Paediatrics Discussion OSCE
Acetaminophen Poisoning
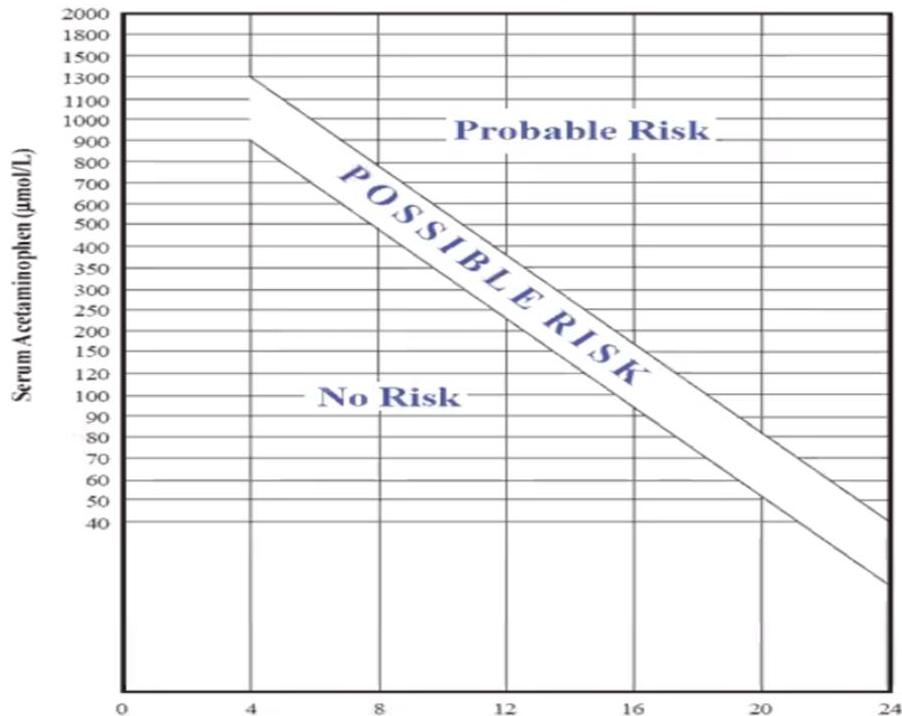
Chart:
- Rumack Nomogram (paracetamol poisoning)
Importance:
- To give antidote to patient
- To assess probable risk
- Proper treatment
When Used:
- Only 4 to 24 hours post-ingestion - because affect of Antidote
- Timing: Take blood levels exactly at 4 hours post-ingestion for nomogram interpretation
Treatment:
- N-Acetylcysteine (NAC) if levels are above the treatment line or if hepatic failure is present
Note:
- Nomogram may not be applicable in extended-release preparations
Hours Since Ingestion *adapted from Medical Toxicology, Eliminate and Introduce, 1988.
Ambiguous Genitalia / Congenital Adrenal Hyperplasia

karyotyping to know female or male
Clinical Presentation: 3-week-old infant, vomiting (5 days), dehydration, tachycardia (rapid heart rate), ambiguous genitalia.
Pathophysiology: Genetic abnormality in steroid synthesis (most common enzyme deficiency is 21-hydroxylase deficiency).
Diagnosis? 21-hydroxylase deficiency (Congenital Adrenal Hyperplasia).
Lab findings?
- Hyponatremia
- Hyperkalemia
- Hyperglycemia
- Normal BUN
- High 17-hydroxyprogesterone
- Low serum cortisol
- High ACTH (primary) / Low ACTH (secondary)
Investigations?
- Karyotyping
- Pelvic & kidney US
- 17-hydroxyprogesterone level
- Serum cortisol, ACTH
Management?
- Hydrocortisone + fludrocortisone + oral salt (mineralocorticoids to replace aldosterone)
- Admission hydration, glucocorticoids
- Acute crisis: Normal Saline bolus for fluid resuscitation; IV Hydrocortisone (most important treatment)
Shock management?
- ABCD, IV fluid 20 ml/kg
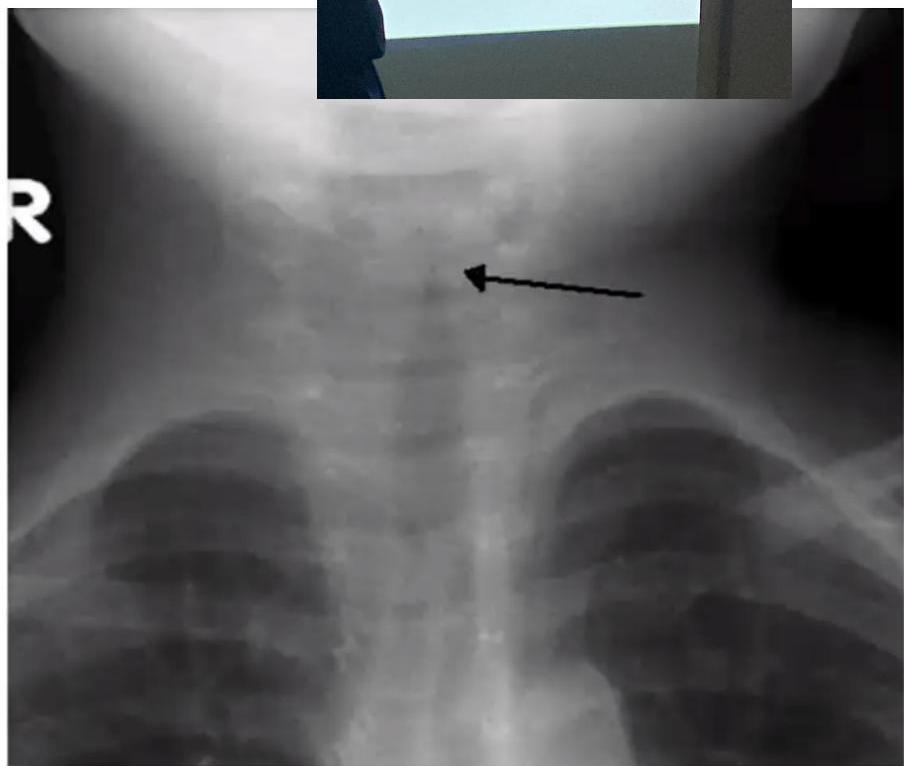
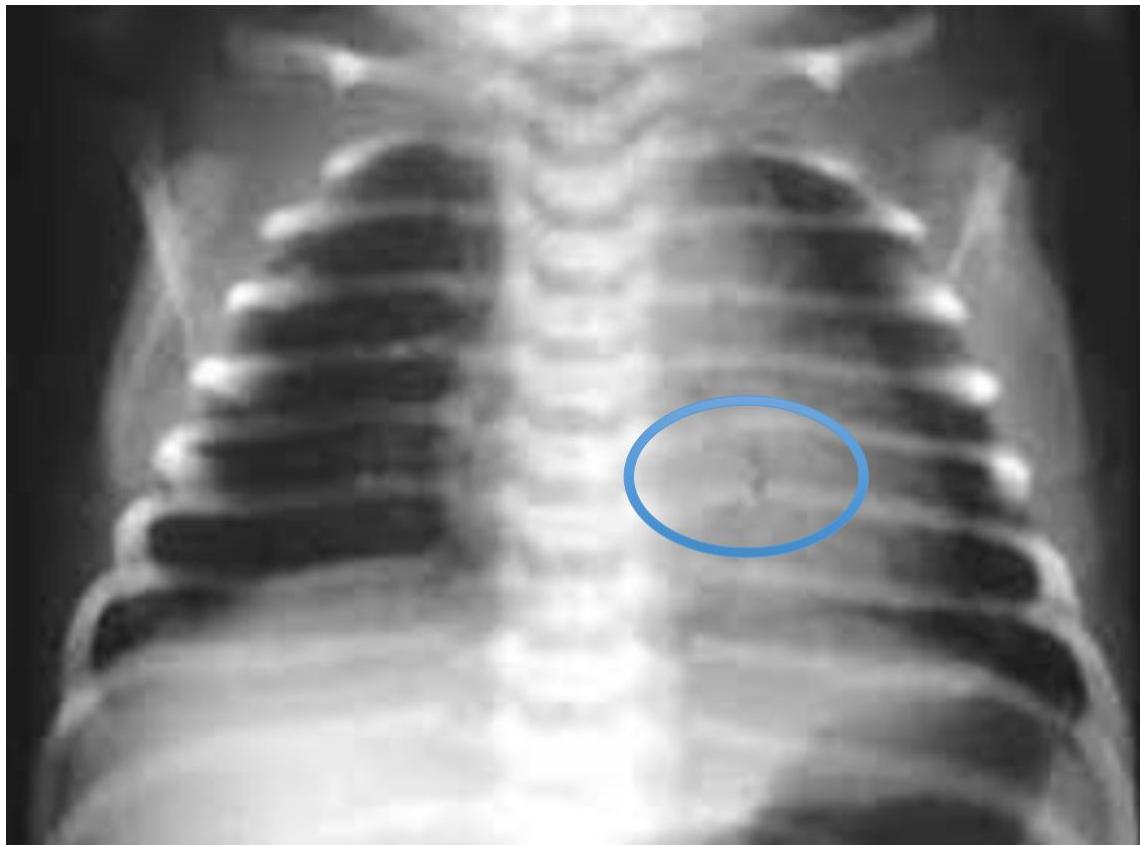
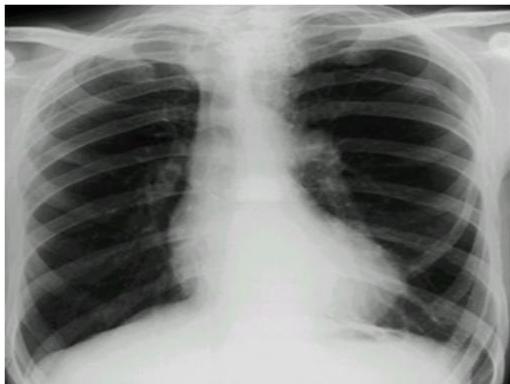
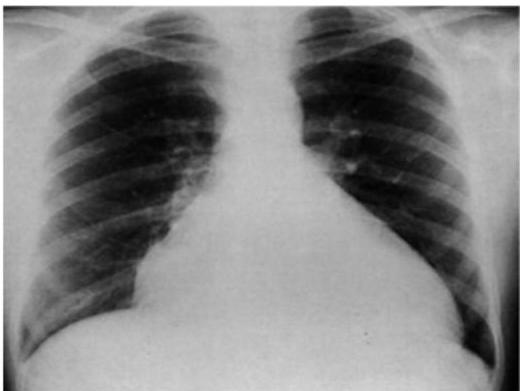
Asthma with Pneumothorax / Emphysema (CXR)
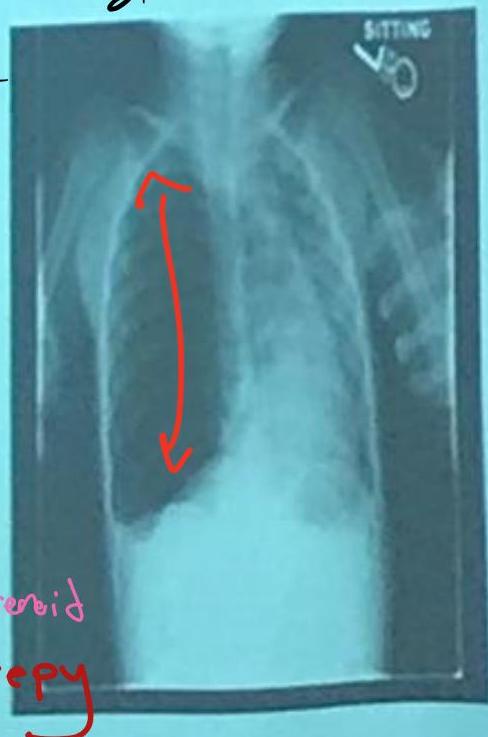
 in This PIC Be Curfiat → Check Countage of the lung
Hint: Loss of contour of lung
in This PIC Be Curfiat → Check Countage of the lung
Hint: Loss of contour of lung
- Check if hyperinflated
The hint is loss of Couture of lung in the emphysema → we doubt see?
Scenario: 5 year old with 3 days of acute asthma, progressive SOB, cyanosis.
CXR findings?
- Right-sided pneumothorax (or horizontal pneumothorax), subcutaneous emphysema, with left mediastinal shift
- Loss of lung opacity
- Mucous plug causing collapse/obstruction
- Other mentions in original: “Liver & mucus”, “Pneumonitis”
Examination Findings (Chest):
- Hyperresonance (increased sound on percussion)
- Pulsus paradoxus
- Decreased breath sounds
Management?
- Address the underlying cause (e.g., decompression for pneumothorax, airway clearance)
- Bronchodilator, inhaled steroid
- Suction + physiotherapy
- If pneumothorax: chest tube — 5th intercostal space, anterior axillary line
- Possible intubation
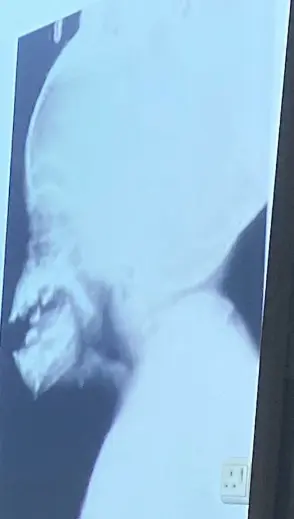
Acute Epiglottitis
Station recall: Video about epiglottitis and how to manage.
Scenario: 3 year old non-vaccinated boy presents with fever, worsening sore throat, and respiratory distress. Exam reveals toxic appearing child, temp 40°C, drooling of saliva, stridor and sitting in tripod position (trunk leaning forward, neck hyperextended, chin thrust forward).
Q1: What is likely diagnosis?
- Acute epiglottitis
- Finding: Thumb sign (on lateral view)
Q2: How do you manage?
- Emergency airway management in the Operating Room (OR) with anesthesia/ENT
- Call the Anesthesia team and prepare for Endotracheal intubation
- First management: intubation and tracheostomy if failed
- All patients should be monitored in ICU
- IV Antibiotics
- Give Rifampin for close contacts
Causes: Staph most common (Streptococcus pneumoniae + Group A strept) if vaccinated, or Haemophilus influenzae type B if not vaccinated

Croup (Laryngotracheobronchitis)
Radiographic Sign: Steeple or pencil sign of the proximal trachea
Signs:
- Inspiratory stridor
- Barking cough
- Hoarseness
Causes:
- Parainfluenza virus type 1
- RSV
- Influenza virus
Management:
- Mild symptoms: Single dose of oral dexamethasone
- Moderate to severe symptoms:
- Supportive care: humidified air or oxygen, intravenous fluids
- Epinephrine
- Dexamethasone
- Surgical intervention if patient doesn’t improve
Intraosseous Infusion


Indications:
- Administration of fluids and medications (Note: Any medication or fluid can be administered via IO)
- Unacceptable IV line
- Patient in shock needing rapid access
Contraindications/Precautions:
- Infection at entry site (cellulitis)
- Osteogenesis imperfecta
- Fracture
- Severe bleeding
- Multiple failed attempts (change site after 2nd trial)
Procedure:
- After 2nd trial, change site
Intubation and Mechanical Ventilation

Procedure? Intubation and mechanical ventilation.
Indications? Respiratory or mechanical insufficiency, ineffective gas exchange (coma, respiratory arrest).
Complications? Pneumothorax, supraglottic stenosis.
Infant CPR (2-rescuer)

Procedure? Cardiopulmonary Resuscitation (CPR) — 2-rescuer technique.
Description?
- One rescuer: bag valve mask ventilation using C-E maneuver (C-shaped fingers hold mask, E-shaped fingers lift jaw)
- Second rescuer: compressions with 2 fingers, 1/2 inch deep
What is the name of the device in the hand of the person at the upper end of bed? Bag valve mask.
Compression-ventilation ratio (2 rescuers)? 15:2. 15 compressions and 2 ventilations.
Positive Pressure Ventilation (PPV)

Procedure:
- PPV by Ambu bag (single rescuer technique)
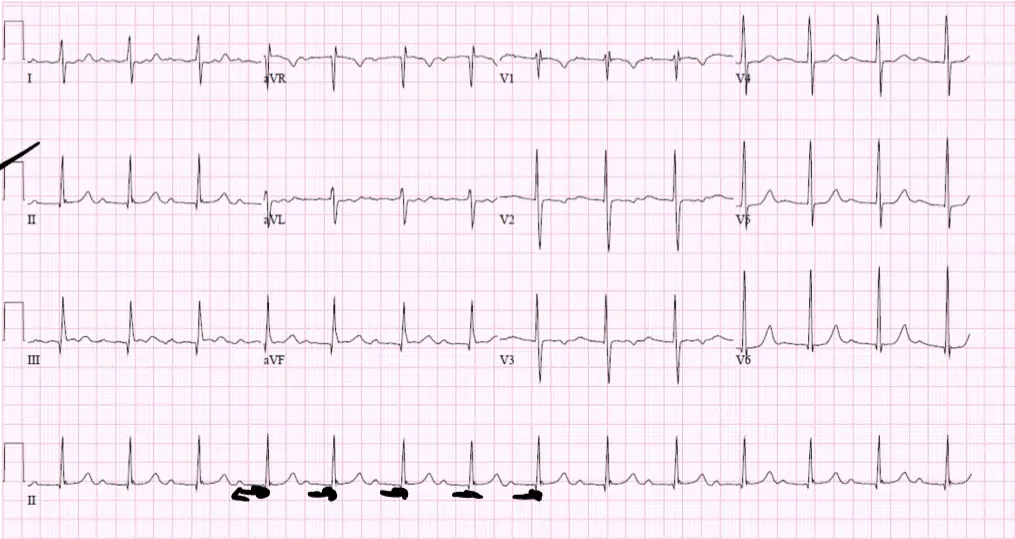
Supraventricular Tachycardia (SVT)
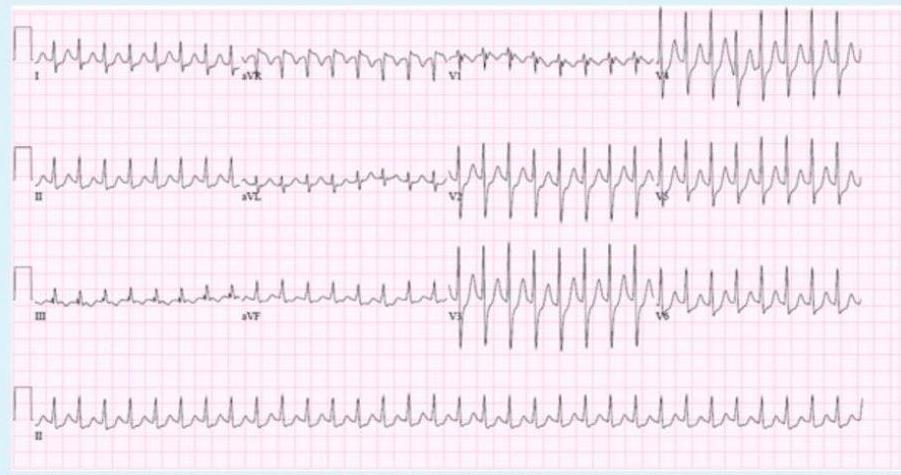
A 1 year old child is brought to the ER because his parents thought his heart was pounding as they were putting him to bed. EKG was done in ER.
Diagnosis? Supraventricular tachycardia (SVT).
Findings:
- Abnormal P waves
- Narrow QRS complex
- Small T waves
- ↑ HR
Causes?
- WPW syndrome
- Ectopic focus / conduction abnormality
ECG Details:
- Narrow QRS complex, HR ~280 bpm, regular RR interval, absent or unclear P-waves
Management (child alert, normal BP)?
- Vagal maneuvers (first step if stable)
- B. Adenosine IV (first line medication if stable)
- Maintenance therapy: Beta-blockers or Class 1C anti-arrhythmics (e.g., Flecainide) for recurrent cases
Management:
- If patient stable: Vagal maneuvers (carotid massage, valsalva maneuver, ice bags, cold shower) first, then IV Adenosine
- If patient unstable/hypotensive: Synchronized Cardioversion
- Rapid heart rate control → Beta Blockers
Paroxysmal SVT

Findings:
- Abnormal P waves
- Narrow QRS complex
- Small T waves
- ↑ HR
Management:
- Rapid heart rate → Beta Blockers
- If patient in shock: cardioversion
- If patient unstable: medications like adenosine, amiodarone
- If patient stable: carotid massage, valsalva maneuver, ice bags, cold shower
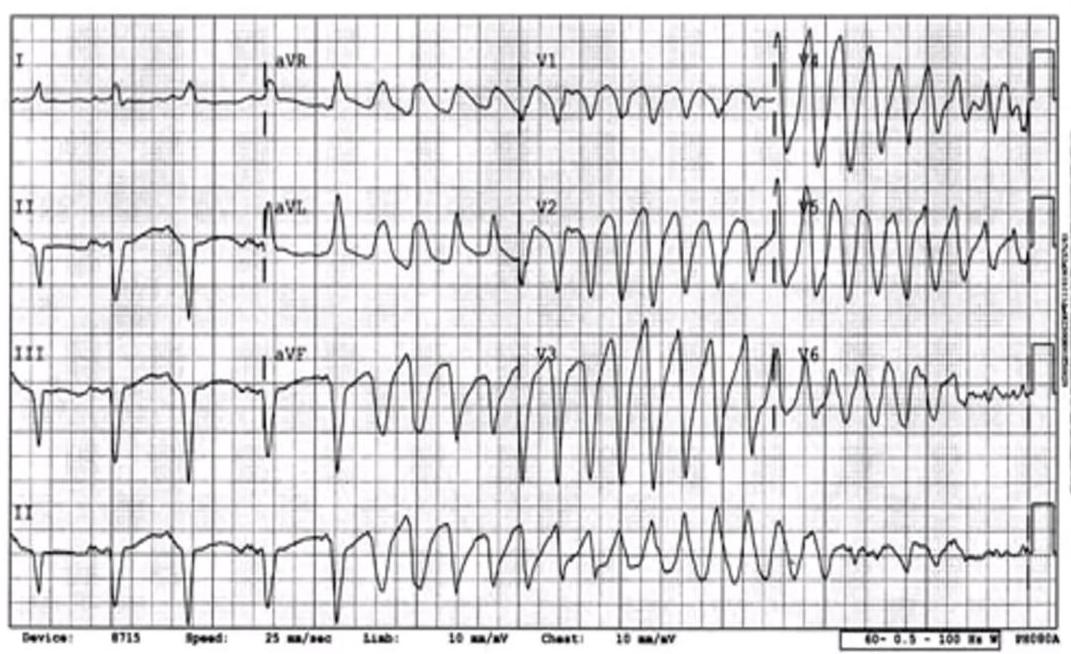
Monomorphic Ventricular Tachycardia
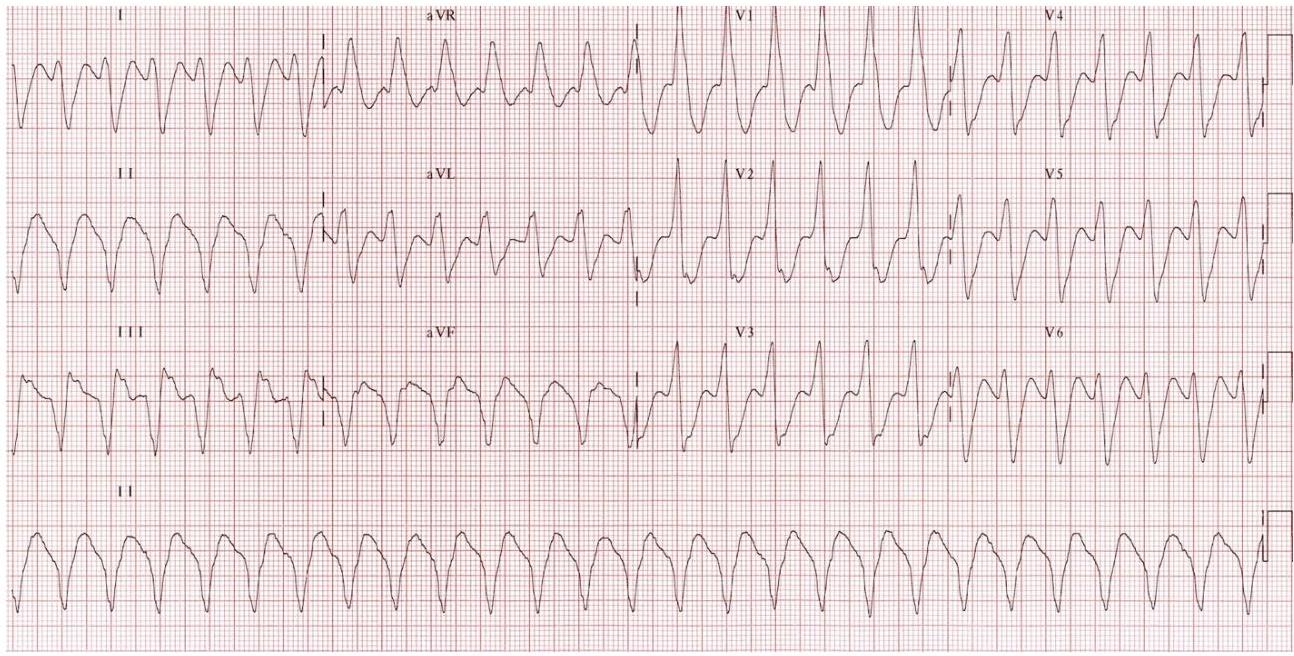
ECG Features?
- Tachycardia (HR: 150 bpm)
- Regular rhythm
- Wide QRS complex
- No discernible PR interval
Diagnosis? Monomorphic ventricular tachycardia.
Causes?
- Myocardial ischemia
- Myocarditis
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
Treatment:
- Stable: Amiodarone or lidocaine (CCB, BB, Amiodarone, Adenosine)
- Low BP but pulse present: Cardioversion
- No pulse: Defibrillation
Monomorphic VT Monomorphic ventricular tachycardia

Finding: Regular wide QRS with v tachycardia
Treatment:
- Stable: Amiodarone or lidocaine
- Low BP but pulse present: Cardioversion
- No pulse: Defibrillation
Defibrillation:
- High energy
- No need for sedation
- No need for synchronization
Give 2 causes:
- Myocardia ischemia
- Myocarditis
How to Manage:
- CCB
- BB
- Amiodarone
- Adenosine
- Cardioversion
- Pulseless: defibrillation
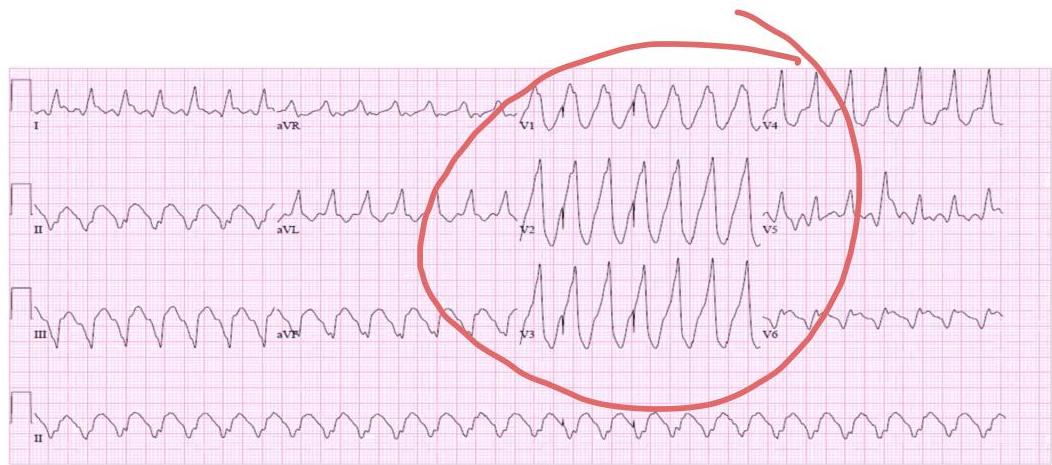
Polymorphic VT (Torsades de Pointes)
ECG Findings:
- Wide QRS + ↑HR
- Twisting around the line
Cases:
- Myocardial ischemia
- Hypokalemia
- Prolonged QT syndrome
Management:
- MgSO₄
- Cardioversion if in shock
WPW (Wolff-Parkinson-White)

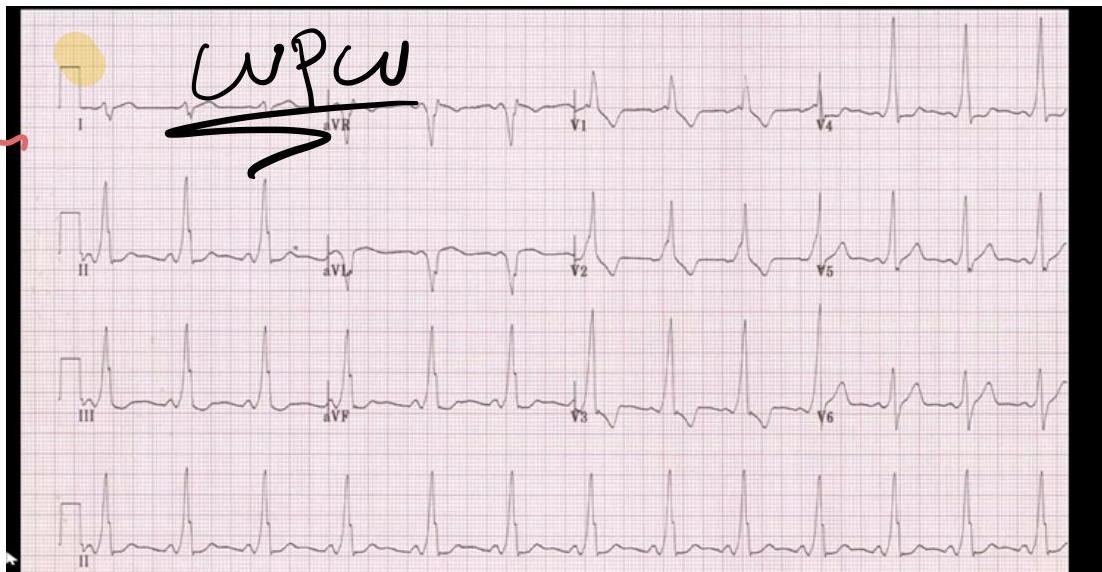
Signs:
- Delta wave (slurred upstroke of QRS, not always clear)
- Short PR interval
- Wide QRS
Complications:
- SVT
- Atrial fibrillation
- Ventricular fibrillation
Management:
- Observation (intermittent can end by itself)
- Medication
- Catheter ablation
Asystole
Management:
- Start CPR immediately
- Note: Often progresses from V-fib if not treated promptly
- Medications: Epinephrine (may give amiodarone)
- No shock (only give shock in case of V.fib or tachycardia)
- Cardiac massage
Automated External Defibrillator (AED)
Uses:
- Cardioversion
- Defibrillation
- Pacing for ↓ HR
Indications:
- Pulseless ventricular tachycardia (VT)
- Ventricular fibrillation (VF)
- Cardiac arrest due to or resulting in VF
Contraindications:
- Dysrhythmias
- Multifocal atrial tachycardia
Error:
- Not making paddles closer (may shock self)

Tilt Table Test
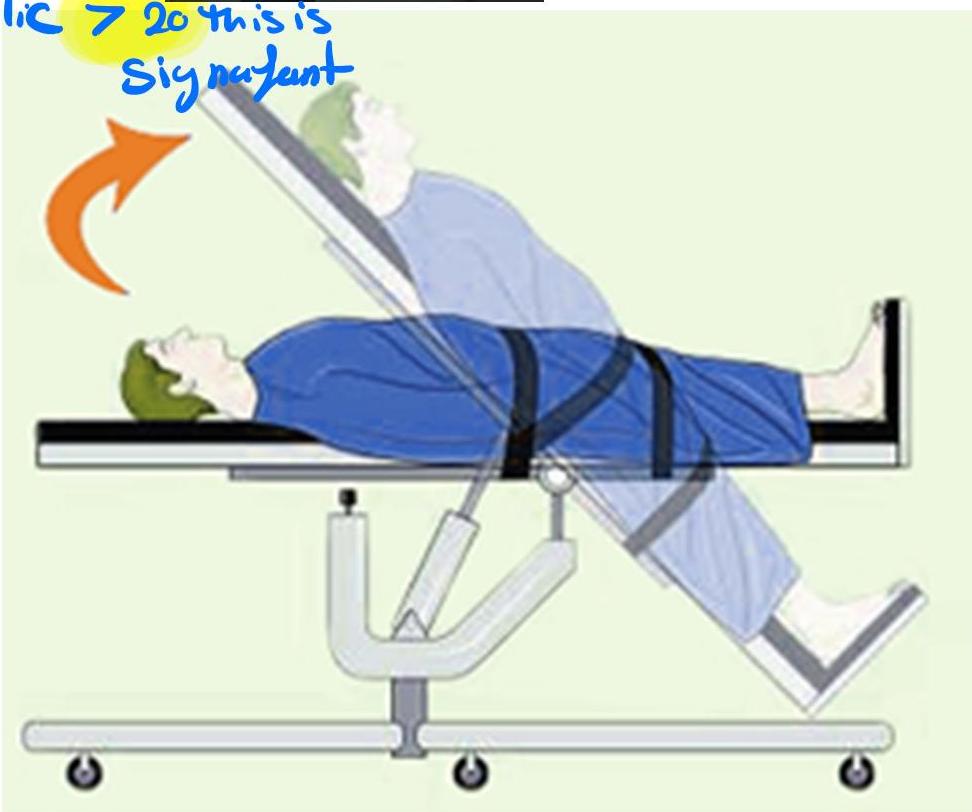
Technique:
- Tilt table test
- If drop in systolic >20, this is significant
Indications:
- Postural hypotension
- Diagnosis of vertigo / paroxysmal vertigo (positional changes)
- Syncope
- Tachycardia with standing
Contraindications:
- Coma
- Severe anemia
- Severe heart failure
Valsalva Maneuver

Indications:
- Supraventricular tachycardia
- Decrease arterial refractory period
- Cases of syncope
Time:
- 5-10 seconds
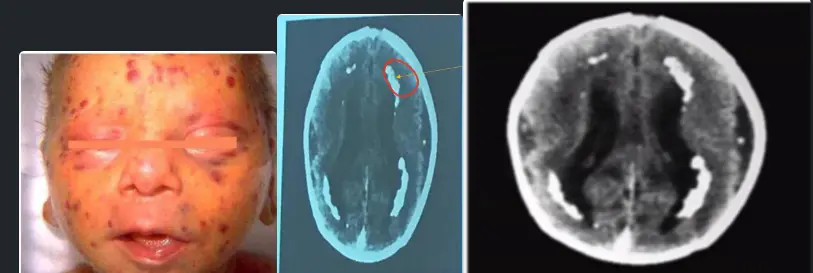
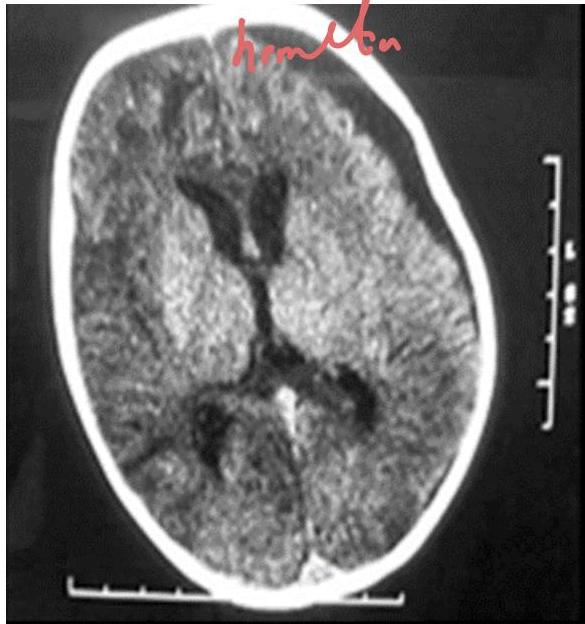
Congenital Toxoplasmosis
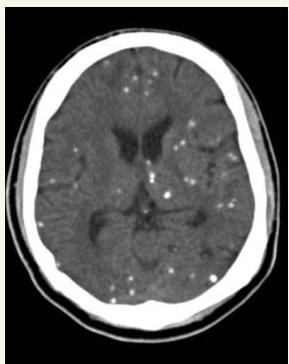

This child was delivered with jaundice, HSM, wide spread rashes and progressive head enlarging. Mather gave history of contact with cats early in her pregnancy.
- Diagnosis?
- Congenital Toxoplasmosis “Lipic Vaginal” (Lipic Vaginal), - differential - CMV if paraventricular
Findings:
- Jaundice
- Hepatosplenomegaly
- Widespread rashes
- Progressive head enlargement
- Mother history of contact with cats early in pregnancy
Investigation? Serology (IgM and IgG).
CT Finding: Intracranial calcification (extensive cerebral calcifications) — scattered pattern.
- CNS calcifications (tram calcification pattern)
- Calcification in the border called “tram calcification”
- CMV has calcification around the ventricles (C-shape)
CMV Infection
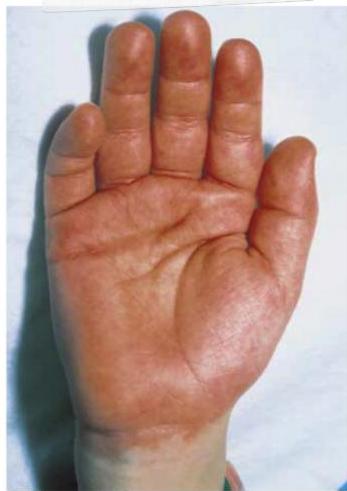
 year old girl has had recurrent episodes of swelling of her hand and feet for last 6 month, these 12 episodes occur following exercise and emotional stress last for 2-3 days and resolve spontaneously. The last episode was accompanied abdominal pain, vomiting and diarrhea the results of routine laboratory workup are normal an older sister and a maternal uncle have had similar episodes as shown in photographs below
year old girl has had recurrent episodes of swelling of her hand and feet for last 6 month, these 12 episodes occur following exercise and emotional stress last for 2-3 days and resolve spontaneously. The last episode was accompanied abdominal pain, vomiting and diarrhea the results of routine laboratory workup are normal an older sister and a maternal uncle have had similar episodes as shown in photographs below
Diagnosis? CMV.
CT finding? Periventricular calcification (vs Toxo which is scattered).
Findings:
- Hepatosplenomegaly
- Microcephaly
- Jaundice
- Hearing loss
- Non-blanching rash
- Small for gestational age
- Calcification around the ventricles (C-shape)
- History: Mother with mild febrile illness in 1st trimester
Memory aid:
- C-shape calcification = CMV
Hypoxic Ischemic Encephalopathy (HIE)
Therapeutic Hypothermia

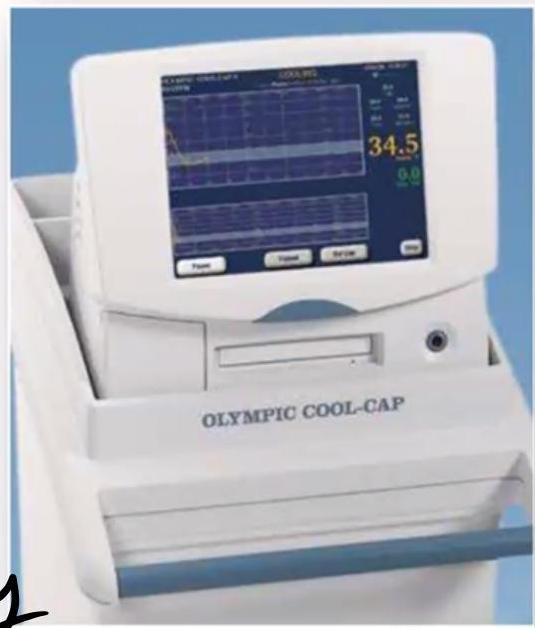

Scenario: One day old baby with severe HIE - Full term newborn admitted to NICU due to severe birth asphyxia (hypoxic ischemic encephalopathy).
Q1: What is the mode of therapy?
- Therapeutic hypothermia Head-selective (or whole body) therapeutic hypothermia (e.g., Olympic Cool Cap).)
- Temperature: 33.5-34.5°C (optimal ~33.5°C)
- Duration: started within 6 hours, used for 72 hours (or 48 hours - 2-3 days)
Q2: What is the effect of this therapy?
- Neuroprotection
- Decrease brain injury
- Reduce energy requirements and level of free radicals
- Preserves anti-oxidants
- Inhibit apoptosis
- Reduce damage caused by 2nd stage
Indications:
- Severe birth asphyxia
Hirschsprung Disease
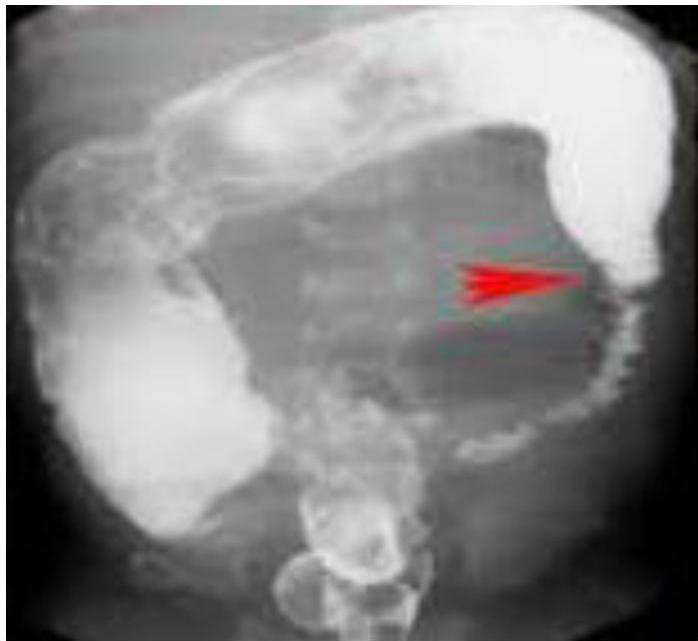
 describe x-ray
There is fecal impaction, transitional zone (dilated part proximally and constricted part distally)
describe x-ray
There is fecal impaction, transitional zone (dilated part proximally and constricted part distally)
Barium Enema Findings:
- Fecal impaction
- Transitional zone (dilated part proximally, constricted part distally)
- Narrow distal segment
- Dilated proximal segment
- Funnel-shaped dilatation at level of transitional zone
Causes:
- Absence of ganglion cells (aganglionic megacolon)
Presentations:
- Delayed passage of meconium
- Chronic constipation
- Toxic megacolon
- Signs of intestinal obstruction
Confirmation:
- Full-thickness rectal biopsy (to check for absence of ganglion cells)
Management:
- Resuscitation, NPO and IV fluids
- Antibiotics
- Rectal tube, irrigation
- At age 6-12 months: resection of aganglionic segment and anastomosing (formal pull-through procedure)
Hemolytic Uremic Syndrome (HUS)
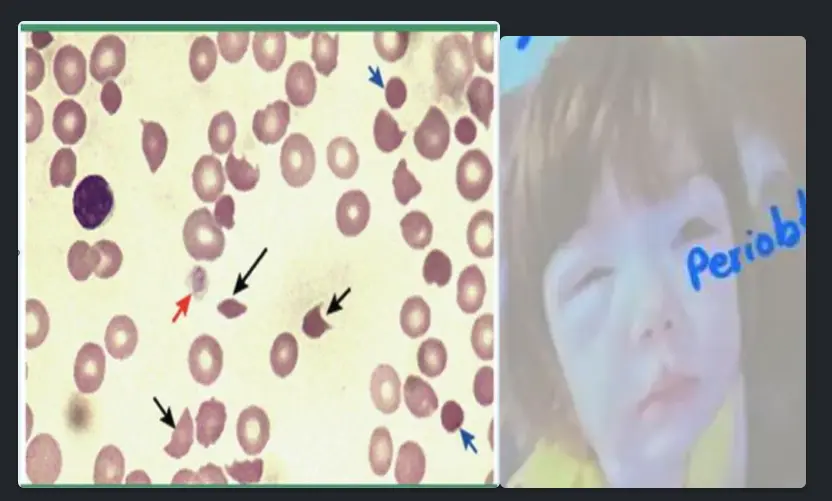
Scenario: 4 year old admitted with abdominal pain and acute onset of bloody diarrhea. Recent outbreak related to a fast food restaurant. Peripheral blood smear shown. Patient developed acute renal failure, microangiopathic haemolytic anaemia and thrombocytopenia. The picture shows his peripheral blood smear.
Peripheral smear abnormality? Schistocytes (fragmented red blood cells).
Diagnosis? Hemolytic Uremic Syndrome (HUS).
Classic triad?
- Thrombocytopenia
- Acute renal failure
- Microangiopathic hemolytic anemia
Signs:
- Bloody diarrhea
- Petechiae
- Oliguria
- Dehydration
- Hypertension
- Seizure
Causes?
- E. coli O157:H7
- Shiga toxin
- Shigella species
- Viral infections
- Congenital factors
Lab investigations?
- Peripheral smear (schistocytes)
- Hemoglobin level (decreased)
- Elevated creatinine
- Normal PT/PTT
Management (supportive):
- Hydration/Fluid replacement
- Managing complications of renal failure (dialysis, HTN control)
- Blood transfusion
Intussusception



- 18 Months old boy presented with crying and vomiting.
- A bloody stool was passed on the day of the imaging examinations (classically described as “currant jelly” stool).
Diagnosis? Ileocolic intussusception.
Investigation? Barium enema.
Sign?
- Cut-off sign in the middle
- Coiled spring appearance / spring sign / target sign
Etiology:
- Idiopathic
- Secondary to: HSP, intestinal polyps
Emergency:
- Type of obstruction
Treatment:
- NPO/IV fluids
- NGT aspiration
- IV antibiotics
- Hydrostatic reduction with Barium/air enema
- Laparotomy and resection if needed
Complications:
- Ischemia and necrosis
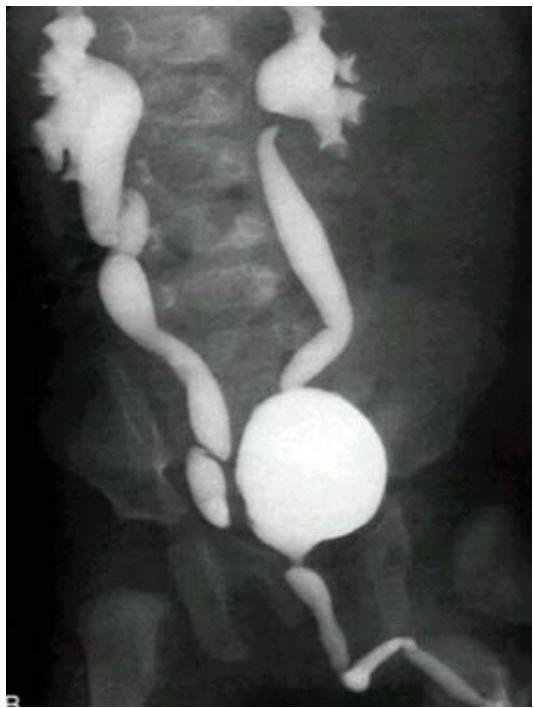
Posterior Urethral Valve (PUV)


Modality:
- MCUG / VCUG (voiding cystourethrogram) only in boys
Findings:
- Dilated proximal urethra
- Dilated ureter
- Dilated bladder
- Dilated posterior urethra
Can be diagnosed antenatal and prevented!
Complications:
- Renal failure
- UTI
Treatment:
- Surgical removal of the valve
- Catheter or drain procedure as temporary measure
Vesicoureteral Reflux (VUR) — MCUG/VCUG

Scenario: Infant referred for evaluation following recurrent UTI.
Investigation? Micturating cystourethrogram (MCUG) / Voiding cystourethrogram (VCUG)
Findings?
- Posterior urethral valve
- Dilated ureters and bladder
- Tortuous ureters
- Dilated renal pelvis and calyces bilaterally (hydronephrosis)
Diagnosis? Vesicoureteral Reflux (VUR) — grade 4-5.
Diagnosis & Grading
- Studies: Renal US (Typically first); MCUG (to confirm diagnosis); RNC (for follow-up).
International Grading System (MCUG Findings):
| Grade | Description / Findings |
|---|---|
| Grade I | Into a nondilated ureter only. |
| Grade II | Into the pelvis and calyces without dilation. |
| Grade III | Mild to moderate dilation of ureter, pelvis, and calyces; minimal blunting of fornices (become close). |
| Grade IV | Moderate ureteral tortuosity and dilation of pelvis and calyces (adhered to each other). |
| Grade V | Gross dilation; significant tortuosity; loss of papillary impressions; blunting of calyces (bilateral/severe). |
Constipation
-
Management: * Acute: Disimpaction (if severe fecal material in rectum).
- Maintenance: Lactulose, hydration, and lifestyle changes.
Perthes Disease
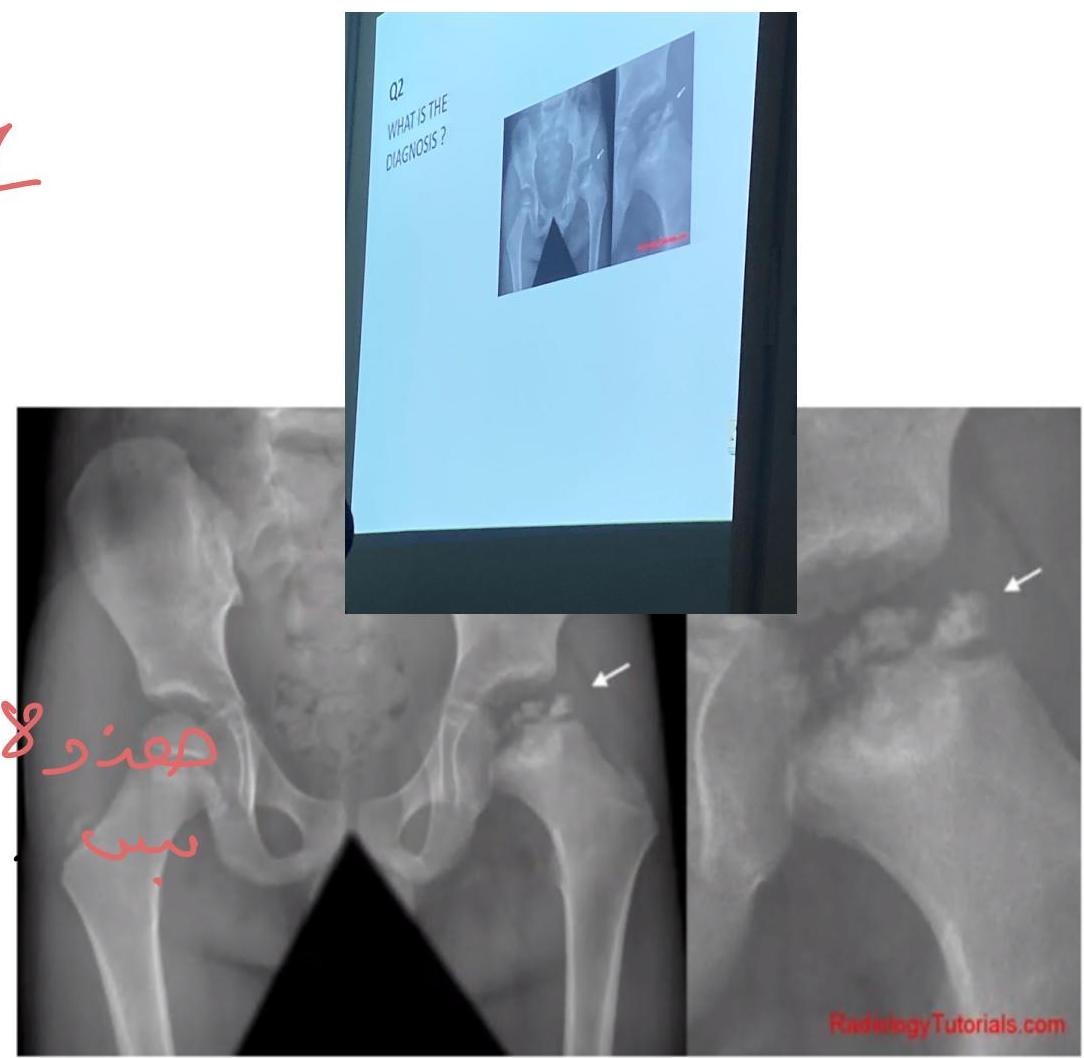
Diagnosis:
- Perthes disease (Legg-Calvé-Perthes disease)
Cause:
- Avascular necrosis of the femoral head (appears as a “broken” or flattened end of the femur)
Most Common Cause of Limping in Children:
- Transient synovitis
Risk Factors:
- Sickle cell disease
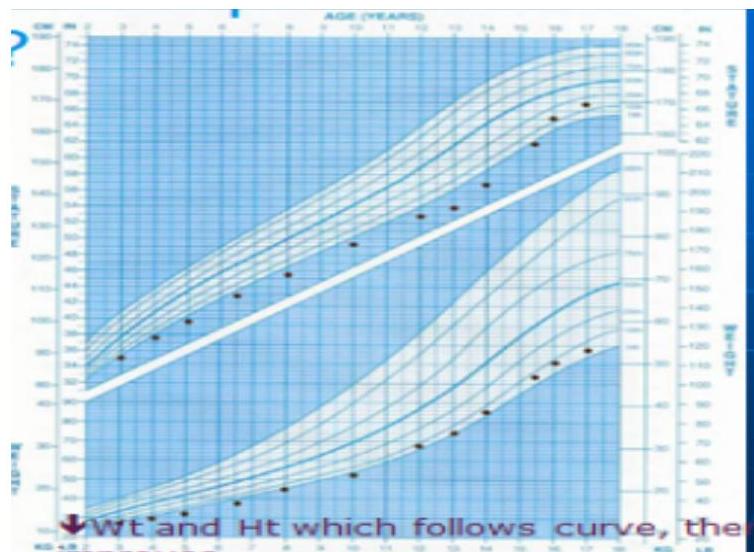
Types of Failure to Thrive
Recurrent FTT (Child Abuse)
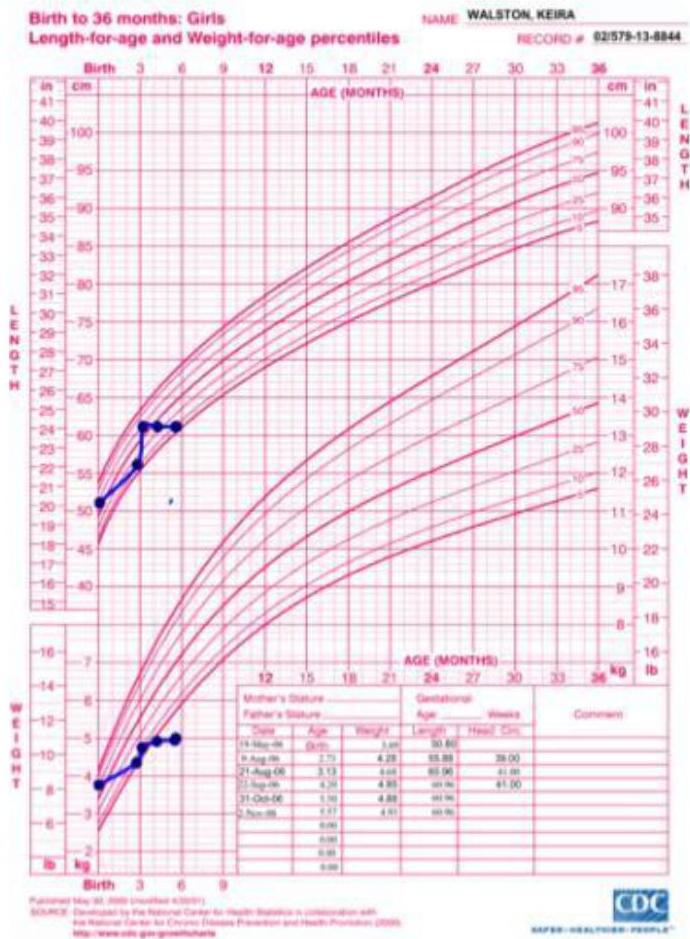
Type:
- Birth up to 36 months
- Length for age and weight for age percentile
Description:
- Both weight and length lines cross 2 centile chart twice
Diagnosis? Child abuse (recurrent failure to thrive, untreated).
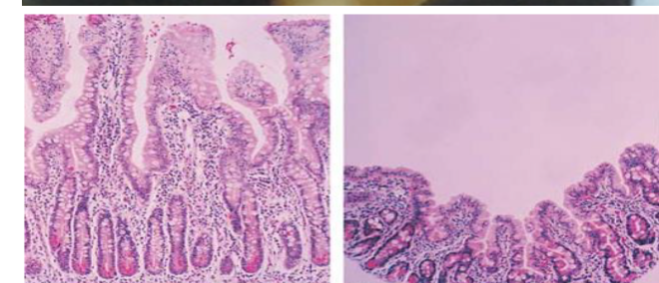
Celiac Disease (FTT Pattern)
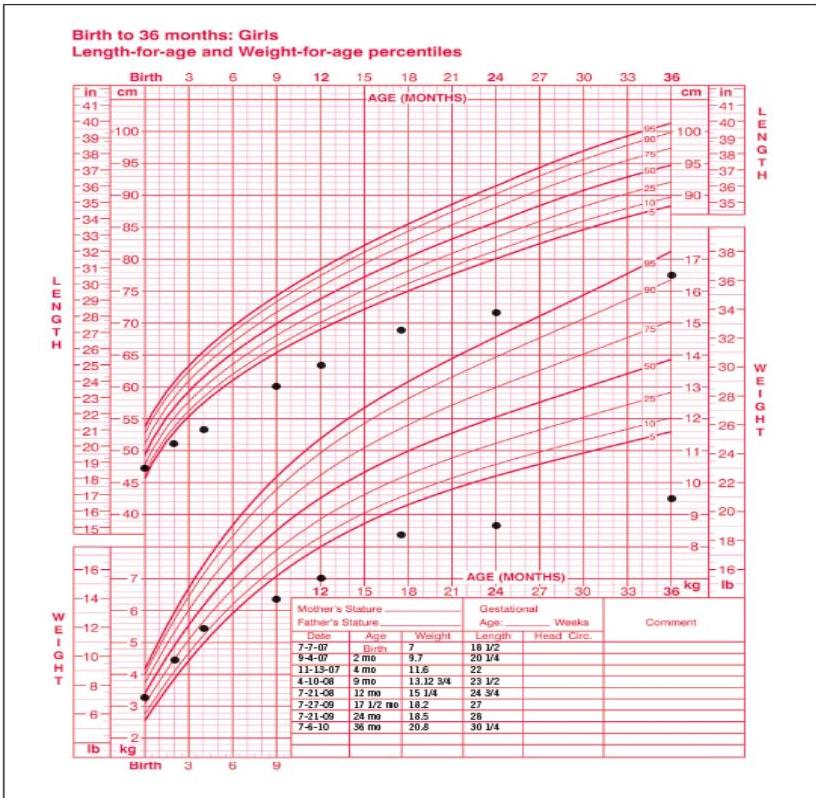
Description:
- Weight and length from birth to age 36 months
- Deceleration of growth apparent at age 9 months
Diagnosis:
- Gluten sensitivity disease (Celiac)
Next Investigation:
- Endomysial antibodies
Congenital Abnormality Pattern
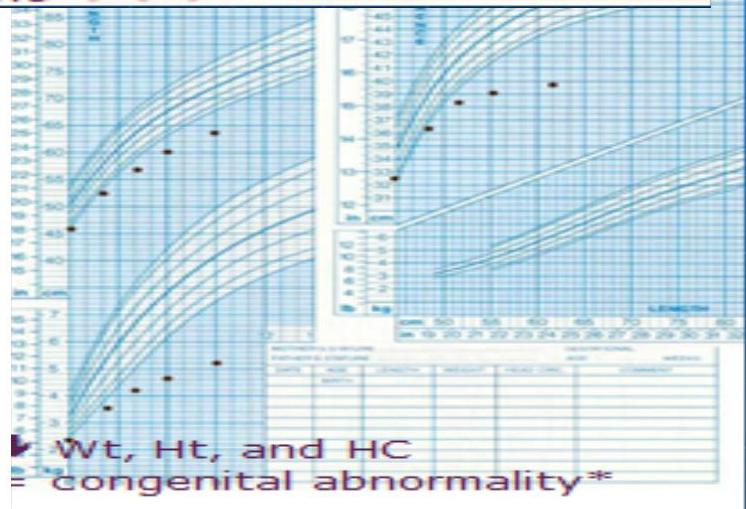
Findings:
- Both weight, height, and head circumference decreased
- Due to congenital abnormality
Recurrent FTT Pattern
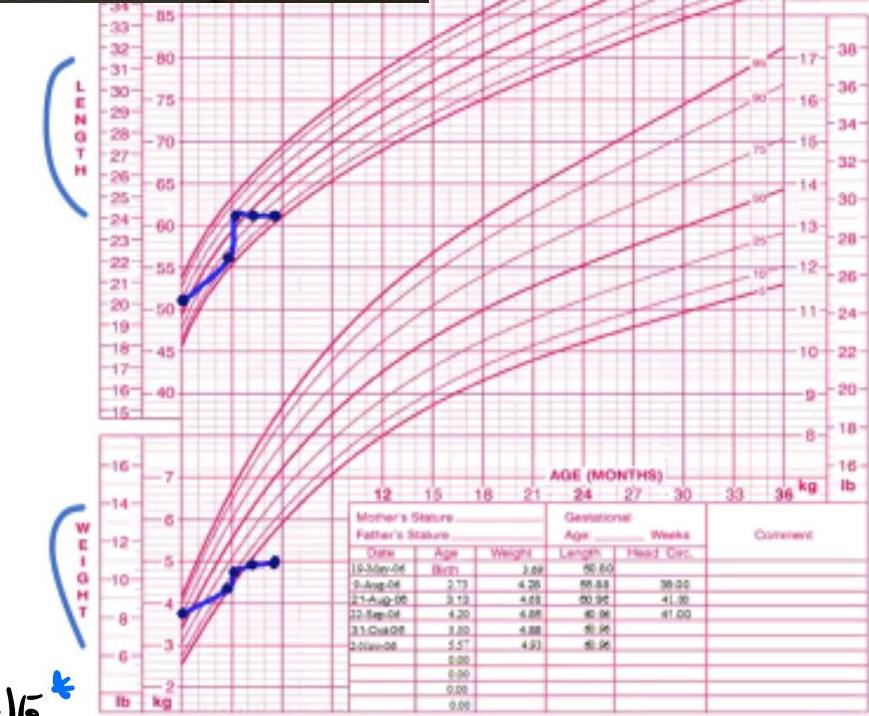
Description:
- Girl: Normal start → FTT → improved → FTT again
- Pink chart for girls
- Both height and weight cross 2 percentile downward twice
Diagnosis:
- Recurrent failure to thrive
Causes:
- Child abuse
- Malabsorption (e.g., celiac disease)
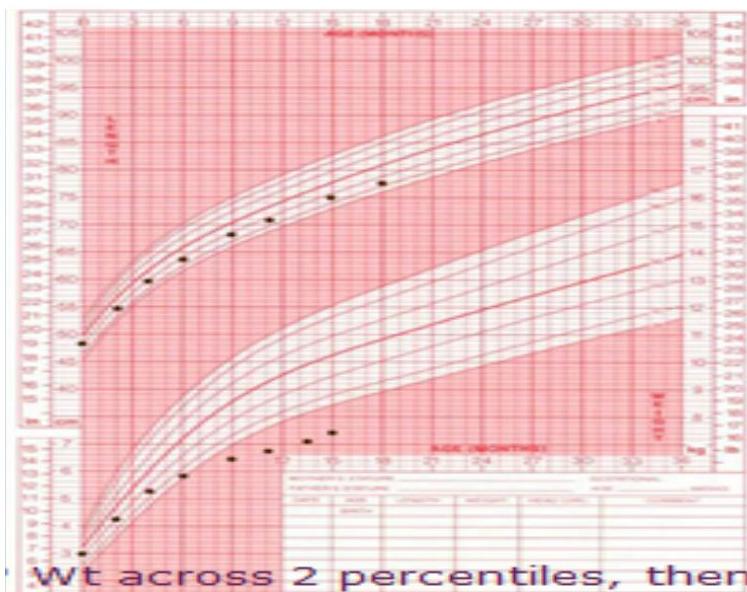
Rib Fracture
- Clinical: Failure to thrive (weight crossing two centile lines downwards twice).
Finding:
- Rib fracture
- Healed fracture / Calluses on ribs
Diagnosis:
-
Child abuse
-
Differential: Rickets (Rachitic rosary) typically presents with bilateral, symmetric rib enlargement in an infant (e.g., 4 months old).
Intermittent FTT Pattern
Description:
- Girl’s growth chart showing intermittent failure to thrive
IUGR Pattern
Description:
- Boy showing FTT, both weight and height affected
- Eventually improved (maybe due to IUGR)
DKA / Urine Dipstick
Scenario: 12 year old, known DM case.
Diagnosis? Diabetic Ketoacidosis (DKA).
Urinalysis findings?
- pH: LOW
- Ketones: HIGH
- Glucose: HIGH
- High protein (high albumin:creatinine ratio 2.2:25)
Management? IV fluid, insulin infusion.
Causes of DKA?
- Non-compliance
- Infection
- Wrong dose
- Expired insulin
- Stress
- Pump failure
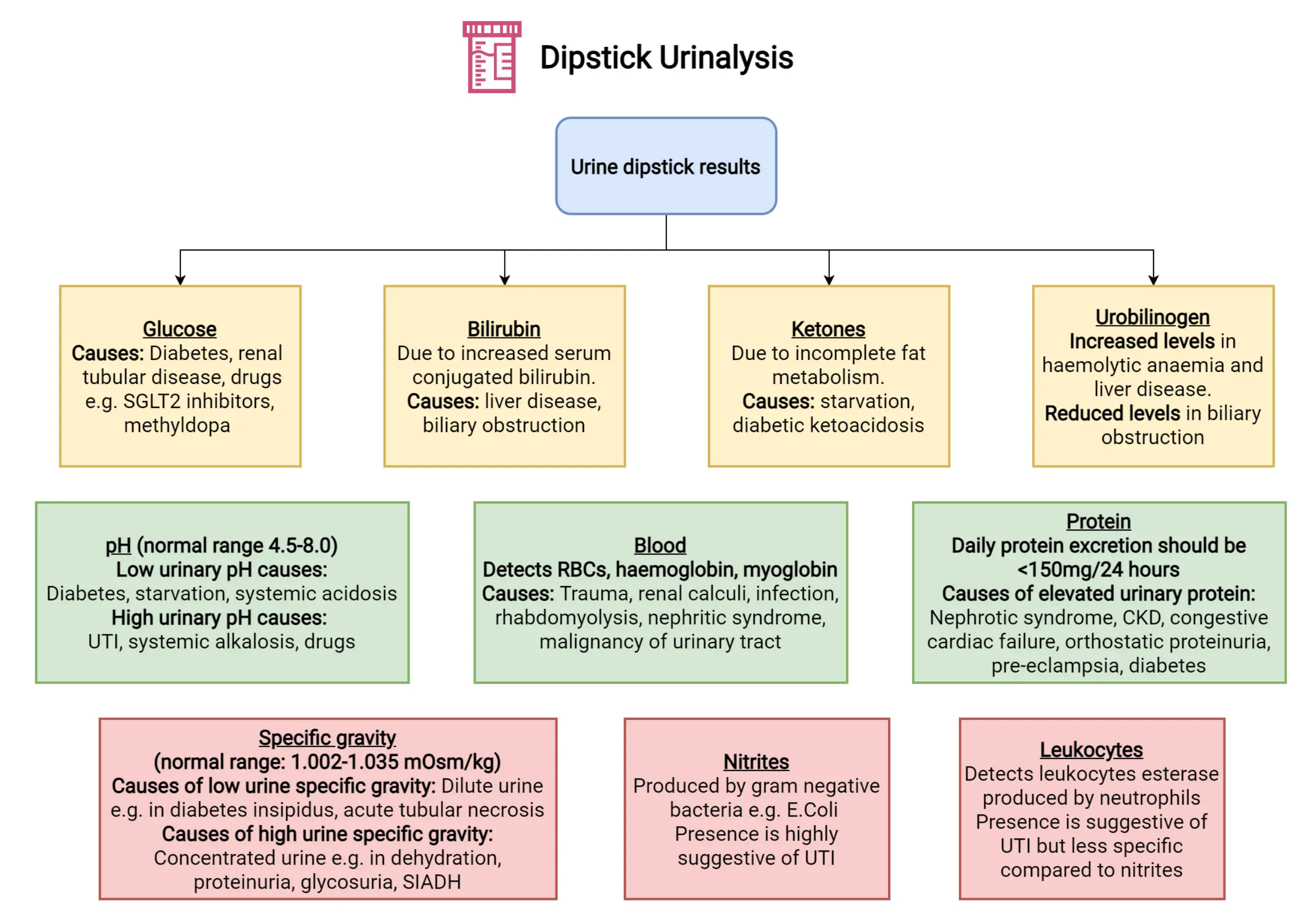
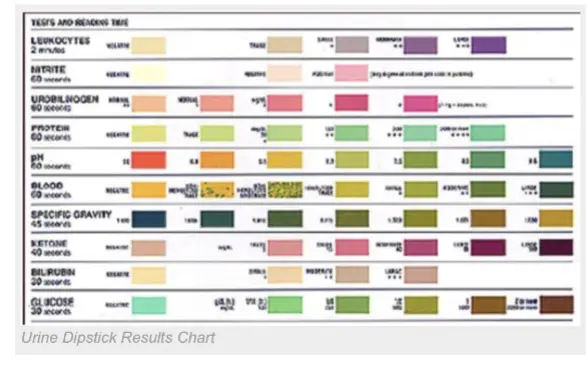
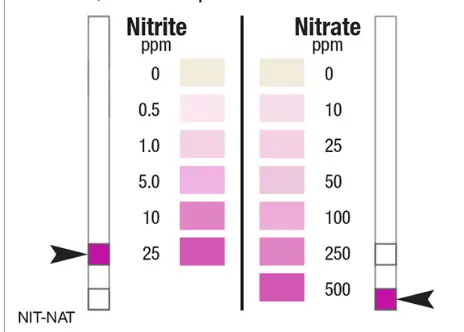
Urine Dipstick
- UTI: Nitrite and Leukocyte Esterase positive.
- DKA: Ketonuria and Glycosuria.
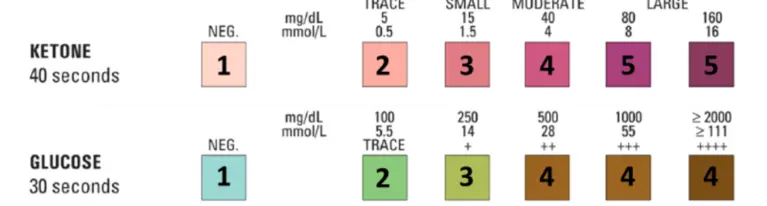
- Chronic Nephropathy: Proteinuria.

Peak Expiratory Flow Meter

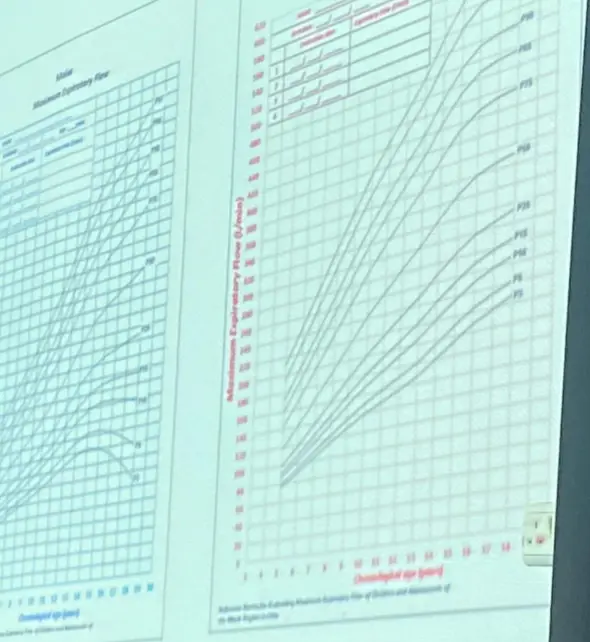
- end Exisiotomy meter What it measures:
- FEV1 (Forced Expiratory Volume in 1 second)
Spirometry / Peak Expiratory Flow Meter


Device? Spirometry / Peak expiratory flow meter
What does it measure? PEF (Peak Expiratory Flow) / FEV1.
Aerochamber Spacer with Mask
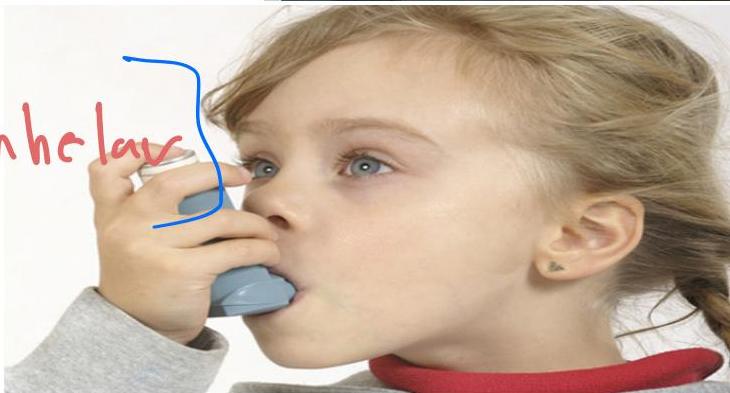

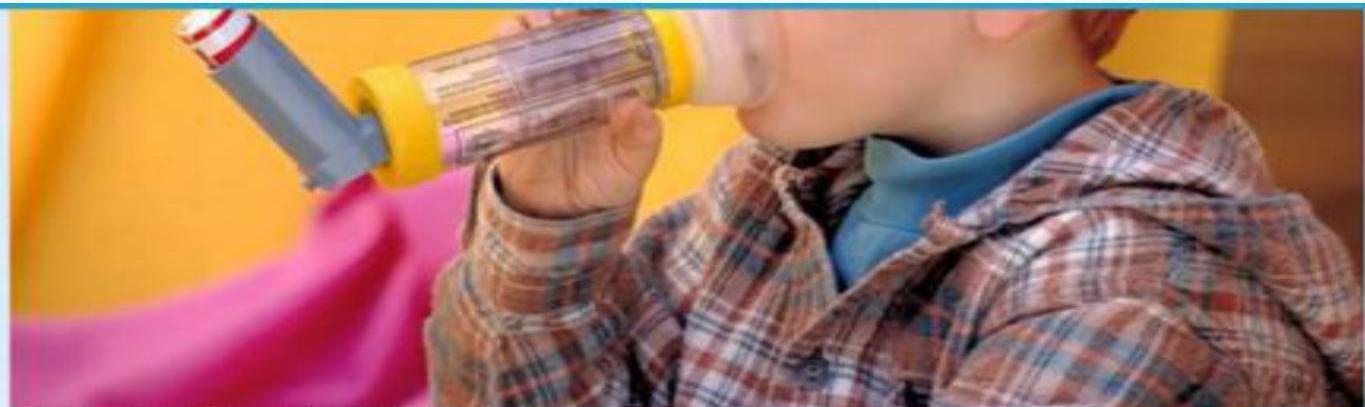
- 5 Year old child with bronchial asthma. vs 2 year old bronchial asthma
Name:
- Aerochamber spacer with mask, flow valve and MDI - Aerochamber Spacer with mask + Metered Dose Inhaler (MDI).
Age:
- With mask: 2-3 years
- With mouthpiece: 6-9 years
Counseling station: Convince mother to add ICS.+}+}
Indication:
- Bronchial asthma below 5 years
Advantages:
- More effective than MDI alone
- Slows down medicine delivered from metered-dose inhaler
- Medicine stays in spacer for child to breathe into lungs
- Without spacer, medicine sprays directly into mouth/throat, less reaches lungs
Medications used: Inhaler medications (e.g. Salbutamol).
- Bronchodilator
- Corticosteroid
Systemic Juvenile Rheumatoid Arthritis (Still’s Disease)



Keywords:
- Spiking fever
- Rash started in the trunk
- Growth affected (chronic condition)
Rash Type:
- Salmon-colored pink rash
- Fades with pressure
Diagnosis:
- Systemic juvenile rheumatoid arthritis (Still’s disease)
Juvenile Rheumatoid Arthritis (JRA)

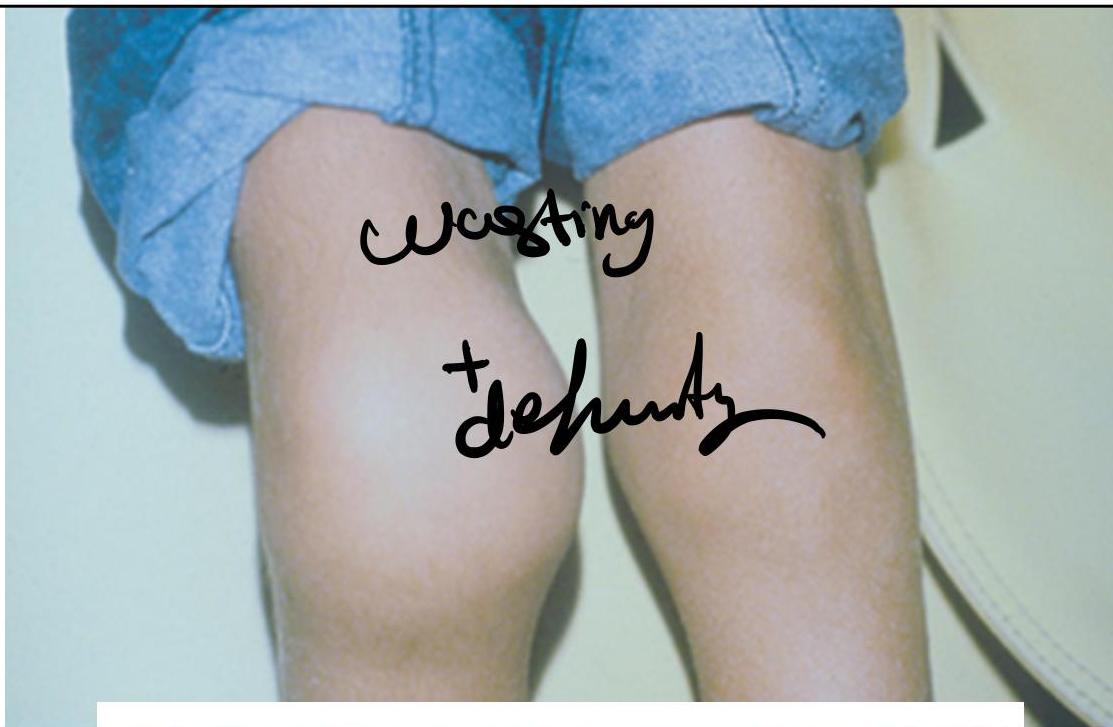

5 years old girl who has been limping with swelling of her right knee for several months, parents note that she cannot fully extend her right knee. She does not want to walk in the morning, but seems fine later in the morning and the rest of the day. Left knee swelling is noticed for last 3 weeks.
Chronic Arthropathy Findings:
- Knee swelling
- Wasting of thigh muscles (indicates chronic condition)
- No redness (indicates chronic vs acute)
Differential Diagnosis:
- Juvenile rheumatoid arthritis (JRA)
- SLE
- Hemarthrosis (in hemophilia)
- transient synovitis?septic arthritis?bruccelosis?
Scenario: 7-year-old child with limping
Abnormalities:
- Deformity in both knees
- Swelling in right knee
- Muscle wasting
Causes:
- JRA
- Hemarthrosis due to hemophilia
Management objectives:
- Promote normal growth and development.
- Factor 8 (for hemophilia)
- Aspiration and antibiotics (for septic arthritis)
if septic
If fever and red swelling knee, rule out first:
- Septic arthritis
Organism: if septic arthritis
- Staphylococcus
Acute Lymphoblastic Leukemia (ALL)
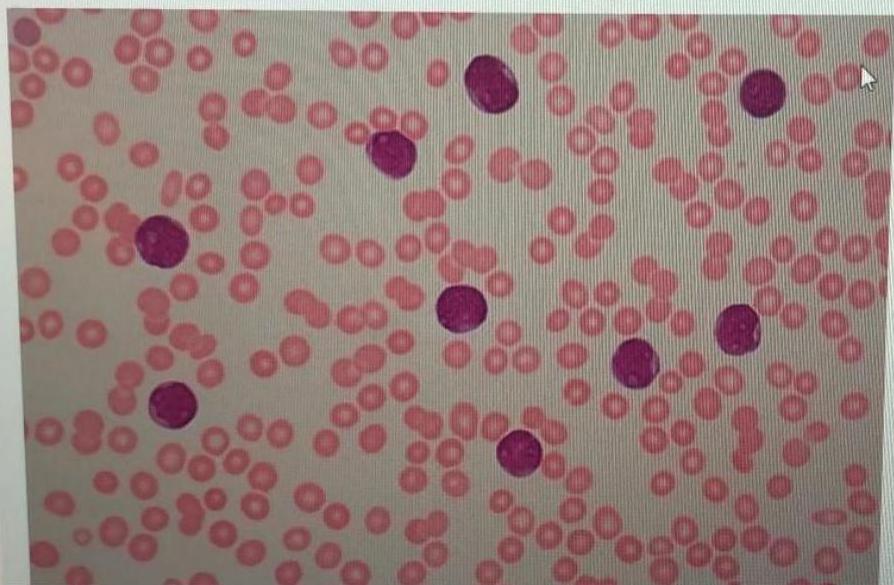
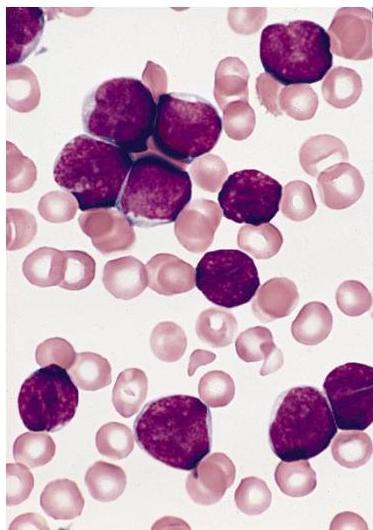
Scenario: 4 year old boy with fever, spontaneous nose bleeding, hepatosplenomegaly. Peripheral blood smear shown.
Abnormality in peripheral smear? Blast cells (lymphoblasts).
Diagnosis? Acute Lymphoblastic Leukemia (ALL).
Confirmatory Investigations:
- Bone marrow aspiration and biopsy
- Immunohistochemistry
Clinical signs?
- Anemia signs: dizziness, pallor
- Thrombocytopenia: petechiae, purpura
- Recurrent infections
- Bone pain
- Weight loss
- Hepatosplenomegaly
Bone Marrow:
- Single cell blast
Prognosis?
- Good prognosis if treated — children are cured in 90%
- Males treated for 3 years, females treated for 2 years
Treatment:
- Chemotherapy
- Supportive measures
History taking: complaint of pallor + rash.
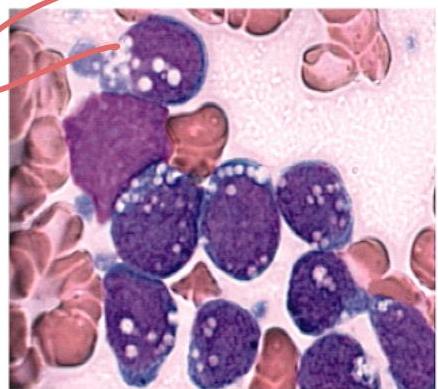
AML (Acute Myeloid Leukemia): Diagnosed via Bone Marrow aspirate/biopsy.
Cardiology
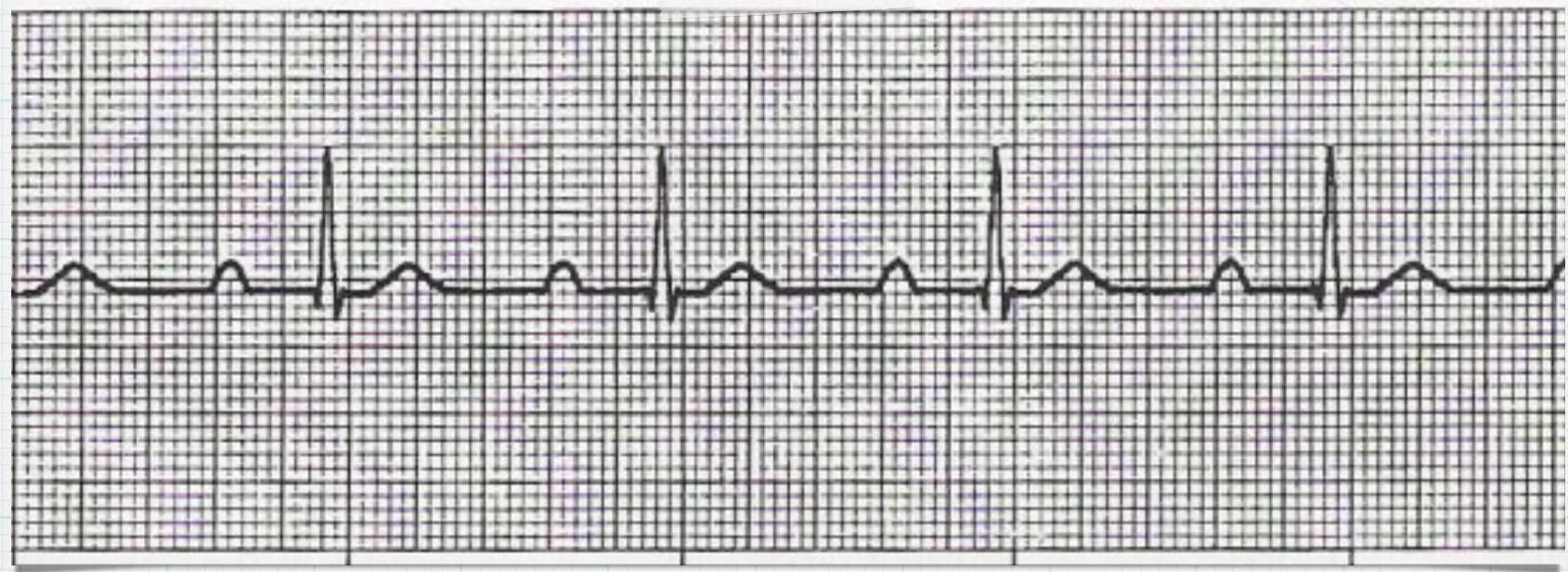
First Degree Heart Block /
ECG Findings:
- Fixed prolongation of PR interval - 1st degree AV block (prolonged PR interval).
Causes:
- Acute rheumatic fever.
- SLE
- Myocarditis
- Electrolyte disturbance
- CHD
Treatment:
- Treat underlying cause
Type II Second Degree AV Block /
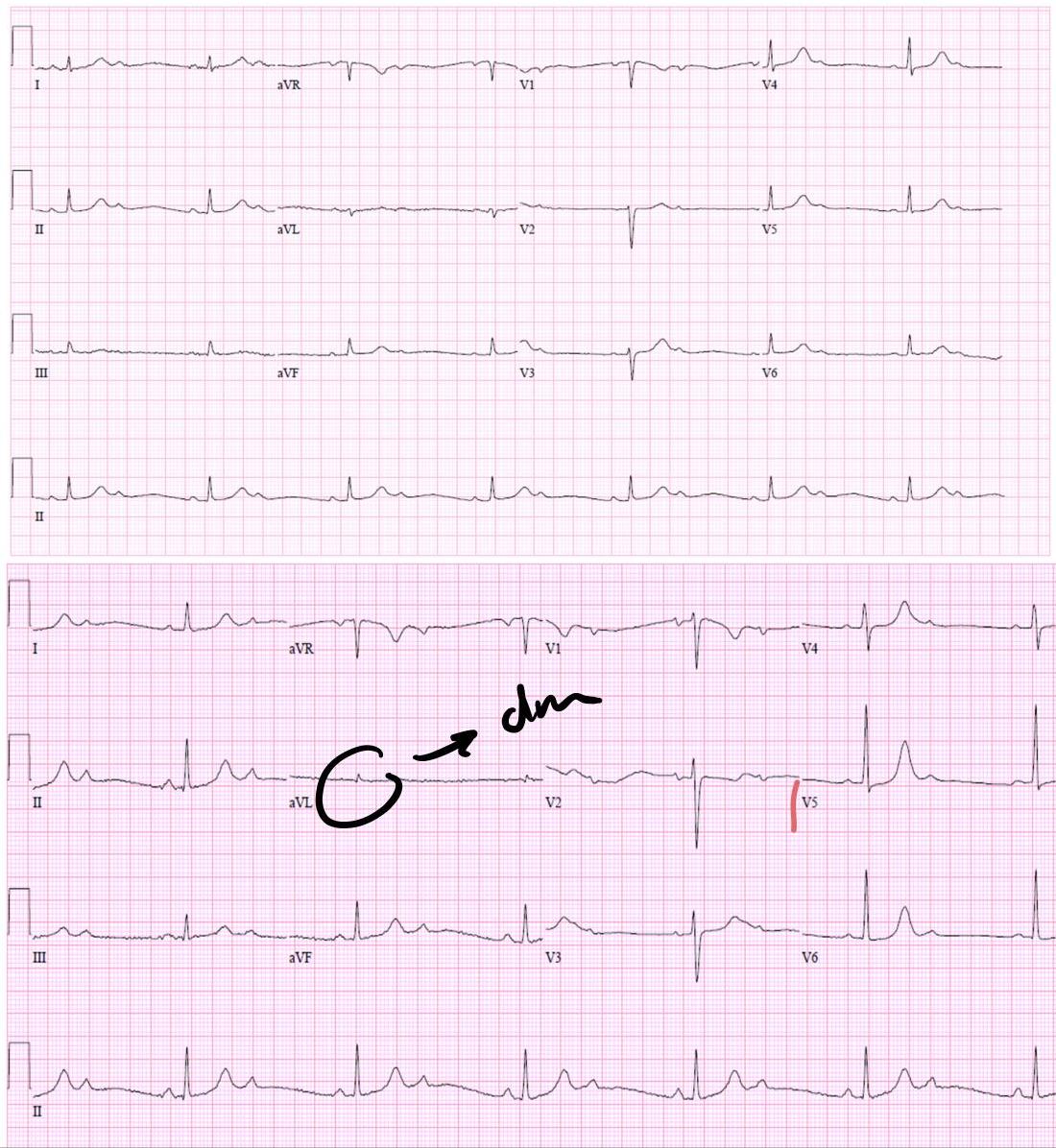
ECG Findings:
- No progressive prolongation
- Intermittent non-conducting P wave
Causes:
- Rheumatic fever
- SLE
- Myocarditis
- Electrolyte disturbance (hypokalemia, hypocalcemia)
- CHD
Treatment:
- Treat underlying cause
- Pacemaker
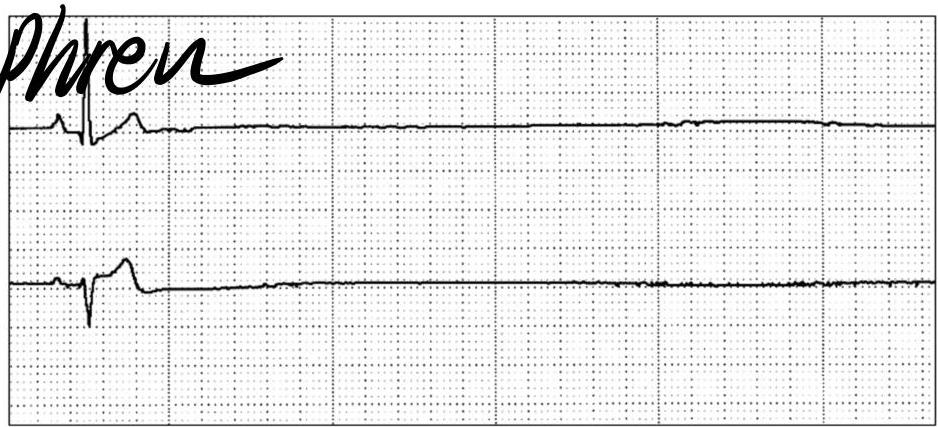
3rd Degree Heart Block /

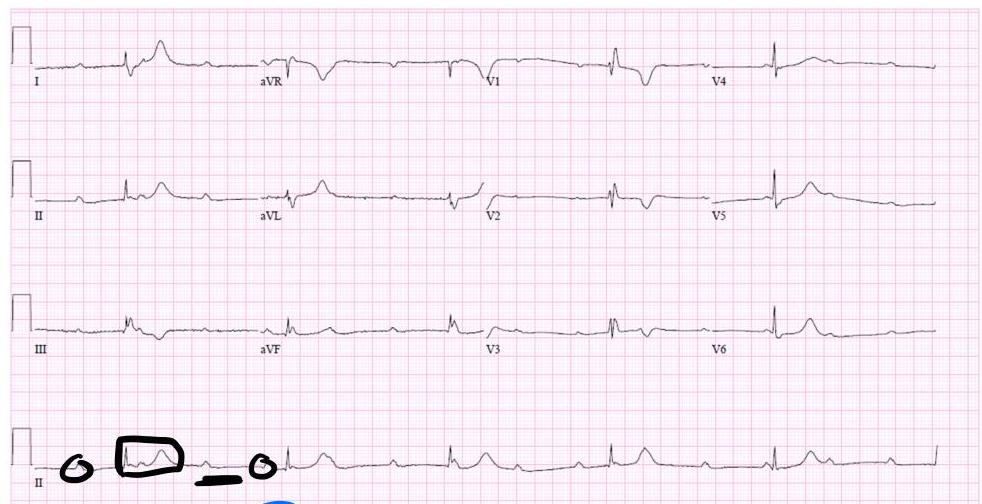
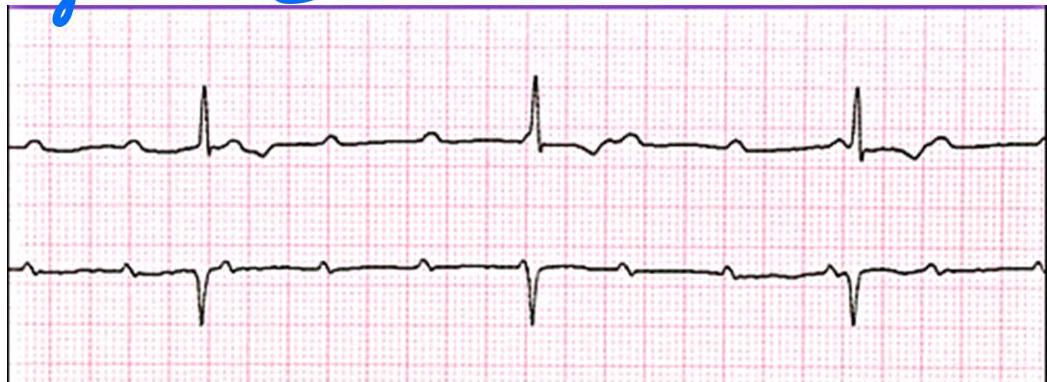
2 week old girl with abnormal cardiac rhythm - describe the ecg features? what is the diagnosis, write one possible cause?
Describe the ECG features?
- P waves more than QRS complexes (AV dissociation).
- Bradycardia.
- Irregular rhythm.
Diagnosis? 3rd degree (complete) heart block.
Causes?
- Neonatal lupus (maternal SLE) — most common congenital cause
- Rheumatic fever
- MI in adults
- BB, digoxin, and CCB
- Neonatal SLE → Can cause any type of heart block
Treatment:
- Pacemaker
An ECG showing bradycardia — “What are the causes?” and “What is the treatment?”
Acanthosis Nigricans




Causes/Conditions:
- Type 2 diabetes
- Cushing disease
- PCOS
- Pituitary disorders
- Hypothyroidism
- High doses of niacin
Investigations:
- Fasting blood sugar
- HgA1C
Insulin Types

Identify the type of insulin and its onset, duration, and peak — check insulin table.
Infant of Diabetic Mother

Scenario: Infant is Large for GA. Startled with jerking of upper limbs lasting 10 seconds at 4 hours of life. Apathy, poor feeding, weak cry. Delivered by elective C/S with normal Apgar scores.
Likely cause of symptoms? Hypoglycemia.
Likely cause of large size? Maternal diabetes.
Baby Shaken Syndrome
Scenario: 4-month girl presents to ED with recurrent vomiting, admitted, discharged stable, 5 days later presents with unresponsive episode, bulging fontanelles to PICU.
Findings:
- Subdural hemorrhage
Diagnsois?
- baby shaken syndrome
Complications:
- Cerebral edema
- Retinal hemorrhage Station recall: Brain MRI showing shaken baby syndrome.
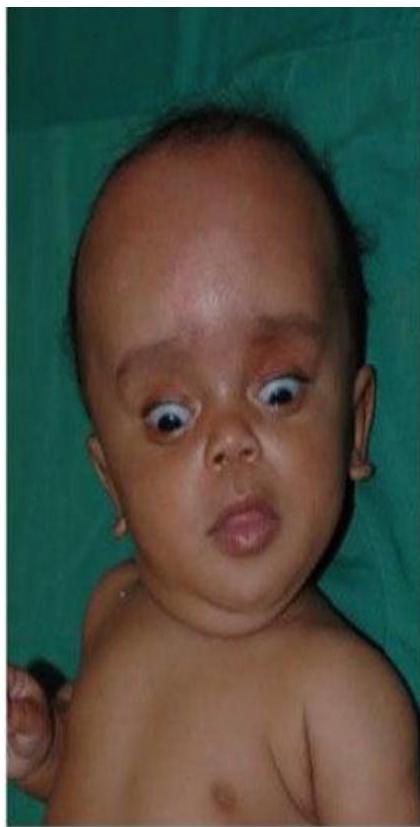
Spina Bifida / Myelomeningocele


Findings:
- Sunset eye
- Big head
- Dilated veins in head (sign of increased ICP)
Most common cause of hydrocephalus:
- Myelomeningocele
Next to examine:
- Back
- Check pulse and BP (increased ICP)
Treatment:
- Closure of myelomeningocele
- VP shunt
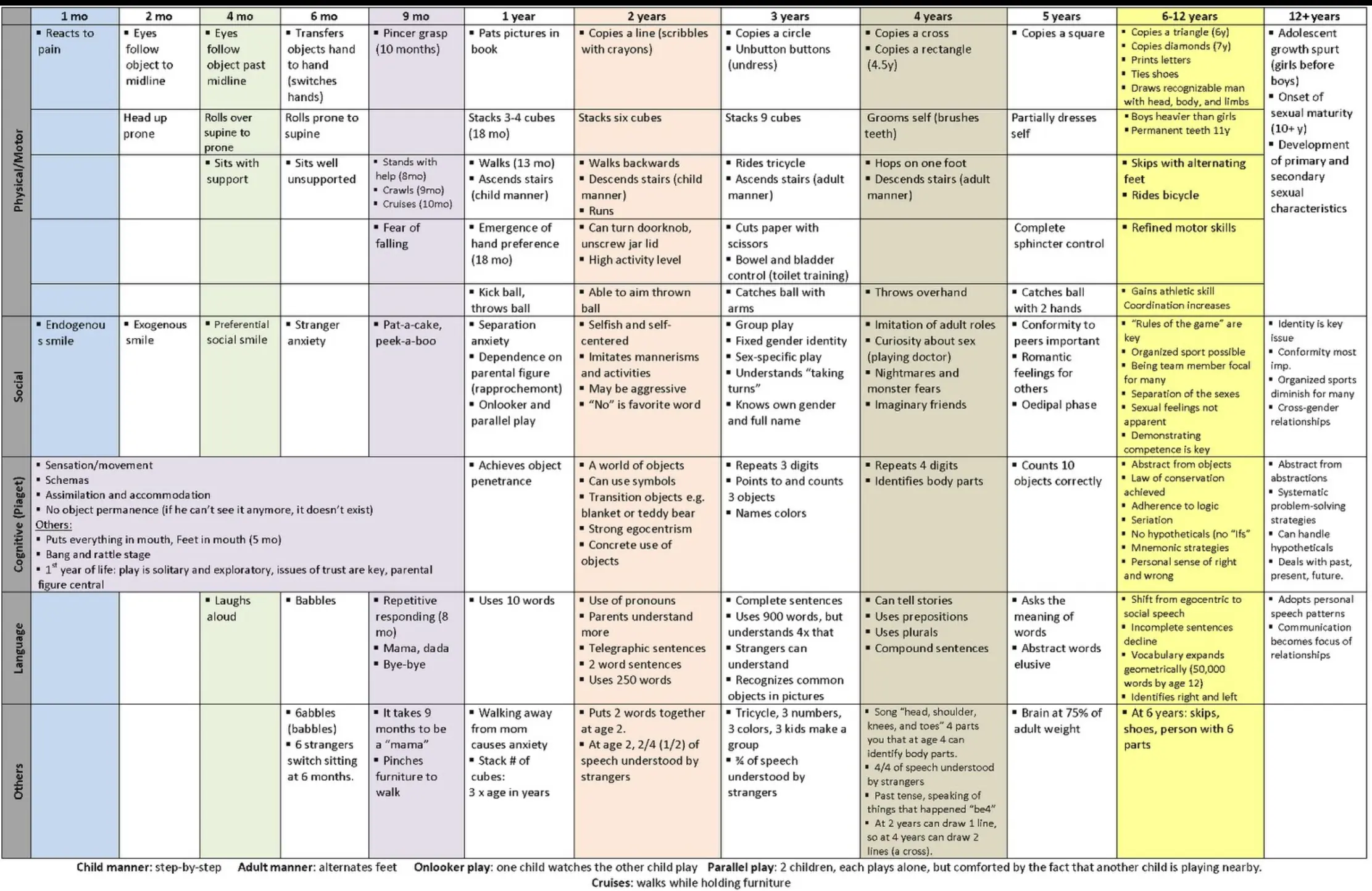 catch with arm 3 yrs, throw 1 yr
catch with arm 3 yrs, throw 1 yr
Turner Syndrome (45X0)
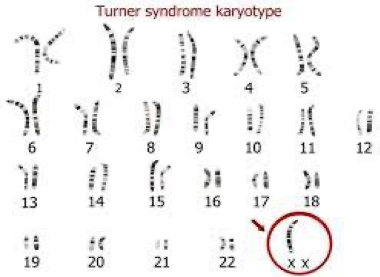
 webbed neck, edema foot at birth, everything widening.
webbed neck, edema foot at birth, everything widening.
Noonan Syndrome
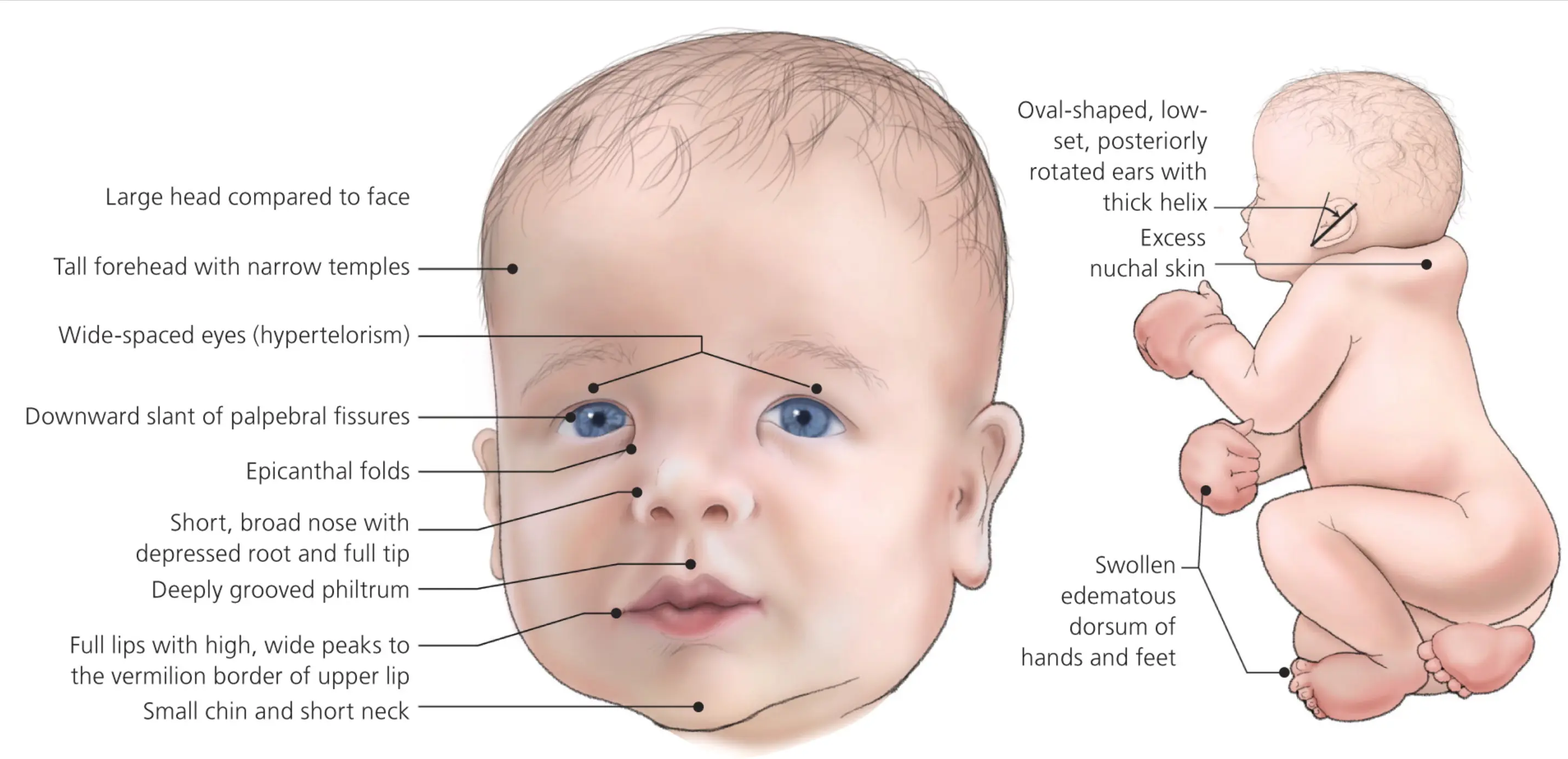
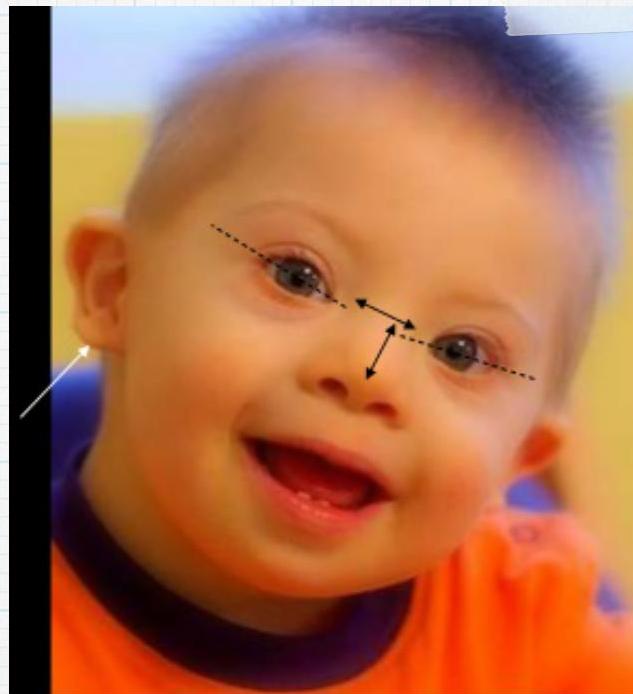
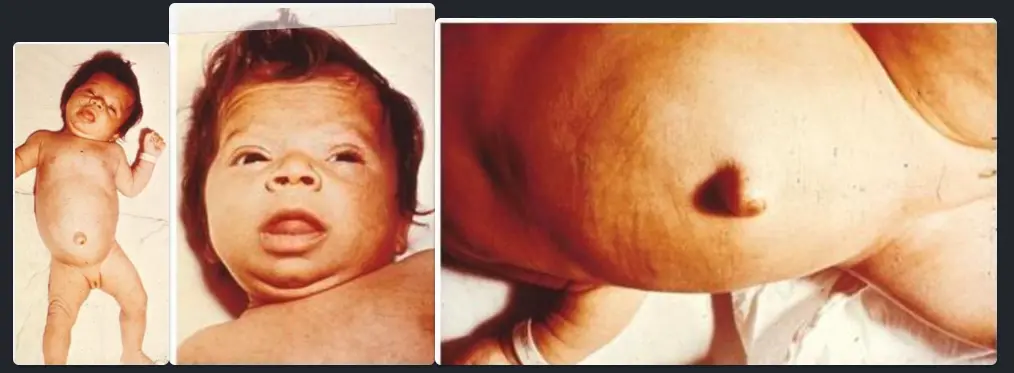
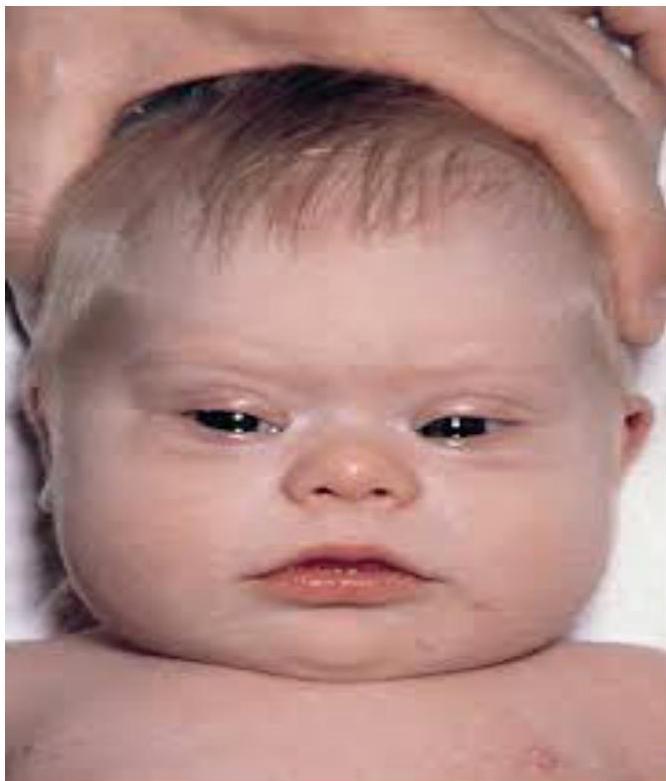
Down Syndrome (Trisomy 21)
Eight-year-old boy with dysmorphic features and learning disability. She was operated for congenital heart disease at infancy.
Diagnosis? Down Syndrome.
Most common cause? Trisomy 21 (meiotic non-disjunction).
Which investigation helps in assessing this patient?
- Thyroid hormone levels
Describe facial features? Round face. Flat nasal bridge .-. Small mouth. protruding tongue - small ear -upslanted palpebral fissure…
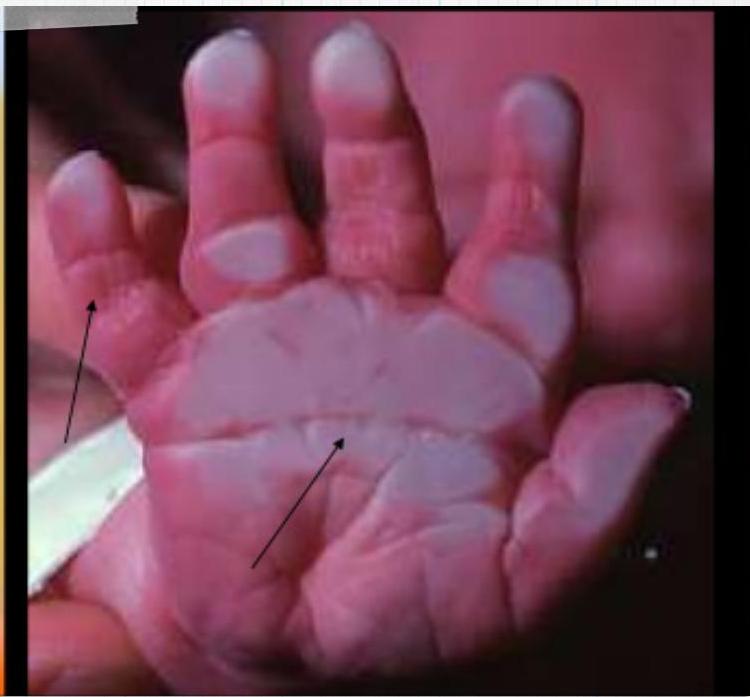
What is the most common Musculoskeletal Problems? Atlantoaxial instability
What are the long-term complications associated with Down Syndrome? Leukemia, hypothyroidism, and obesity.
Patau Syndrome (Trisomy 13)
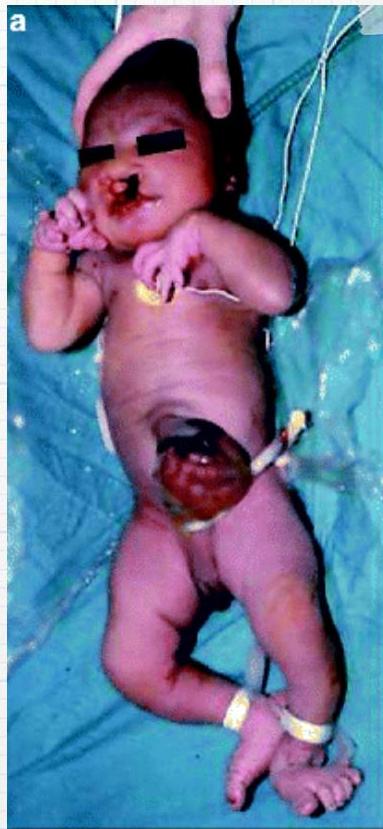
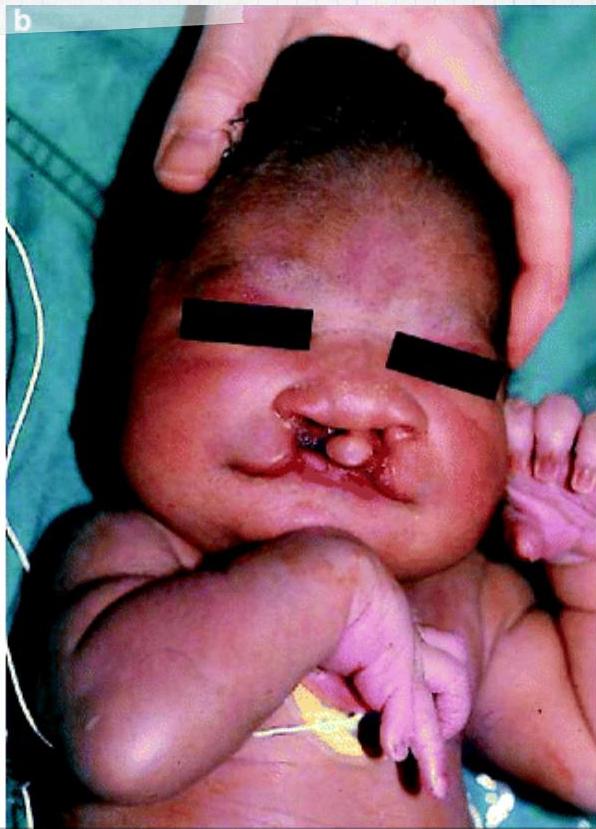
Condition? Patau Syndrome.
Cause? Trisomy 13.
Autosomal Dominant Inheritance
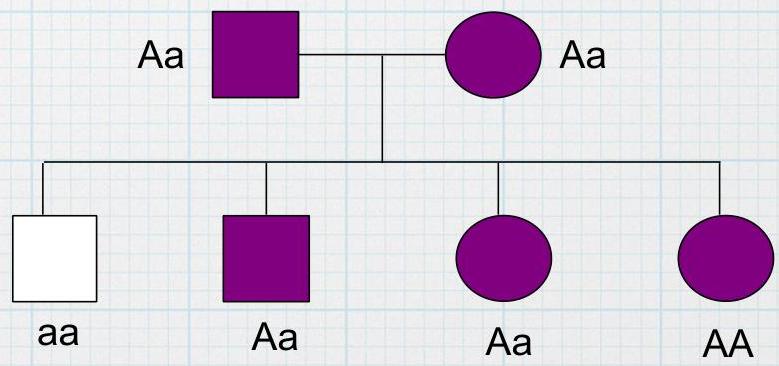
Mode of inheritance? Autosomal Dominant.
Example disease? Huntington Disease. Marfan syndrome, Osteogenic imperfecta, Porphyria, Achondroplasia
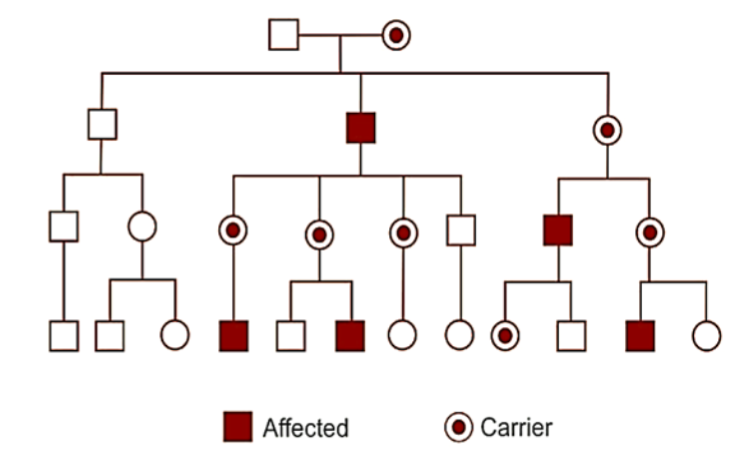
Case
1. Name the mode of inheritance? X-linked Recessive 2.What are the features seen on a family tree? males affected exclusively, the gene alteration is transmitted from female carriers to sons, affected males cannot transmit the condition to their sons. 3. Mention 1 example ? Hemophilia, Duchenne’smuscular dystrophy, G6PD deficiency, Albinism
 A 18 months old boy manifests poor appetite, diarrhea, and irritability.
He had been well until 9 month of age. Thereafter, he was weaned from
breast milk to regular foods. His growth curve is flattening. Patient with type 1 diabetes on insulin, experiencing frequent hypoglycemia and abdominal distension.
A 18 months old boy manifests poor appetite, diarrhea, and irritability.
He had been well until 9 month of age. Thereafter, he was weaned from
breast milk to regular foods. His growth curve is flattening. Patient with type 1 diabetes on insulin, experiencing frequent hypoglycemia and abdominal distension.
- What is your diagnosis?
- Celiac disease
- How to diagnose this condition?
Antibody titer (deamidated gliadin peptide and transglutaminase).
- Tissue transglutaminase - Ig A
- Duodenal Biopsy
Metabolic
Galactosemia

Scenario: 3 month old with hepatosplenomegaly, hypoglycemia, decreased tone and muscle strength. Older brother on special milk formula.
Clinical sign? Bilateral cataracts.
Diagnosis? Galactosemia.
Leukocoria (Retinoblastoma)
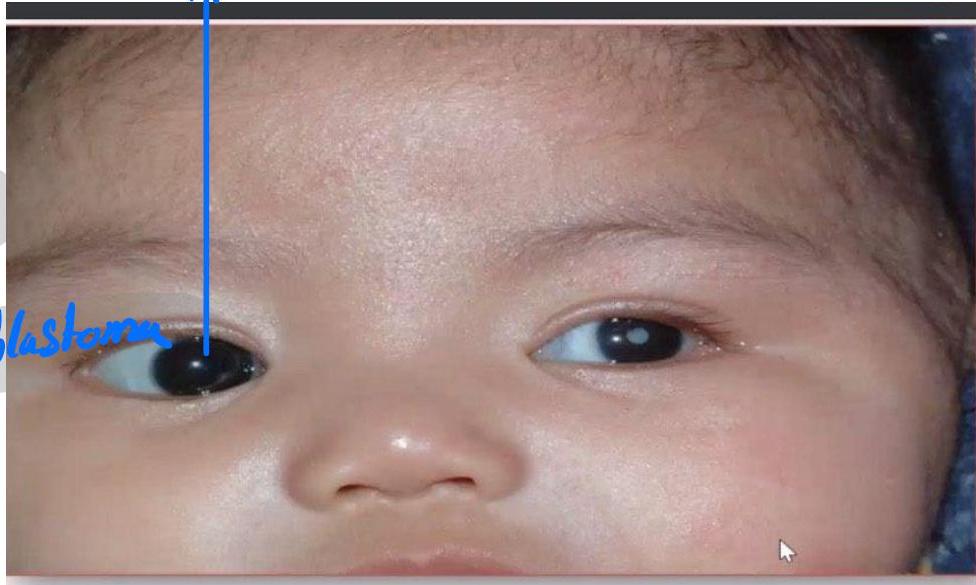
Finding:
- White reflex in the pupil (leukocoria)
- Cat’s eye reflex
Diagnosis:
- Retinoblastoma
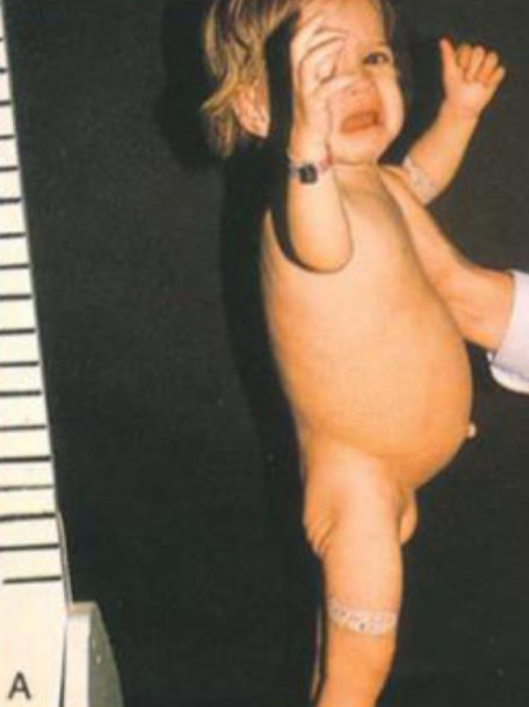
Hypoglycemia, hyperlipemia, abdominal distention and pain, normal LFT.
A) what is your diagnosis? B) what lab investigations will you order? We answered kwashiorkor or celiac disease.
Picture of a child, standing, sad, abdomen distended, thin limbs
Neonatal Jaundice Grading
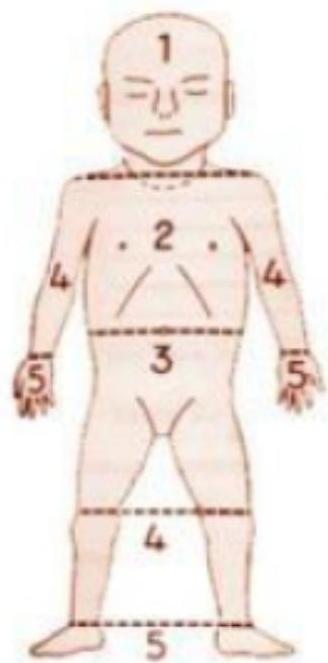


| Grade | Extent of Jaundice |
|---|---|
| 0 | None |
| 1 | Face and neck only |
| 2 | Chest and back |
| 3 | Abdomen below umbilicus to knees |
| 4 | Arms and legs below knees |
| 5 | Hands and Feet |
Grade in the neonate shown? Grade 5.
Management? Check TSB and choose accordingly: exchange transfusion or phototherapy.
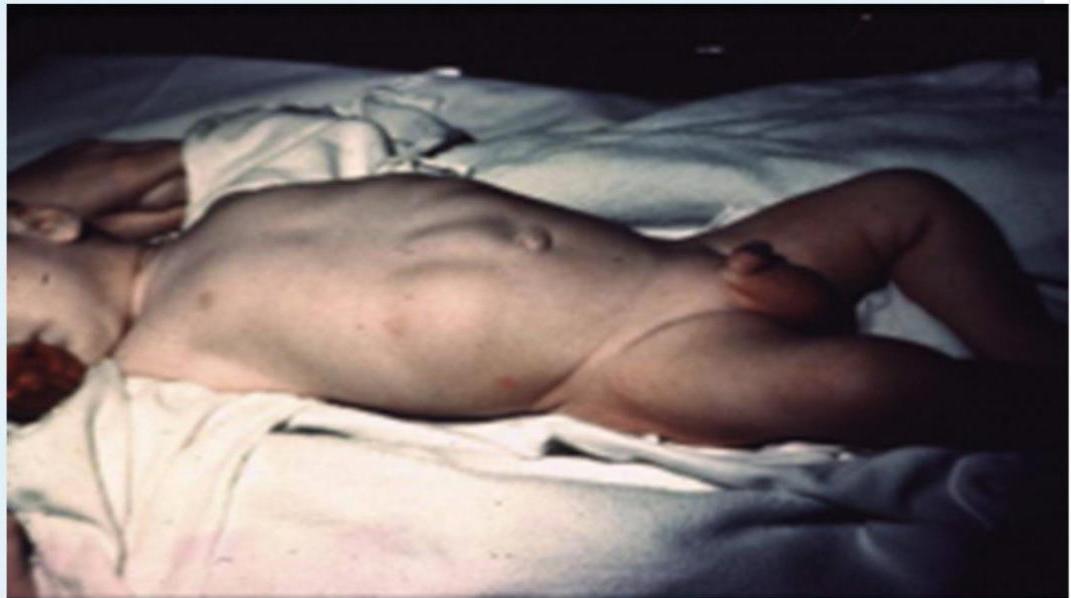
Marasmus
Infant was delivered by c/s due to fetal distress at 40 weeks gestation. His birth weight was 2.1 kg. He developed severe, difficult to control hypoglycemia. What is the diagnosis?

Questions
- Diagnosis?
- Marasmus
- Describe?
- Wasting, wild eyes, abdominal distention, senile monkey face
- Cause?
- Caused by malnutrition, Large VSD
Roseola Infantum

Scenario: Infant with high fever (39.4-40.6°C) lasting 2 days. After fever ended, rosy-pink rash appeared mostly on trunk, neck, and arms. Rash not itchy, lasted 2 days.
Diagnosis:
- Roseola infantum
Group B Streptococcus (GBS)

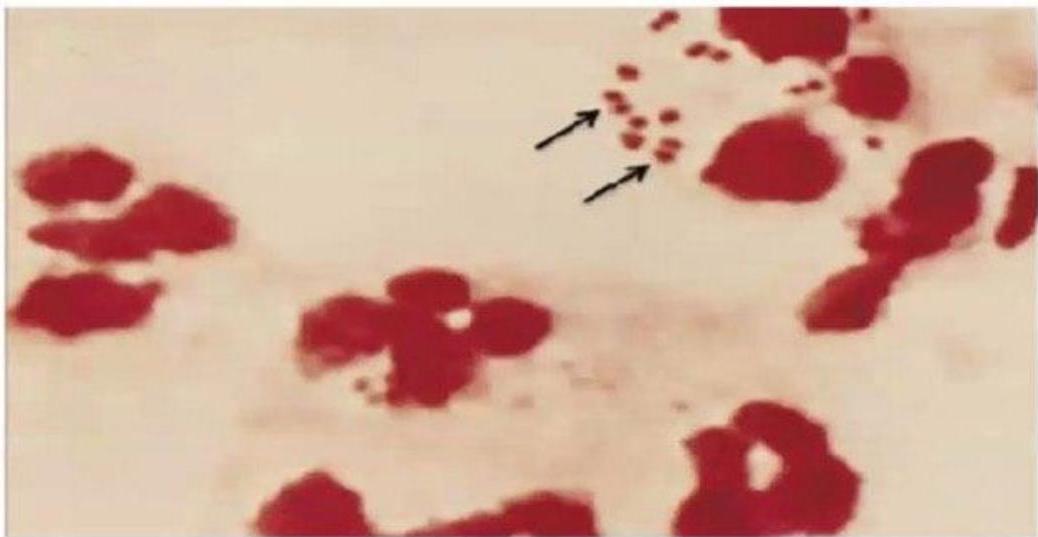
- Baby with severe resp distress after birth. Blood cluture shows gram +ve cocci
- Cause ?
- GBS
- 2nd picture shows ?
- Gram negative N.meningitides
Meningococcemia
,Parents bring their child in for evaluation due to acute development of high fever, malaise and lethargy. On exam, the patient is mottled with poor perfusion, tachycardic, and has developed a new rash
 !
!
Findings:
- Purpura, petechiae, ecchymosis (non-blanching)
- Mottled appearance
- Poor perfusion
- Tachycardia
Blood Culture:
- Gram negative N. meningitidis
Diagnosis:
- Meningococcemia
Scenario: Baby with severe respiratory distress after birth
Blood Culture:
- Gram positive cocci
Cause:
- GBS
Henoch-Schönlein Purpura (HSP)







Scenario: 11-year-old female with abdominal pain, joint pain, new skin rash. Stool positive for occult blood. - 10 year old boy with purpuric skin rash and adbdominal pain what is most likely diagnosis? mention 2 complication - 8-year-old boy with joint and abdominal pain.
Rash Description:
- Purpuric rash at buttock and extensor arms
- Palpable purpura
Diagnosis:
- Henoch-Schönlein purpura (HSP)
- Part of IgA nephropathy
Complications:
- Renal involvement (hematuria, proteinuria, chronic kidney disease, hypertension)
- Intussusception
- Encephalopathy
- Massive GI bleeding
- Acute glomerular lesion
- In boys: scrotal edema and testicular torsion
Kawasaki Disease


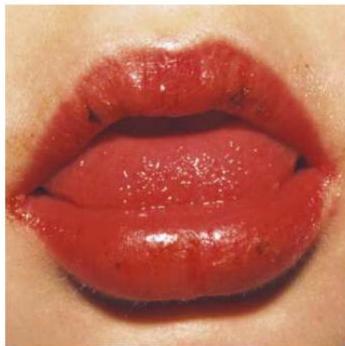






Physical Findings:
- Strawberry tongue
- Bilateral conjunctival injection
- Mucosal changes
- Cervical lymphadenopathy
Complication:
- Coronary artery aneurysm
Differentiation from Hand-Foot-Mouth Disease:
- No strawberry tongue in HFMD
- Fever >5 days in Kawasaki vs 2 days in HFMD
Erythema Marginatum

Rash? Erythema Marginatum.
Associated condition? Acute rheumatic fever.
Congenital Hypothyroidism
Diagnosis? Congenital Hypothyroidism.
Investigations? TSH, free or total T4.
Neonatal Lupus

Scenario: 3-month-old anti-Ro/SSA positive male infant OR 2-month-old anti-Ro/SSA positive male infant - Scenario: Neonate with skin rash and low pH. Mother has facial rash, occasionally pruritic.
Findings:
- Discoid rash
- Photosensitivity
- Skin rash and low pH
- Mother with facial rash occasionally pruritic
Diagnosis:
- Neonatal SLE / Neonatal lupus / Neonatal lupus erythematosus.
Other Manifestations:
- Complete heart block
- Hepatomegaly (hepatitis)
- Anemia
- Thrombocytopenia (bruise)
- Oral ulcer
- Arthritis
Cardiac Complication:
- Heart block
| Condition | Description |
|---|---|
| TGA (Transposition of Great Arteries) | Egg on side, generalized cardiomegaly, narrow mediastinum |
| VSD/AVSD | Cardiomegaly, increased pulmonary vascular markings (plethoric lung fields) |
| Ebstein Anomaly | Marked cardiomegaly extends wall to wall (Box Shape) |
| Tetralogy of Fallot | Boot shape heart with upward cardiac apex (RVH), concave PA segment, decreased pulmonary vascular markings |
| Total Anomalous Pulmonary Venous Drainage | Snowman or figure of 8 - dilated vertical vein on left + brachiocephalic vein on top + SVC on right form the head; enlarged atrium forms the body |
| Heart Failure | Nonspecific cardiomegaly |
TGA:

- Egg on string appearance - EGG ON SIDE, generalized cardiomegaly, Narrow mediastinum Description: Knee chest position (Squating position) to treat the episodes of TOF
Squatting
- Common with unrepaired TOF
- Increases oxygen saturations
- Angulation and kinking of femoral arteries with increased SVR, decreasing the R→L shunt

Snowman Sign (TAPVD):
 snowman or figure of 8 Dilated vertical vein on the left and bracocephalic vein on top + superior vena cava on the right form the head of snowman, the body of snowman is formed by the enlarged atrium
snowman or figure of 8 Dilated vertical vein on the left and bracocephalic vein on top + superior vena cava on the right form the head of snowman, the body of snowman is formed by the enlarged atrium
Dx: Total Anomalous Pulmonary venous Drainage
Ebstein Anomaly:
 Description: marked cardiomegaly extend from wall to wall (Box Shape)
Description: marked cardiomegaly extend from wall to wall (Box Shape)
Dx: Ebstein Anomaly
Tetralogy of Fallot:
 Description: Boot shape heart with upward cardiac apex due to Right ventricular hypertrophy and concave pulmonary artery segment and decrease pulmonary vascular marking at peripheral lung felid.
Description: Boot shape heart with upward cardiac apex due to Right ventricular hypertrophy and concave pulmonary artery segment and decrease pulmonary vascular marking at peripheral lung felid.
Dx: Tetralogy of Fallot
VSD/AVSD:
 Description: cardiomegaly, increase pulmonary vascular markings (plethoric lung fields)
Description: cardiomegaly, increase pulmonary vascular markings (plethoric lung fields)
DDx : VSD, AVSD
Cardiomegaly (Heart Failure): (nonspecific)
Heart Failure with Pulmonary Edema:
Scenario: 3-month-old with heart failure, cyanotic and cardiac murmur
Findings:
- Small heart
- Pulmonary edema
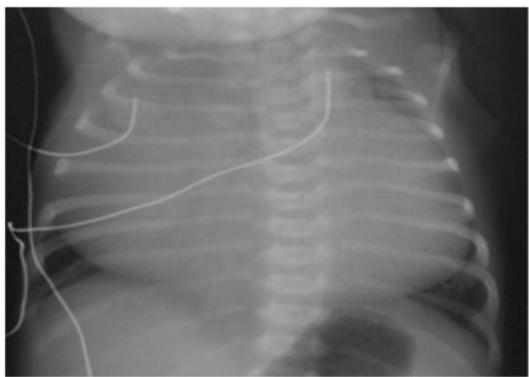
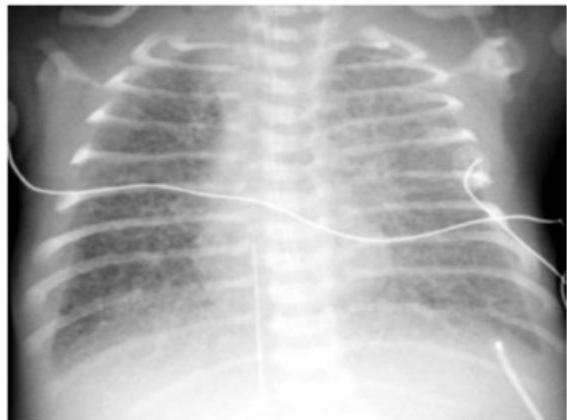
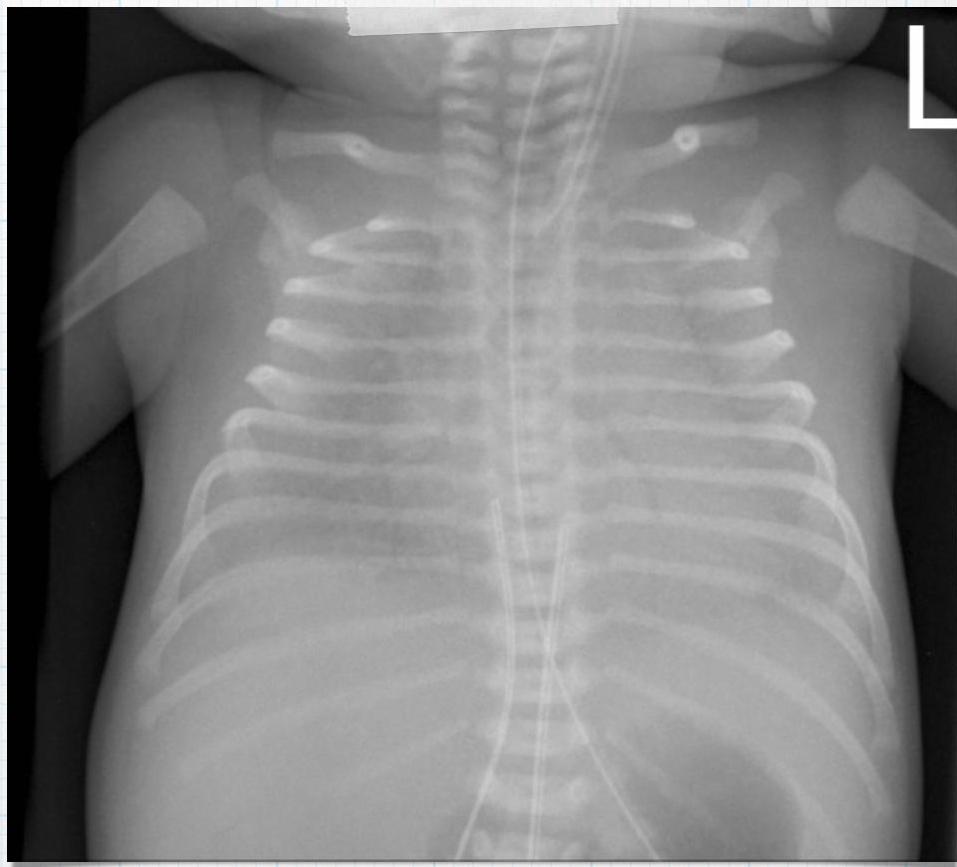
Preterm Infant with Respiratory Distress
- Preterm 29 weeks gestation C/S delivery showed severe respiratory distress soon after birth - RDS
- Air bronchograms

-
There is a homogeneous opacification of both lungs with white-out lungs - (1 .field (grounds glass appearance) and air bronchogram bilaterally
-
.The diagnosis is Acute Respiratory Distress Syndrome (ARDS) - (2
-
**;The most common causes of ARDS are **
- .A- Bacterial or viral pneumonia
- .B- Sepsis
- .C- Major trauma
- .D- Major surgery
- .E- Massive aspiration pneumonitis
- .F- Severe poisoning and intoxication
- .G- Severe envenomation (snake bite and scorpion sting)
- .H- Severe and prolonged hypoxia
- .I- Massive blood transfusions Preterm 29-weeks gestation C/S delivery showed severe respiratory distress soon after birth. This chest x-ray was taken at the age of 6 hours.
- Q1: Write 2 abnormalities in the X-Ray?
- Q2: What is the likely diagnosis?
- Q3: Write 2 management steps.
Answers:
- Q1: Ground glass appearance, wide intercostal space.
- Q3: Mechanical ventilation, give Surfactant for lungs maturation.
What are the possible diagnoses? Congenital pneumonia or respiratory distress.
Hand-Foot-Mouth Disease





Scenario: A 2 years old child presented with two days history of fever, malaise, abdominal pain. Mother brought him to medical attention today because of the appearance of this rash.
Diagnosis:
- Hand-foot-mouth disease
Cause:
- Coxsackievirus A16
Why not Kawasaki:
- No strawberry tongue
- Fever only 2 days (Kawasaki >5 days)
Gastroenterology
Pyloric Stenosis

Scenario: weeks old male infant presented with vomiting after feeding progressively worse, non bilious, no fever, no diarrhea, less active than before
Clinical Findings:
- Signs of dehydration. Z
- Abdominal distension
- Visible peristalsis
- Inverted umbilicus
- Olive sign in epigastrium
Diagnosis:
- Infantile hypertrophic pyloric stenosis / Congenital pyloric stenosis
Complications:
- Hypochloremic hypokalemic metabolic alkalosis
- Severe dehydration
Mode of Inheritance:
- Autosomal Dominant
Management:
- Fluid resuscitation
- Potassium chloride and electrolyte correction
- Surgical treatment (pyloromyotomy)
GERD — pH Probe
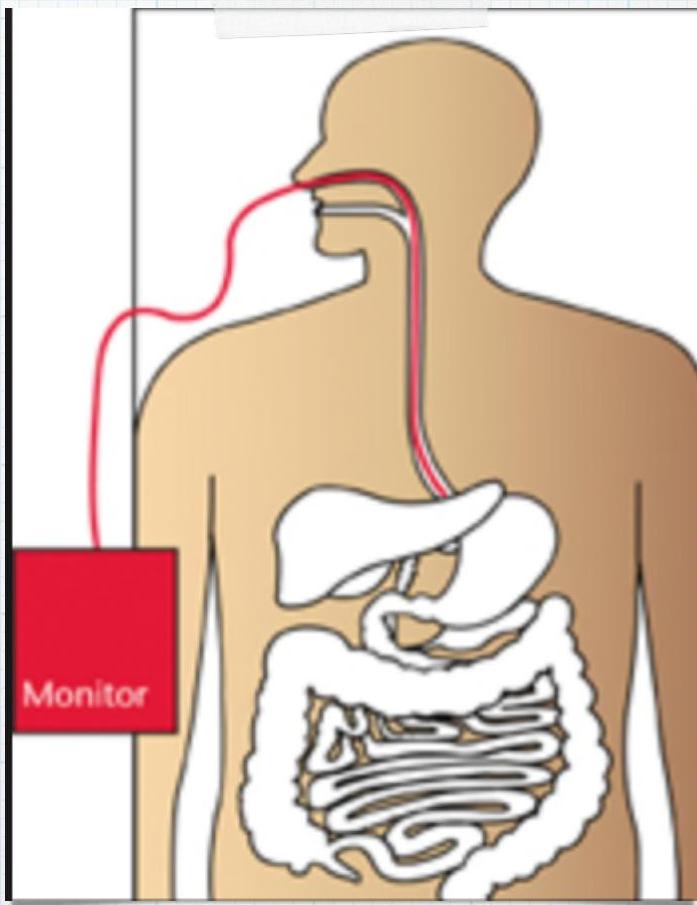

Procedure? pH Probe.
Diagnostic for? GERD.
Corrosive Poisoning / Esophageal Stricture
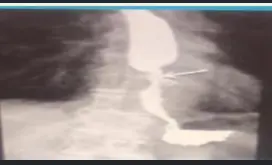
Scenario: 3 year old poisoned at home with severe acute injury and long-term complications.
Poison type? Corrosive (bleach, disinfectants, detergents, cleaning agents).
Barium swallow finding? Esophageal stricture.
Corrosive Poisoning


Scenario: Toddler reached chemicals area OR 15-month-old with corrosive ingestion
Findings:
- Drooling saliva
- Lip ulcer
- Redness in right eye
- NGT in place
Question: What type of poisoning?
- Corrosive poisoning
Contraindicated Measures:
- Induction of emesis
- Gastric lavage
- Administration of activated charcoal
- Neutralizing substances with weak acid/base
Management:
- Endoscopy
Long-term Complication:
- Esophageal stricture
Respiratory Distress Syndrome (Premature Neonate)
X-ray? Ground glass appearance of the lungs with air bronchogram.
Diagnosis? Respiratory Distress Syndrome.
Neonatology
Neurology
Cerebral Palsy

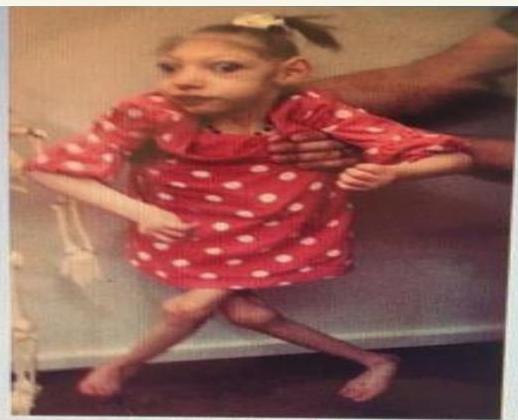
Diagnosis? Severe spastic quadriplegic cerebral palsy and microcephaly.
Features?
- Microcephaly
- Limbs scissoring
- Fisting (hands tightly clenched with thumb tucked inside fist)
Axial Hypotonia
2 month old baby is examined in the clinic Tests:
- Ventral suspension test (inverted U shape)
- Pull to sit test (head lag)
Findings:
- U-shaped on ventral suspension
- Floppy child
- Head lag on pull to sit test
Causes:
- Down syndrome
- Cerebral palsy
- Muscular dystrophies
How do you expect the power?
- Reduced.
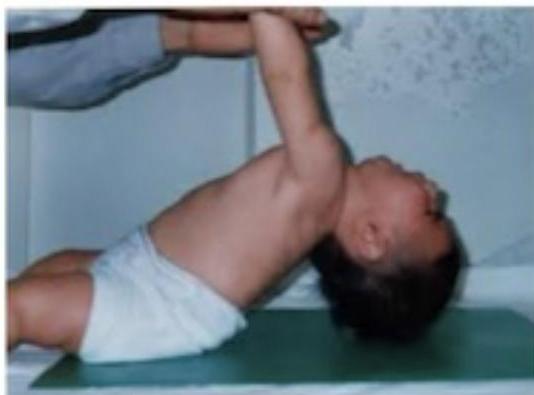
 U shaped
U shaped

Skin Lesions from Child Abuse
Sock-glove burn: & Cigarette Burns

Pattern:
- Sock-glove like burns
- Multiple rounded scars (cautery marks)
Seen when:
- Feet or hands held in water
- Line of demarcation suggests non-accidental injury
Diagnosis:
- Child abuse
Immersion Burns

Scenario: 2 year old with symmetrical burns on both hands and feet, brought to ER.
Burn pattern? Thermal injuries with stocking-and-glove distribution (immersion injuries).
Accidental? FALSE — this is child abuse.
Wilson Disease
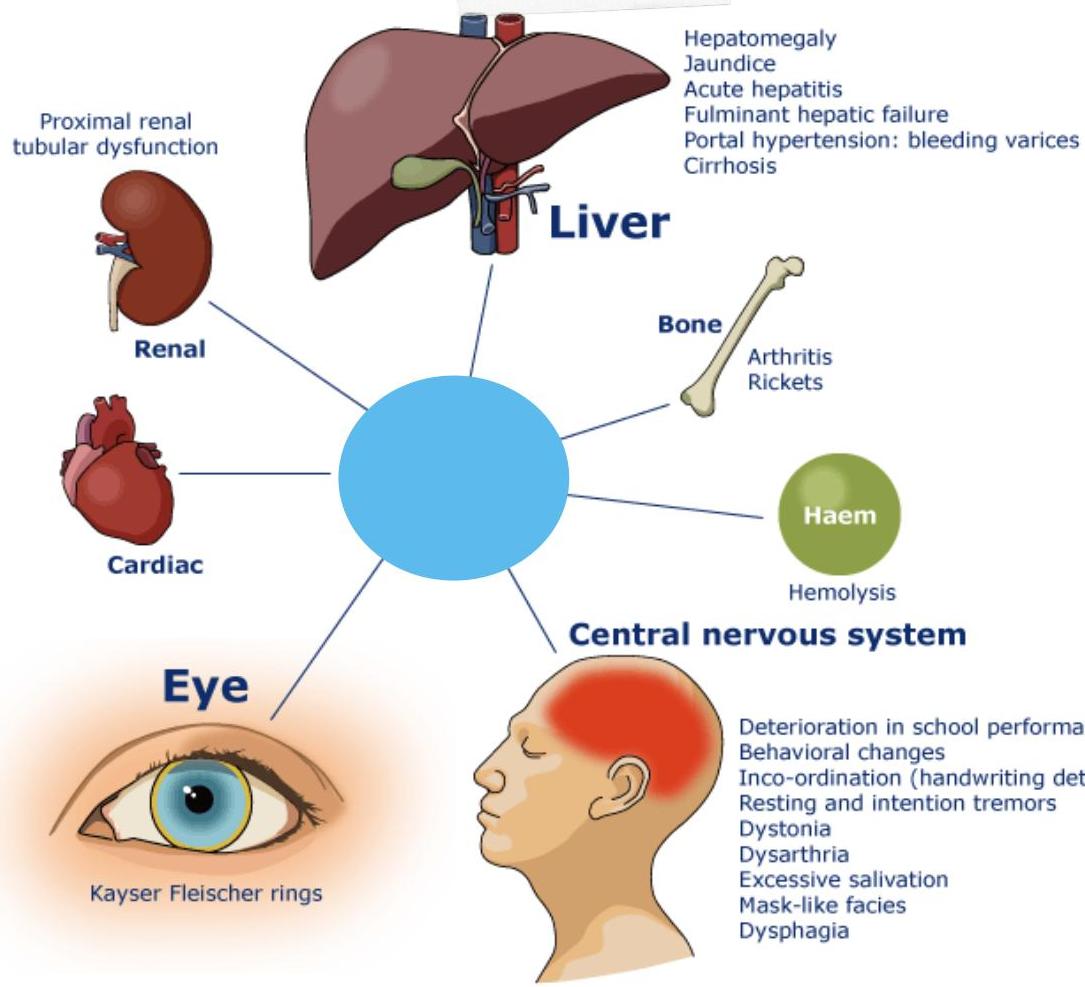
Diagnosis? Wilson Disease.
Management? D-penicillamine (copper chelation), zinc supplementation, low copper diet.