Acute Kidney Injury: Definition and Clinical Features
Definition
Acute kidney injury (AKI) is a sudden, potentially reversible decline in renal function characterized by:
- Oliguria: <0.5 ml/kg per hour
- Biochemical: Elevated blood urea nitrogen (BUN) and serum creatinine
- Homeostasis: Disturbances in fluid, electrolyte, and acid-base balance
Clinical Features
The severity and presentation of AKI can vary widely depending on the underlying cause, patient age, and comorbidities. Early recognition is critical for appropriate management.
- Fluid Balance: Oliguria/anuria, edema
- Electrolytes: Hyperkalemia, hyponatremia
- Acid-Base: Metabolic acidosis
- Cardiovascular: Hypertension
- Neurological: Lethargy, confusion
- GI: Nausea, vomiting, decreased appetite
Visual Summary of AKI Causes
 NORMAL
NORMAL
 PRERENAL: Decreased blood flow to kidneys (e.g., hemorrhage, hypovolemia, heart failure).
PRERENAL: Decreased blood flow to kidneys (e.g., hemorrhage, hypovolemia, heart failure).
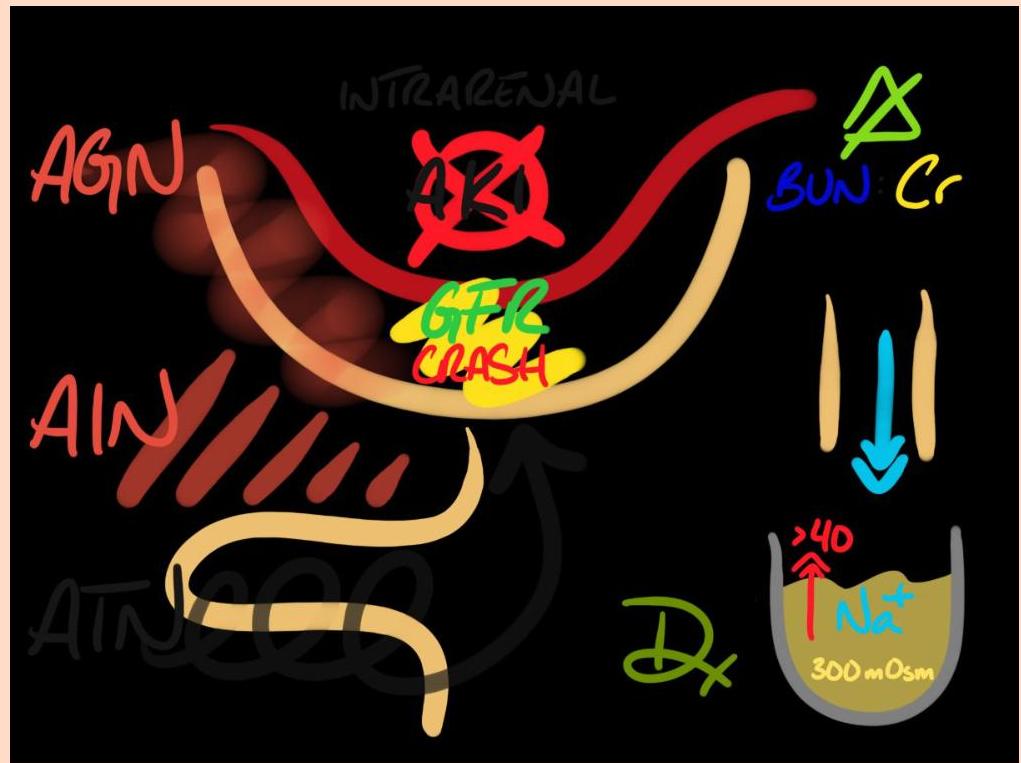
 INTRINSIC: Disease within kidney (e.g., acute tubular necrosis, inflammation, toxicity).
INTRINSIC: Disease within kidney (e.g., acute tubular necrosis, inflammation, toxicity).
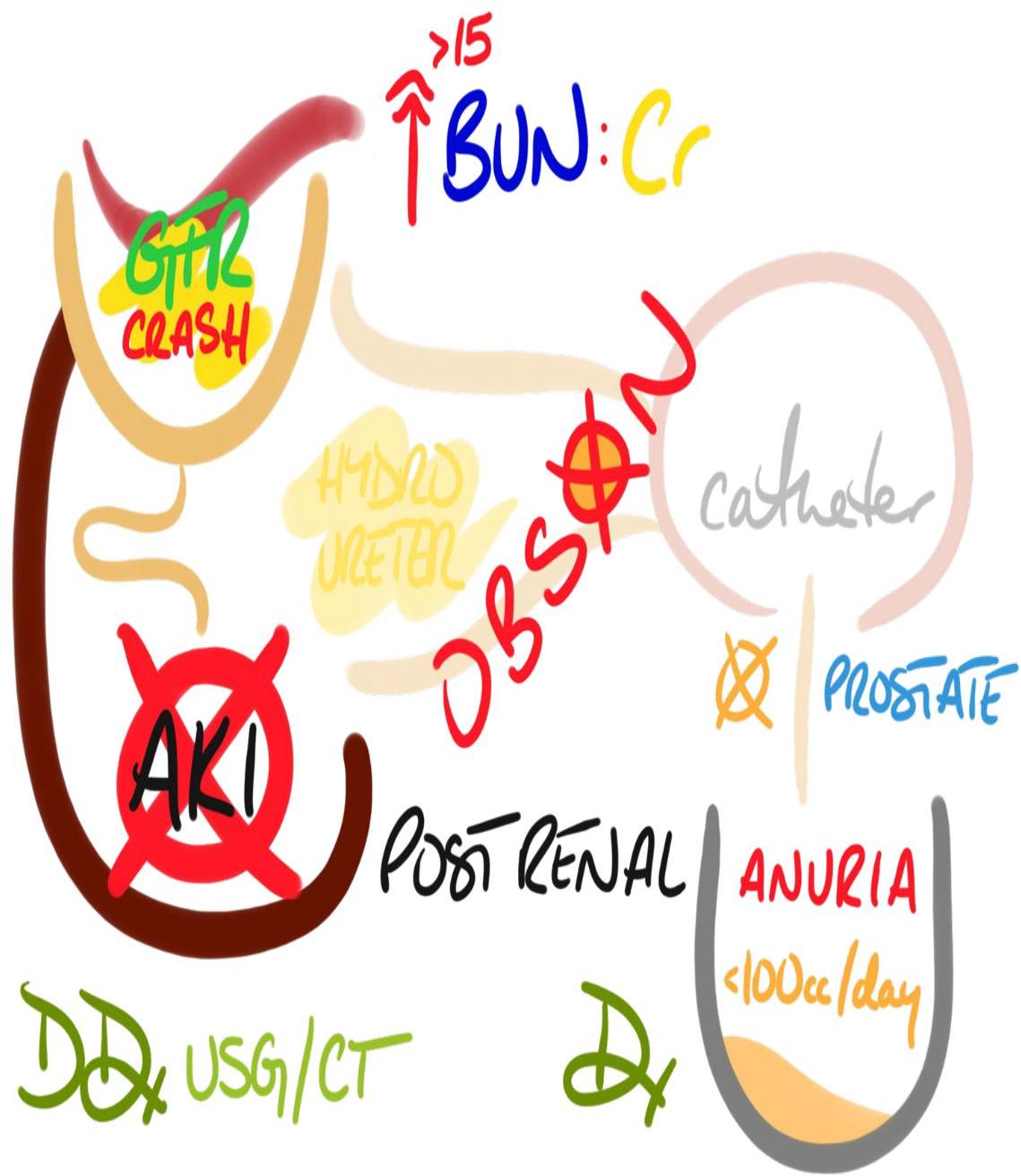
 POST-RENAL: Urinary outflow obstruction (e.g., Kidney stones, BPH, tumors, surgery).
POST-RENAL: Urinary outflow obstruction (e.g., Kidney stones, BPH, tumors, surgery).
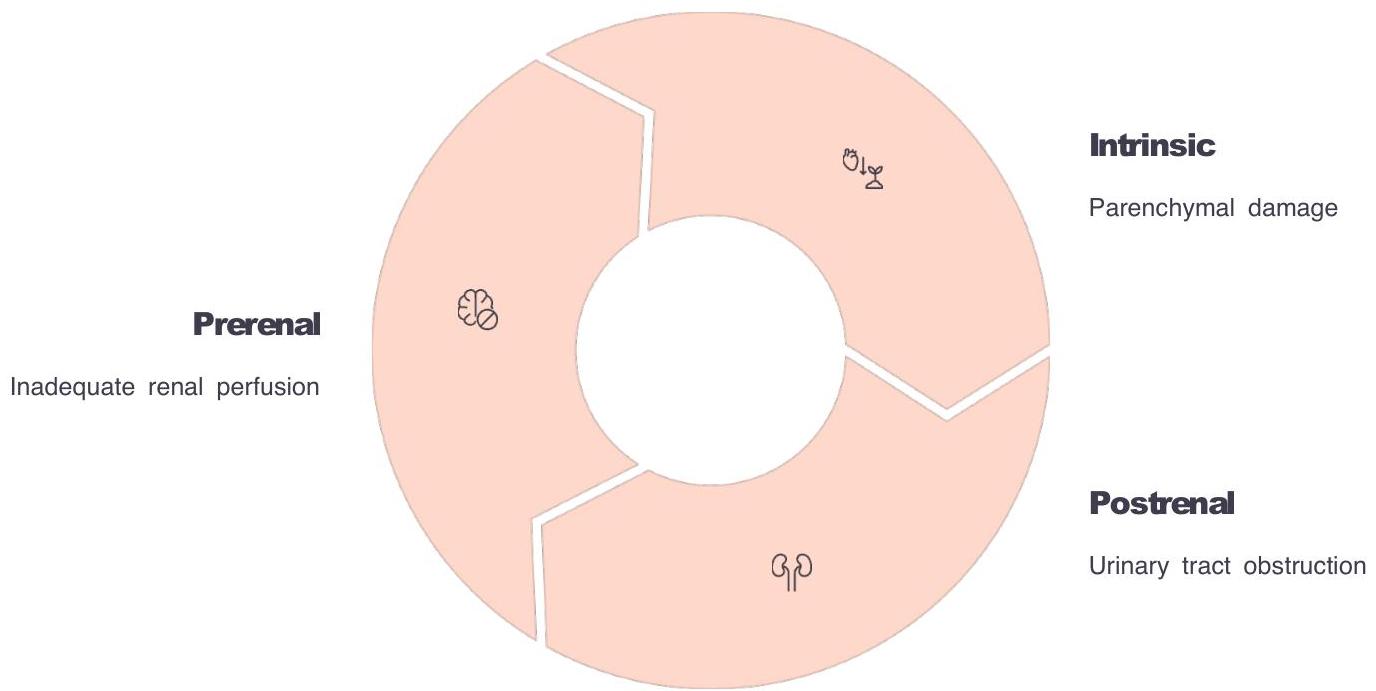
Etiologies of Acute Kidney Injury
The traditional classification system divides AKI into three main categories based on the anatomical location of the primary problem. This approach guides the diagnostic workup and initial management.
1. Prerenal
- Hypovolaemia:
- Gastroenteritis
- Burns
- Sepsis
- Haemorrhage
- Nephrotic syndrome
- Circulatory failure
2. Renal (Intrinsic)
- Vascular:
- Haemolytic uraemic syndrome (HUS)
- Vasculitis
- Embolus
- Renal vein thrombosis
- Tubular:
- Acute tubular necrosis (ATN)
- Ischaemic
- Toxic
- Obstructive
- Glomerular:
- Glomerulonephritis
- Interstitial:
- Interstitial nephritis
- Pyelonephritis
3. Postrenal
- Obstruction:
- Congenital (e.g., posterior urethral valves)
- Acquired (e.g., blocked urinary catheter)
Category Details
Prerenal Acute Kidney Injury
Definition
Hypoperfusion of the kidney leading to decreased glomerular filtration rate (GFR) while maintaining structurally intact nephrons. The kidneys respond appropriately by conserving sodium and water.
Common Causes in Pediatrics
- Hypovolemia: Gastrointestinal losses (vomiting, diarrhea), hemorrhage, or third-space losses.
- Decreased cardiac output: Congenital heart disease, myocarditis.
- Sepsis: With distributive shock.
- Hepatorenal syndrome.
Prerenal AKI is the most common form in pediatrics and is potentially reversible with prompt restoration of renal perfusion.

Intrinsic (Renal) Acute Kidney Injury
Definition
Structural damage to the kidney parenchyma involving the glomeruli, tubules, interstitium, or vasculature.
Common Causes
- Prolonged Prerenal Insults: Uncorrected hypoperfusion leading to Acute Tubular Necrosis (ATN). ATN is the most common form of intrinsic AKI.
- Nephrotoxins: Medications (aminoglycosides, contrast media), myoglobin, hemoglobin.
- Vascular Disorders: Hemolytic uremic syndrome (HUS), Bilateral renal vein thrombosis, Cortical necrosis.
- Glomerular Disease: Post-infectious glomerulonephritis, Rapidly progressive GN.
- Interstitial Nephritis: Drug-induced (NSAIDs, antibiotics), Infection-related.
Pathophysiology
The pathophysiology involves complex interactions between vascular, inflammatory, and tubular mechanisms:
- Vascular Injury: Microvascular injury with endothelial damage leads to reduced perfusion.
- Reduced perfusion: ischemia or toxin exposure
- Tubular Damage: Cell death, dysfunction, cast formation, and tubular obstruction.
- Cellular Injury: ATP depletion, oxidative stress.
- Reduced Function: Decreased GFR, electrolyte abnormalities.
Postrenal Acute Kidney Injury
Definition
Obstruction to urine flow at any level of the urinary tract (renal pelvis to external urethral meatus), leading to increased backpressure and decreased glomerular filtration.
Common Causes in Pediatrics
- Congenital Anomalies:
- Posterior urethral valves (most common obstructive uropathy in male infants).
- Ureteropelvic junction obstruction.
- Ureterocele.
- Acquired Conditions:
- Nephrolithiasis (bilateral or in solitary kidney).
- Neuropathic bladder (spinal cord injury, myelomeningocele).
- Tumor compression or Blood clots.
 Renal ultrasound demonstrating hydronephrosis from urinary tract obstruction a hallmark .finding in postrenal AKI
Renal ultrasound demonstrating hydronephrosis from urinary tract obstruction a hallmark .finding in postrenal AKI
Clinical Assessment and Diagnosis of AKI
1. Clinical History
A thorough history provides essential diagnostic information for determining the etiology.
- General Assessment: Decreased oral intake, fluid losses (vomiting, diarrhea), symptoms of dehydration or heart failure.
- Specific Clues:
- Sore throat/fever (10 days prior): Suggests Post-streptococcal glomerulonephritis.
- Bloody diarrhea (with progressive pallor): Suggests Hemolytic Uremic Syndrome (HUS).
- Medication History: NSAID use, aminoglycosides, contrast exposure.
- Systemic Symptoms: Rash, arthritis (systemic lupus, vasculitis).
2. Physical Examination
- Circulatory Assessment:
- Prerenal signs: Low BP, poor capillary refill, cool peripheries (may respond to fluid challenge).
- Volume Overload: Normal/raised BP, raised JVP, good peripheral perfusion, gallop rhythm.
- Fluid Status: Weight comparison, skin turgor, edema (nephrotic/nephritic), ascites.
- Urinary Tract: Palpable bladder (obstructive nephropathy), urine output measurement.
- Skin: Drug rash (interstitial nephritis), purpura (vasculitis/Henoch-Schönlein).

3. Diagnostic Investigations
Urine Analysis
Biochemical analysis of urine provides valuable differential diagnostic information, particularly between prerenal and intrinsic causes.
- Urinalysis:
- Dipstick: Blood, protein, glucose (glucose with normal blood sugar suggests tubular dysfunction/interstitial nephritis).
- Microscopy:
- ATN: Muddy brown granular casts, renal tubular epithelial cells.
- Glomerulonephritis: RBC casts, dysmorphic RBCs.
- AIN: WBC casts, eosinophiluria.
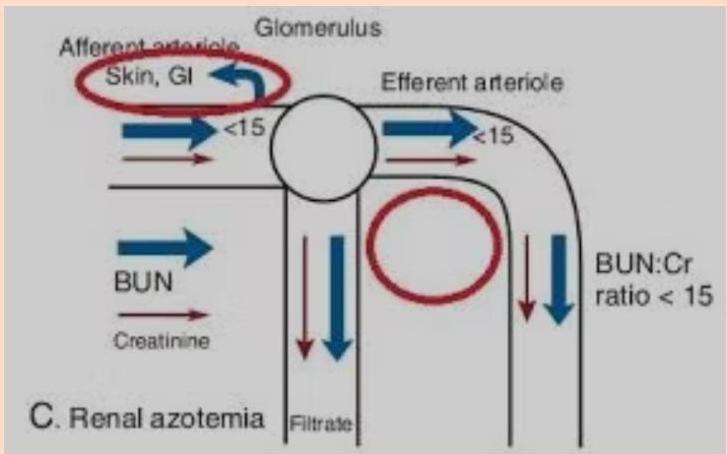
- Urine Indices (Differentiation):
- Prerenal: Concentrated urine (high osmolality), Low Na+, High BUN:Cr ratio.
- Intrinsic: Dilute urine (low osmolality), High Na+, Low BUN:Cr ratio.
| Urine Indices | Prerenal Failure | Intrinsic Renal Failure |
|---|---|---|
| Osmolality | >500 (conc.) | <300 (dilute) |
| Urine Na+ (mEq/L) | <10 | >40 |
| Urine:Plasma Urea Ratio | >10:1 | <7:1 |
| Fractional Excretion of Na+ (FENa) | <1% | >1% (>2.5-3% in neonates) |
Note: FENa is most useful when calculated with the first available urine sample before significant fluid resuscitation.
Blood Studies
- Biochemistry: Comprehensive electrolyte panel (Na, K, Cl, Ca, PO4, Mg), Urea, Creatinine, Urate.
- Hematology: CBC with blood film (check for schistocytes in HUS).
- Acid-Base: Venous or capillary blood gas (metabolic acidosis).
- Serology (for Intrinsic causes):
- Streptococcal antibodies (ASO, anti-DNase B).
- Complement levels (C3, C4). low in - , ,post infectious GN MPGN lupus nephritis
- Autoimmune markers (ANA, anti-dsDNA, ANCA for vasculitis, Anti-GBM for goodpasture’s syndrome).
Imaging Studies
- Renal Ultrasound:
- AKI: Normal or increased kidney size with slightly increased echogenicity.
- Chronic Renal Failure: Small kidneys with poor corticomedullary differentiation.
- Postrenal: Hydronephrosis, hydroureter, distended bladder.
- Advanced Imaging:
- Doppler: Evaluate vascular flow (thrombosis).
- Nuclear Scan: Perfusion defects, cortical necrosis, differential function.
- Voiding Cystourethrogram (VCUG): For posterior urethral valves / reflux.
- CT/MRI: Specific indications (stones, tumors).

Renal Biopsy Indications
- Rapidly increasing serum creatinine without clear cause.
- Suspected acute glomerulonephritis requiring specific therapy.
- Positive serology for systemic diseases (SLE, ANCA-vasculitis).
- Rapidly progressive glomerulonephritis (RPGN).
- Persistent AKI without improvement despite treatment.
- Need to distinguish between acute and chronic processes

Management Strategy
Key considerations for patient management
- Fluid Management – restrict fluids when volume overload is present and calculate maintenance needs carefully.
- Nutritional Support – provide high‑calorie, adequate‑protein intake to minimize catabolism.
- Electrolyte Management – monitor and correct potassium, calcium, and phosphate imbalances.
- Acid‑Base Correction – when pH < 7.2, administer sodium bicarbonate for severe metabolic acidosis.
- Medication Adjustment – adjust doses for renal function and avoid nephrotoxic agents.
General Principles
- Early Intervention: Prompt liaison with pediatric renal unit.
- Medication: Dose adjustment for renal function; strict avoidance of nephrotoxins (NSAIDs, aminoglycosides).
- Nutrition: High-calorie, appropriate protein intake to minimize catabolism.
Fluid Management
Fluid therapy must be tailored to the underlying cause and current volume status.
- Prerenal / Hypovolemia:
- Action: Urgent fluid resuscitation to restore intravascular volume.
- Protocol: Isotonic crystalloids (NS or LR) at 10-20 mL/kg boluses.
- Goal: Restore perfusion to prevent progression to ATN.
- Intrinsic (Euvolemic):
- Action: Maintain balance. Replace insensible loss (300 ml/m² per day) + urine output.
- Protocol: Replace insensible loss (300 ml/m²/day) + urine output matching.
- Volume Overload (Edema/Hypertension):
- Action: Fluid restriction and diuresis.
- Protocol: Restrict to insensible losses. Challenge with loop diuretic (e.g., Furosemide). Contraindicated if prerenal.
Management of Complications
Management of these abnormalities is critical for stabilizing patients with AKI and preventing complications while the underlying condition is addressed.
1. Electrolyte & Metabolic Abnormalities
| Abnormality | Treatment |
|---|---|
| Metabolic acidosis | Sodium bicarbonate (if pH <7.2) |
| Hyperphosphataemia | Calcium carbonate (binders), Dietary restriction |
| Hyperkalaemia | • Calcium gluconate (stabilize cardiac membrane if ECG changes) • Salbutamol (nebulized/IV) • Glucose and insulin • Calcium exchange resin • Dialysis (refractory cases) |
2. Hypertension
- If hypertension is due to extracellular fluid (ECF) volume overload:
- Challenge with a loop diuretic
- If due to volume overload: Loop diuretics.
- Vasodilators: Nifedipine or Hydralazine preferably .
- Target treatment of hyperkalaemia\
3. Postrenal Obstruction
- Rapid recognition is vital as it is readily reversible.
- Intervention: Bladder catheterization, nephrostomy, or surgical correction.
- Watch for Post-Obstructive Diuresis after relief.
Renal Replacement Therapy (Dialysis)
Indications for initiating acute dialysis (when conservative measures fail):
- Severe fluid overload → uncontrolled hypertension, pulmonary edema, or resistance to diuretics.
- Critical electrolyte disturbances → refractory hyper‑kalemia, extreme hypo‑ or hyper‑natremia.
- Toxin or metabolite clearance – effective for low‑molecular‑weight, non‑protein‑bound substances:
- Drugs: gentamicin, salicylates, lithium
- Poisons: ethanol, ethylene glycol
- Metabolites: leucine (maple‑syrup urine disease), ammonia
- Multisystem failure – when renal dysfunction is part of broader organ collapse.
Renal replacement therapy in pediatric patients
Options include peritoneal dialysis, hemodialysis, and continuous renal replacement therapies. Choice depends on:
- the child’s overall clinical condition and hemodynamic stability,
- availability of appropriate equipment and specialist expertise,
- the specific metabolic problem needing correction.