Posterior Urethral Valve (PUV) – Pathophysiology & Epidemiology
-
Most common cause of severe obstructive uropathy in male infants – ~1 case per 8,000 births.
-
Severity of obstruction determines downstream effects:
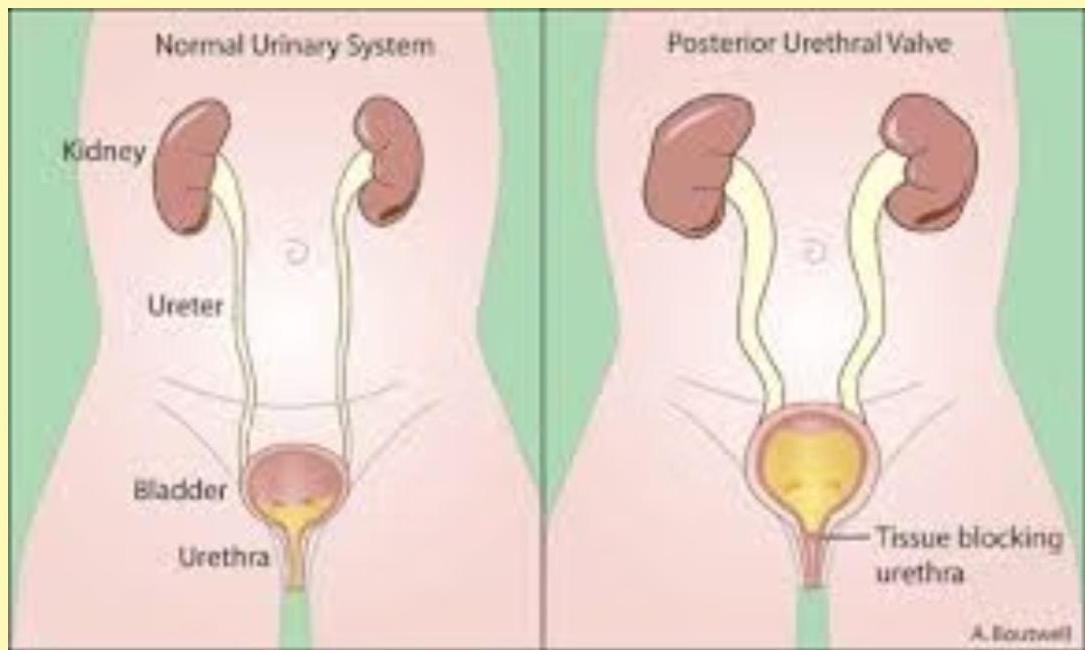
- Posterior urethral dilatation → bladder muscle hypertrophy → hydronephrosis → renal dysplasia → eventual renal failure.
- Prenatal diagnosis (second trimester) carries a poorer prognosis than a post‑natal discovery.
Anatomical note: the valve is a persistent embryologic membrane in the posterior urethra that creates a partial or complete blockage, producing a high‑pressure urinary system that involves the whole tract.
Clinical Presentation
- Neonatal – distended bladder, weak/dribbling stream, bilateral flank masses (hydronephrotic kidneys), sometimes respiratory distress from pulmonary hypoplasia.
- Delayed/late recognition – failure to thrive, uremic symptoms, recurrent UTIs, sepsis.
- Milder or later‑onset cases – isolated UTI, diurnal incontinence persisting > 6 y, enuresis resistant to standard therapy, or a noticeably poor stream reported by caregivers.
Diagnostic Imaging
-
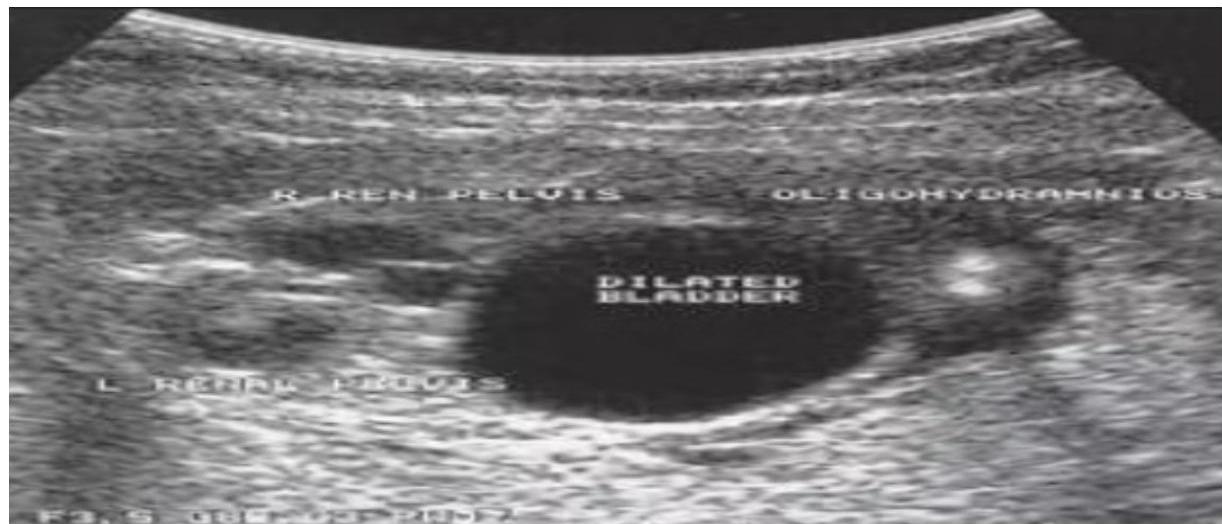
Antenatal ultrasound – Antenatal ultrasound showing urinary outflow obstruction from posterior urethral valve, with characteristic findings of dilated posterior urethra, thickened bladder wall, and bilateral hydronephrosis.
-
Micturating Cystourethrogram (MCUG) – The definitive diagnostic study for PUV, showing the classic “keyhole” sign with dilated posterior urethra and bladder, often with vesicoureteral reflux. MCUG establishes the diagnosis and helps plan surgical intervention.
-1769065376526.webp)
-
Additional studies – Additional imaging studies may include renal scintigraphy to assess differential renal function and drainage, which helps in surgical planning and prognostication.
Treatment Approach
-
Initial management (stabilization):
- Insert a suprapubic catheter to relieve obstruction.
- Correct electrolyte disturbances & manage renal insufficiency.
- Start antibiotic prophylaxis to prevent UTIs.
-
Definitive therapy:
- Trans‑urethral ablation of valve leaflets using pediatric endoscopic equipment (first‑line).
- For neonates too small for endoscopy, a temporary vesicostomy may be performed.
-
Follow‑up care (long‑term):
- Ongoing monitoring of renal function, blood pressure, and urinary tract health.
- Management of persistent bladder dysfunction after valve ablation.
- Serial imaging to track upper‑tract changes and improvement.
In summary, PUV is a rare but critical obstructive condition in male infants; prompt recognition—ideally before irreversible renal damage—combined with timely decompression and definitive valve ablation offers the best chance for preserving kidney function and urinary health.

