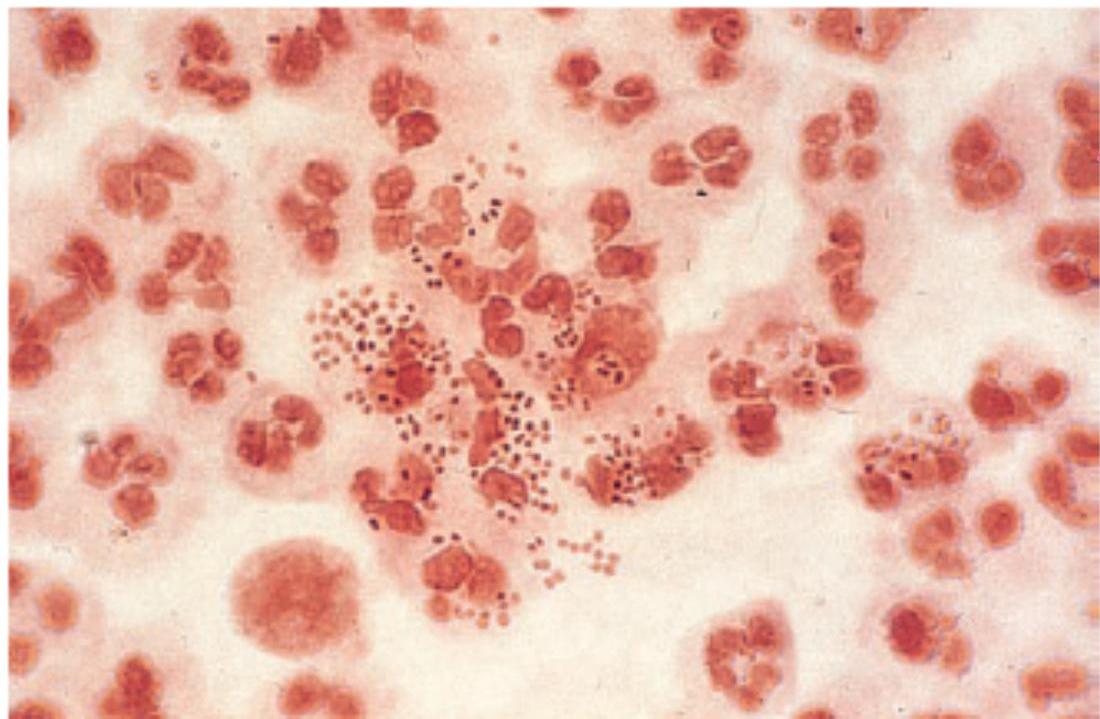 Fig. 4.39 Neisseria gonorrhoeae – Gram-negative intracellular diplococci. Courtesy of Dr B Goh.
Fig. 4.39 Neisseria gonorrhoeae – Gram-negative intracellular diplococci. Courtesy of Dr B Goh.
red Stain (gram Neg.
11
GONORRHOEA (GC)
Clinical Features:
-
Upto 50% of women and 10% of men are asymptomatic. male most of them symptomatic
-
Incubation period is 2-14 days with symptoms occurring between 2-5 days.
-
In men most common symptom is anterior urethritis causing dysuria and urethral discharge.
-
In women symptoms include vaginal discharge, dysuria, intermenstural bleeding, pelvic pain due to ascending infection.
12
GONORRHOEA (GC)
Diagnosis:
- N. Gonorrhoeae – culture from infected area
- Microscopy of gram stain of secretion may demonstrate intracellular gram negative diplococci (looking red color) allowing rapid diagnosis
- Nuclear acid amplification test (NAATs) on urine specimen are highly sensitive but may give false positive results in all screening tests
- Blood culture and synovial fluid investigation in disseminated GC
- should be there
- systematic involvement
- septecemia
13
GONORRHOEA (GC)
Treatment:
- Single dose ceftriaxone injection IM 500 mg
- (use to prolong penicillin action)
- Oral Amoxicillin 3 gm with probenecid 1 gm
- Ciprofloxacillin 500 mg single dose in uncomplicated gonorrhoea.
14
Syphilis
- Syphilis is chronic systemic disease, it may be acquired or congenital
- Causative organism – treponema pallidium (TP)
- It is motile spirochaete (bacterial infection) which is acquired by sexual contact or can be transmitted transplacentaly
- We will discuss acquired and congenital syphilis
not cultured we see it in microscope
Syphilis
15
1-Acquired Syphilis:
- Early stages
- Primary
- Secondary
- Late stage – tertiary
- Primary Acquired Syphilis:
After exposure to pathogen a papule develops at the site of innoculation. Incubation period 21 days (10-91 days) This ulcerates to become painless firm chancre.
There is painless regional lymphadenopathy
Healing occurs in 2-3 weeks
Syphilis
16
generalized and
systematic involvement
Secondary Acquired Syphilis:
- Incubation period is 4-10 weeks, in the secondary stage there is fever,
sore throat, malaise, arthralgia.
- Organs may be affected leading to hepatitis, nephritis, arthritis,
meningitis.
-
Signs of secondary syphilis include
-
Generalised lymphadenopathy – 50%
-
Generalised skin rash – involving palms and soles but not the face
Rash is maculopapular, non-itchy
but all symptomatic “not itchy”
-
Mucosal ulcers found in mouth, on genitalia described as snail tract ulcers
-
Condylomata lata – warty plaque like lesion found in perianal region
in brain
Syphilis
maculopapular rash
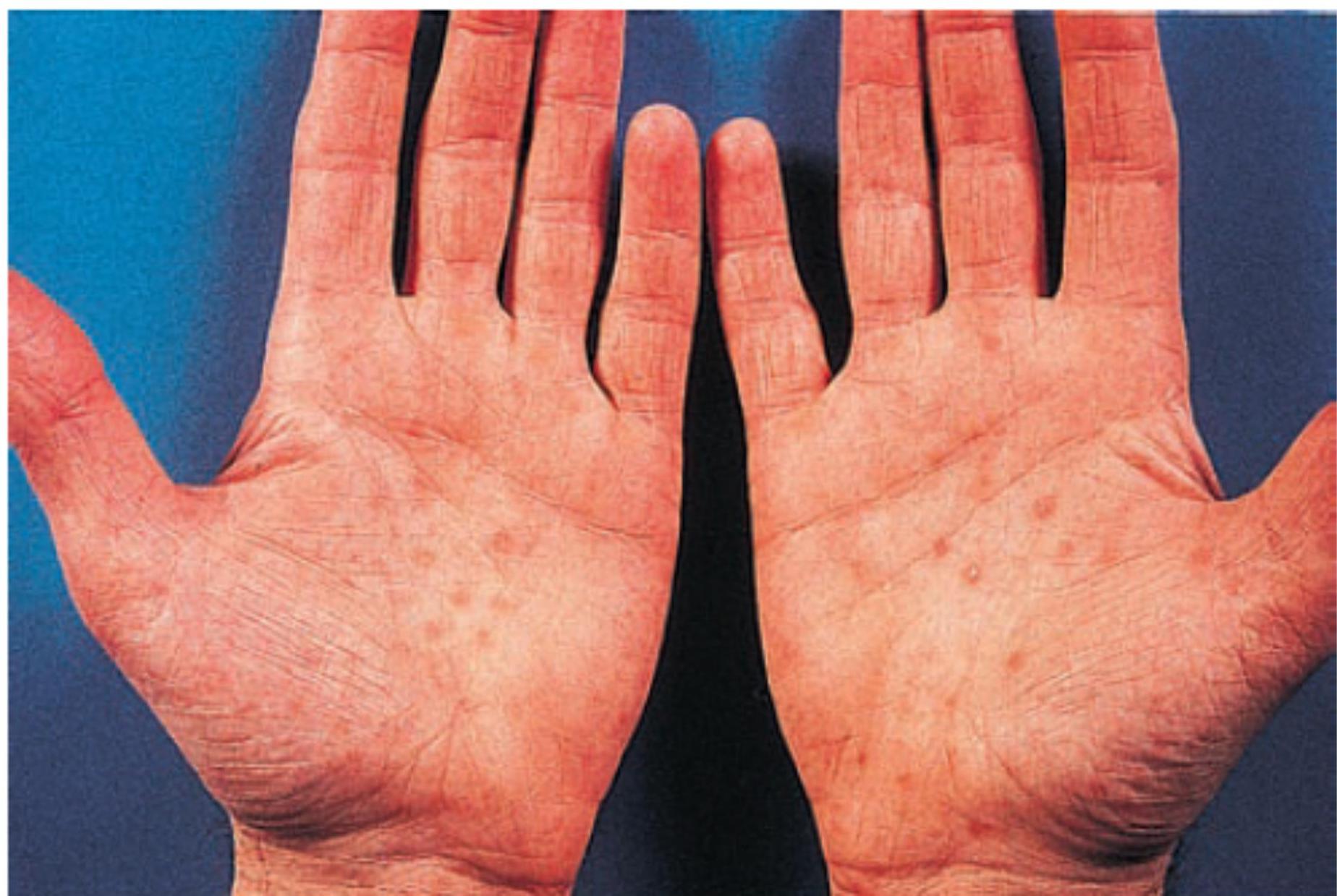 Fig. 4.41 Rash of secondary syphilis on the palms.
Fig. 4.41 Rash of secondary syphilis on the palms.
18
SYPHILIS- Secondary syphilis rash on body

19
Syphilis
- Gumm (granulomatous lesion involving skin, bone (skull, tibia, fibula) and viscera (liver))
- CVS – aortitis, aortic regurgitation
- Neurosyphilis – tabes dorsalis, general paralysis of insane (GPI)
Nablion
Syphilis
20
2-Congenital Syphilis:
- Becomes apparent 2-6 weeks after birth
- Early stages – still birth or failure to thrive
- Skin and mucus membrane lesion like secondary syphilis
- Late syphilis
Occurs after 2 years and seen as stigmata, Hutchinson’s teeth, sabre tibia
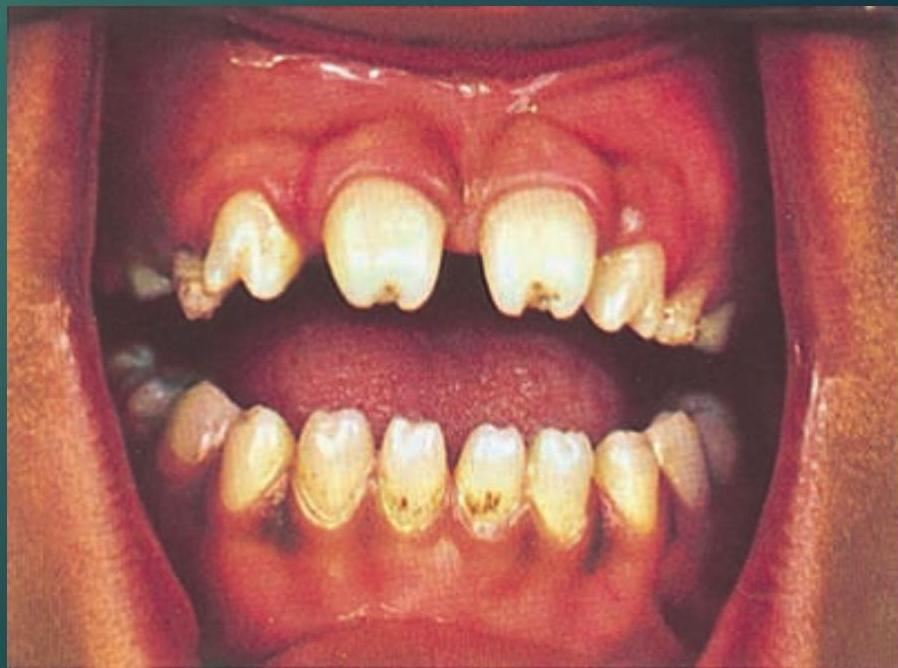
Picture showing Hutchinson’s Teeth
21
Syphilis
Investigation:
- T. Pallidium can not be cultured in vitro
- Most sensitive method of identification is dark ground microscopy – organism is found in primary chancre
- Trepenomal specific test
- T Pallidium Enzyme Immunoassay (EIA)
- Agglutination test (TPHA – T Pallidium Hemagglutination Assay)
- FTA-abs – Fluorescent Treponemal antibody absorb test (Most specific test)
- Trepenomal nonspecific test
- VDRL – Veneral disease Research Laboratory
- NOTE – Screening Test
- EIA – screening test of choice detects both IgM, IgG antibodies
22
Syphilis
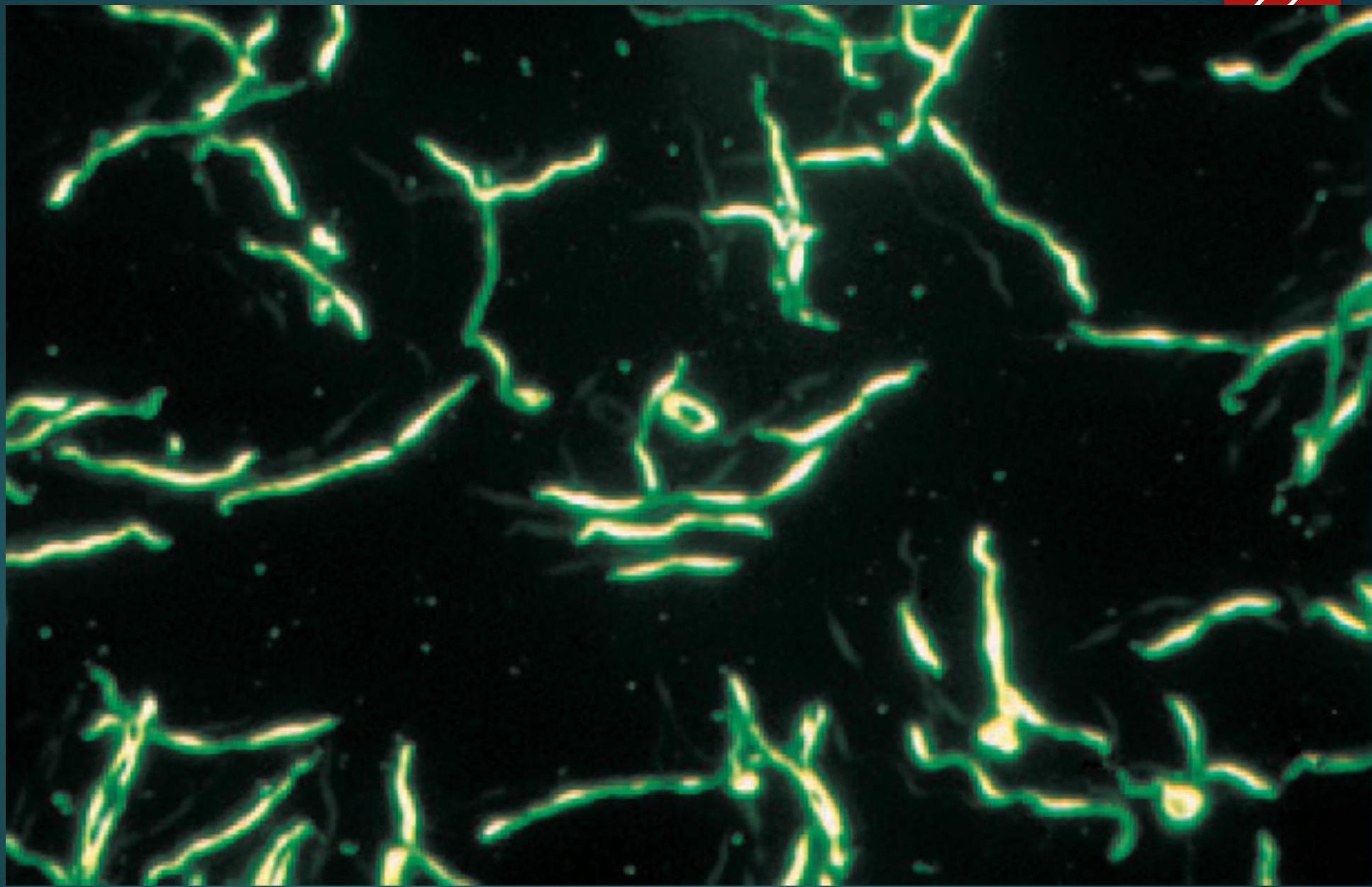
Photomicrograph of Treponema pallidum, as Seen with Dark-field Microscopy
23
Syphilis
Treatment:
-
Early syphilis (Primary & Secondary) is treated with long acting penicillin eg. Procaine penicillin 600 mg im daily for 10 days
-
Late stage syphilis procaine penicillin for 2-3 weeks
-
Other drugs
-
Doxycycline
-
Erythromycin
Very poor to cross BBB so that’s why it’s not affected in tertiary
24
CHLAMYDIA
- Chlamydia is STD caused by bacterium Chlamydia trachomatis, affects genitalia
- Most people have no symptoms.
- Symptoms in men include urethral discharge, burning with urination & Epididymitis.
- Symptoms in women include vaginal discharge, burning with urination.
25
CHLAMYDIA ( CONT )
- Investigation PCR on swab taken from cervix ( women ) and from urethra in men.
- culture
- Treatment- Chlamydia is treatable with antibiotics.
- Azithromycin – 1 gm as a single dose
- Doxycyclin – 100 mg 12 hrly for 07 days
- Important- Chlamydia is one of the most common STD infection worldwide.
Lymphogranuloma Venereum (LGV) 26
LGV is bacterial infection caused by Chlamydia Trachomatis (another specie) and is a sexually transmitted infection, affects lymphatic system. Highest incidence in Africa, India and south-east Asia.
Clinical features:
There are characteristic 3 stages:
- Stage I – primary lesion is painless ulcerating papule on the genitalia occurring 7-21 days following exposure.
- Stage II – A few days to weeks after this lesion heals, regional lymphadenopathy develops.
- The lymph nodes are painful, fixed and overlying skin is erythematous.
- Stage III – finally lymph node become fluctuant (buboes) and can rupture.
Lymphogarnuloma Venereum (LGV) 27

Lymphogarnuloma Venereum (LGV) 28
Diagnosis:
- Isolation of Chlamydia Tarchomatis from clinical lesion and tissue culture
- PCR
- C. Trachomatis serology
- Compliment fixation test
Treatment:
- Doxycycline 100 mg twice daily for 21 days or
- Erythromycin 500 mg 4 times daily for 21 days
29
Herpes Simplex
- It is one of the most common STI worldwide and caused by Herpes Simplex Virus (HSV)
- Peak incidence 16 – 24 years in both sexes
- Genital herpes is caused by HSV type II
- Oral Herpes is caused by HSV type I
- Herpes simplex infection which is life long, may be primary or recurrent.
- (in genital)
- Why?
Because virus has ability to establish latency in dorsal root ganglia by ascending through peripheral sensory nerve from site of inoculation. It is because of this recurrent attacks occur.
Zoster → in face and skin
30 Clinical Features:
Herpes Simplex
- Painful Condition
- Painful shallow ulcers develop which may coalesce (join)
- Tender inguinal lymphadenopathy occurs
- Usually accompanied by systemic symptoms like fever, myalgia, headache
- In women there is Vulval lesions and the cervix is almost always involved
- Rectal infection may lead to proctitis
- Neurological complication includes asceptic meningitis
- (negative culture)
Herpes Simplex
31
Diagnosis:
- Virus detection from lesion by PCR
- Virus culture
Management:
- Primary
- Aciclovir 200 mg 5 times per day for 5 days or
- Famciclovir 250 mg 3 times per day for 5 days or
- Valaciclovir 500 mg twice daily for 5 days
Recurrence
- Recurrent attacks are less severe
32
HUMAN PAPILLOMA VIRUS (HPV) WARTS
- Anogenital warts are most commonly sexually acquired infection caused by HPV. Clinical Features
- Warts appear around the external genitalia in women and peri anal region.
- In men penile shaft is most common site.
- Warts are called CONDYLOMA ACUMINATA.
HUMAN PAPILLOMA VIRUS (HPV) WARTS

HPV 34
Diagnosis It is essentially clinical
Treatment
- Podophyllin extract 15-25% solution apply locally once or twice weekly.
- Cryotherapy
- Electro cautery
- Laser ablation
35
TRICHOMONIASIS (TV)
- Trichomoniasis vaginalis (TV) is flagelleted protozoon and is predominantly sexually transmitted.
- Infected women may be asymptomatic.
- Major complaint is vaginal discharge which is offensive and there is local irritation
- Examination reveals frothy yellowish discharge and erythematous vaginal wall.
- Men may be asymptomatic or C/O urethral discharge, irritation or urinary frequency.
36
TRICHOMONIASIS (Cont)
D/D
Candidiasis – vulvovaginal infection with candida albicans is extremely common. Vaginal discharge is white, crudy, adherent.
- Predisposing Factors- pregnancy, Diabetes, corticosteroids, Immunosuppression
Bacterial vaginosis (BV)
-
BV is characterized by offensive, greyish white vaginal discharge
-
It is not regarded as STD without Sexual Contact
37
TRICHOMONIASIS
Diagnosis
- Phase contrast, dark ground microscopy of drop of vaginal discharge show T.Vaginalis swimming with a motion in 40- 80% of cases.
- Culture confirms the diagnosis
TREATMENT
- Metronidazole 2 gm orally as single dose or 400 mg twice daily for 7 days.
- Intra vaginal Tinidazole
38
HUMAN IMMUNE DEFICIENCY VIRUS HIV AND AIDS
- First described in 1981.
- HIV identified in 1984
Routes of Transmission
- Sexual intercourse (vaginal and anal)
- Mother to child - Trans placental, Breast feeding
- Contaminated blood, blood products
- Organ donations
- Contaminated needles (IV drug abusers), injections, Needle stick injuries.
39
HIV AND AIDS
The virus:
- HIV virus belongs to lenti virus group of retrovirus family.
- It is RNA virus, the reverse transcriptase polymerase enzyme converts viral RNA into DNA
There are two types
- HIV 1 – most common globally
- HIV 2 – confined to west Africa
HIV AND AIDS
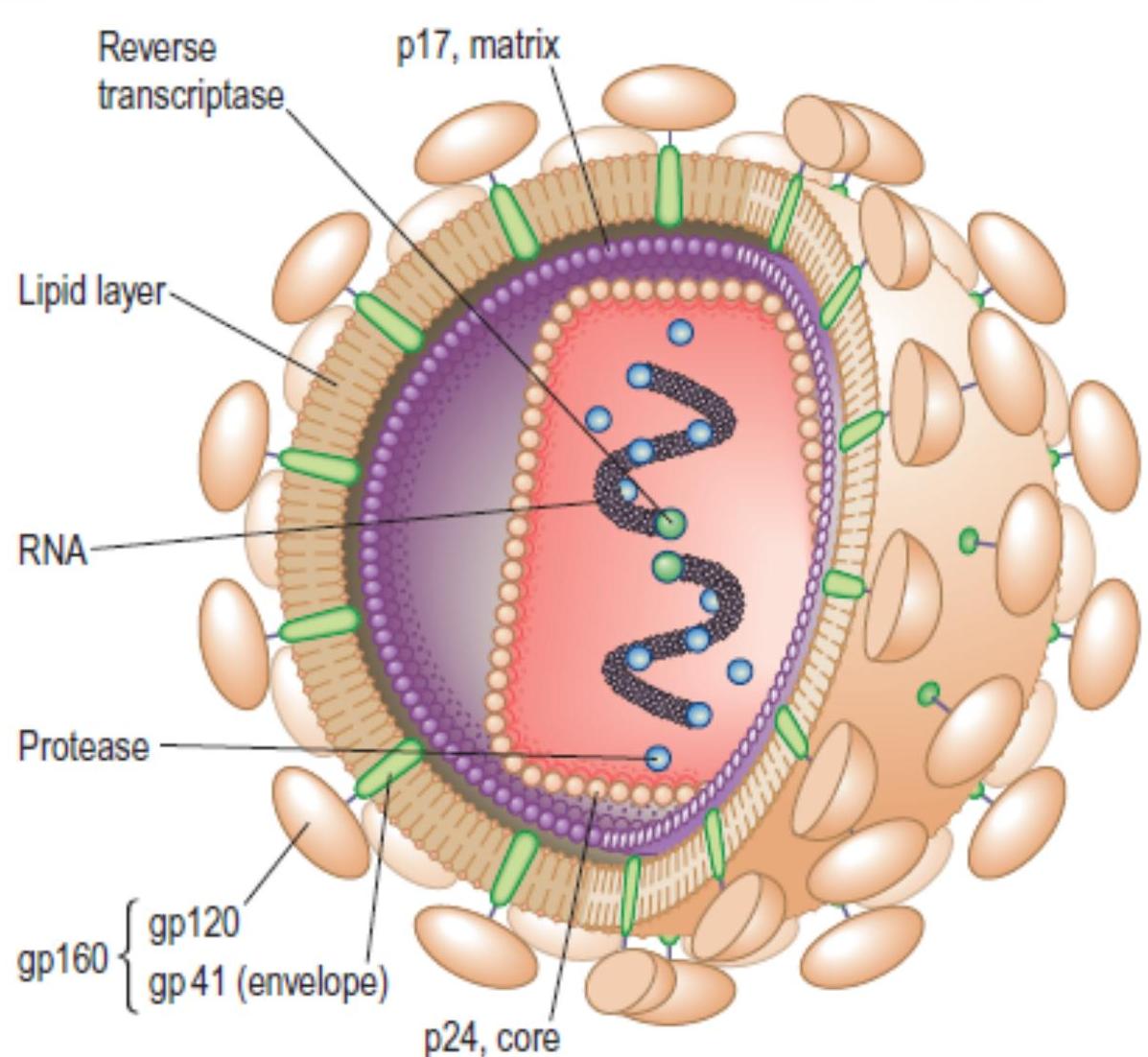
Fig. 4.43 Structure of HIV. Two molecules of single-stranded RNA are shown within the nucleus. The reverse transcriptase polymerase converts viral RNA into DNA (a characteristic of retroviruses). The protease includes
41
HIV AND AIDS
Tests:
- Simple and rapid HIV antibody assays are available giving results in minutes.
- Serum / Plasma, oral fluid, whole blood and urine can be tested
- IgG antibodies to P24 (Anti P24)
- Viral P24 antigen (P24 Ag)
- Virus culture
- Antibodies to HIV (IgG) cross placenta therefore all babies born to HIV infected women will have antibodies at birth.
42
HIV AND AIDS
Clinical Features HIV/AIDS:
- When CD4 count is below 200/mm³ there are clinical manifestations of AIDS. (Normal CD4 500–1500/mm³)
when CD4 decrease in number: AIDS defining Conditions:
- Candidiasis of Bronchi, Trachea, Lungs
- Candidiasis of Oesophagus
- Herpes simplex
- Histoplasmosis
- Kaposis Sarcoma
- TB
- Lymphoma
- Pneumocystitis Jiroveci Pneumonia
- Toxoplasmosis
- HIV related Encephalopathy
HIV AND AIDS
i Box 4.17 AIDS-defining conditions
- Candidiasis of bronchi, trachea or lungs
- Candidiasis, oesophageal
- Cervical carcinoma, invasive
- Coccidioidomycosis, disseminated or extrapulmonary
- Cryptococcosis, extrapulmonary
- Cryptosporidiosis, chronic intestinal (1-month duration)
- Cytomegalovirus (CMV) disease (other than liver, spleen or nodes)
- CMV retinitis (with loss of vision)
- Encephalopathy, HIV-related
- Herpes simplex, chronic ulcers (1-month duration); or bronchitis, pneumonitis or oesophagitis
- Histoplasmosis, disseminated or extrapulmonary
- Isosporiasis; chronic intestinal (1-month duration)
- Kaposi’s sarcoma
- Lymphoma, Burkitt’s
- Lymphoma, immunoblastic (or equivalent term)
- Lymphoma (primary) of brain
- Mycobacterium avium-intracellulare complex or M. kansasii, disseminated or extrapulmonary
- Mycobacterium tuberculosis, any site
- Mycobacterium, other species or unidentified species, disseminated or extrapulmonary
- Pneumocystis jiroveci (formerly P. carinii) pneumonia
- Pneumonia, recurrent
- Progressive multifocal leucoencephalopathy
- Salmonella septicaemia, recurrent
- Toxoplasmosis of brain
- Wasting syndrome, due to HIV
44
HIV AND AIDS
Course of HIV infected patients:
- 1-Incubation, Seroconversion, Primary illness, 2-Asymptomatic stage
- 3-Late course (AIDS)
Pathogenesis
- Interrelationship between HIV and the Host Immune system is the basis of pathogenesis of HIV disease
- HIV is now manageable chronic condition but only in those who are aware of their diagnosis and start their therapy earlier
45
HIV AND AIDS
1-Incubation, Seroconversion, Primary illness:
- First 2-4 weeks after infection may be silent both clinically and serologically
- In many people a self limiting non specific illness occurs 3-6 weeks after exposure.
- Symptoms include fever, myalgia, arthralgia, lethargy, lymphadenopathy, mucosal ulcers.
- The illness last for 3 weeks and recovery is usually complete.
(pil will be Asymptomatic “Latency”)
46
HIV AND AIDS
1- Incubation, Seroconversion, Primary illness (cont)
- Antibodies to HIV maybe absent during early stage but level of circulating RNA is high and P24 antigen may be detected
2- Clinical latency / Asymptomatic stage
-
Majority of people are asymptomatic for variable length of time but virus continues to replicate and person is infectious. normal 500 and more
-
Most people with HIV have gradual decline in CD4 count over a period of 10 years, before progression to AIDS (Acquired Immunodeficiency Syndrome)
-
Subgroup of patients with asymptomatic infection have PGL (Persistent Generalized Lymphadenopathy) (may activate later and develop AIDS at any time)
47
3-HIV AND AIDS
Table 4.51 Some mucocutaneous manifestations of HIV infection (see also Ch. 23)
| Skin | Mucous membranes |
|---|---|
| Dry skin and scalp | Candidiasis: |
| Onychomycosis | oral |
| Seborrhoeic dermatitis | vulvovaginal |
| Tinea: | Oral hairy leucoplakia |
| cruris | Aphthous ulcers |
| pedis | Herpes simplex: |
| Pityriasis: | genital |
| versicolor | oral |
| rosea | labial |
| Folliculitis | Periodontal disease |
| Acne | Warts: |
| Molluscum contagiosum | oral |
| Warts | genital |
| Herpes zoster: | |
| mutidermatomal | |
| disseminated | |
| Papular pruritic eruption | |
| Scabies | |
| Icthyosis | |
| Kaposi’s sarcoma |
48
HIV AND AIDS

Vasculatis Carcours bad sign
Kaposi’s Sarcoma in AIDS Patient Young Pit Specialty
HIV AND AIDS
appraationistic infection
49
Table 4.52 Major HIV-associated pathogens
| Protozoa | Bacteria |
|---|---|
| Toxoplasma gondii | Salmonella spp. |
| Cryptosporidium parvum | Mycobacterium tuberculosis |
| Microsporidia spp. | M. avium-intracellulare |
| Leishmania donovani | Streptococcus pneumoniae |
| Isospora belli | Staphylococcus aureus |
| Haemophilus influenzae | |
| Viruses | Moraxella catarrhalis |
| Cytomegalovirus | Rhodococcus equii |
| Herpes simplex | Bartonella quintana |
| Varicella zoster | Nocardia |
| Human papillomavirus | |
| JC polyoma virus |
Fungi and yeasts
Pneumocystis jiroveci
(formerly P. carinii)
Cryptococcus neoformans
Candida spp.
Dermatophytes (Trichophyton)
Aspergillus fumigatus
Histoplasma capsulatum
Coccidioides immitis
HIV AND AIDS
50
 Fig. 4.46 Untreated CMV retinitis.
Fig. 4.46 Untreated CMV retinitis.
Pizza like lesion
d 51
HIV AND AIDS
- Compilation therapy
- 2-3 together
- to maintain CD4
- > 200
- Forever
Drugs used for HIV/AIDS:
- Zydovudine
- Efavirenz
- Fosamprenavir
- Maraviroc
- Enfuvirtide
52
Thank You