APPROACH TO LYMPHADENOPATHY
Prepared by: DR. Salma ELgazzar
LEARNING OBJECTIVES
- Define lymphadenopathy.
- Provide a summary of nodal distribution and anatomic drainage.
- Discuss the differential diagnosis of localized and generalized lymphadenopathy.
- Develop a systematic approach to the evaluation and management of lymphadenopathy.
- Recognize worrisome features of lymphadenopathy that should prompt a referral for a biopsy.
ANATOMY AND PHYSIOLOGY
Lymphatic Drainage
| Region | Drained Area |
|---|---|
| CERVICAL | head and neck |
| HILAR | lungs |
| CELIAC | Upper abdominal viscera |
| INTERNAL ILIAC | Anal canal, bladder, vagina, prostate |
| PARA-AORTIC | Testes, ovaries, kidneys, uterus |
| AXILLARY | Upper extremity, breast, skin of upper trunk. |
| MEDIASTINAL | trachea & esophagus |
| SUPERIOR/INFERIOR MEENTERIC | Small & large intestines. |
| SUPERFICIAL INGUINAL | Anal canal, skin of lower trunk, scrotum, vulva |
| POPLITEAL | Dorsolateral foot, posterior calf |
The Lymphatic System
- Cervical lymph nodes
- Axillary lymph nodes
- Mesenteric lymph nodes
- Iliac lymph nodes
- Iguinal lymph nodes
- Supraclavicular lymph nodes
- Thoracic duct
- Cisterna chyli
- Lumbar lymph nodes
- Popliteal lymph nodes
Lymph Nodes
-
Children often have easily palpable lymph nodes, particularly in the anterior cervical, inguinal and axillary regions.
-
Generalized lymphadenopathy may be present with viral infections, e.g. exanthems or infectious mononucleosis or systemic diseases, e.g. juvenile idiopathic arthritis.
-
Supraclavicular nodes of any size at any age or nodes that are firm, non-tender of variable size and matted together warrant further investigation, as they can be associated with malignancy.
-
Erythema, warmth, tenderness and fluctuation of a node suggest lymphadenitis of infective origin.
-
Nodes of variable size and consistency – is it TB?
DEFINITIONS
- Lymphadenopathy: defined as enlargement of lymph nodes. Enlarged lymph node(s). LN > 2cm have increased chance of being caused by serious pathology.
- This process is often secondary to infection and is frequently benign and self-limited.
- It is crucial to rule out rarer, more serious causes such as lymphomas or leukemia.
- Normally, lymphoid tissue enlarges until puberty and then undergoes gradual atrophy throughout the rest of life.
- Normal lymph nodes are most prominent in children ages 4 to 8 years old.
- Lymphadenitis: enlarged lymph node that is due to an inflammatory / infective process; usually warm, tender, erythematous +/- systemically unwell
- Generalised lymphadenopathy: lymph nodes enlarged in 2 or more non-contiguous areas
- Localised lymphadenopathy: lymph nodes enlarged in only one area
- Acute lymphadenopathy: < 2 weeks
- Subacute lymphadenopathy: 2 – 6 weeks
- Chronic lymphadenopathy: > 6 weeks
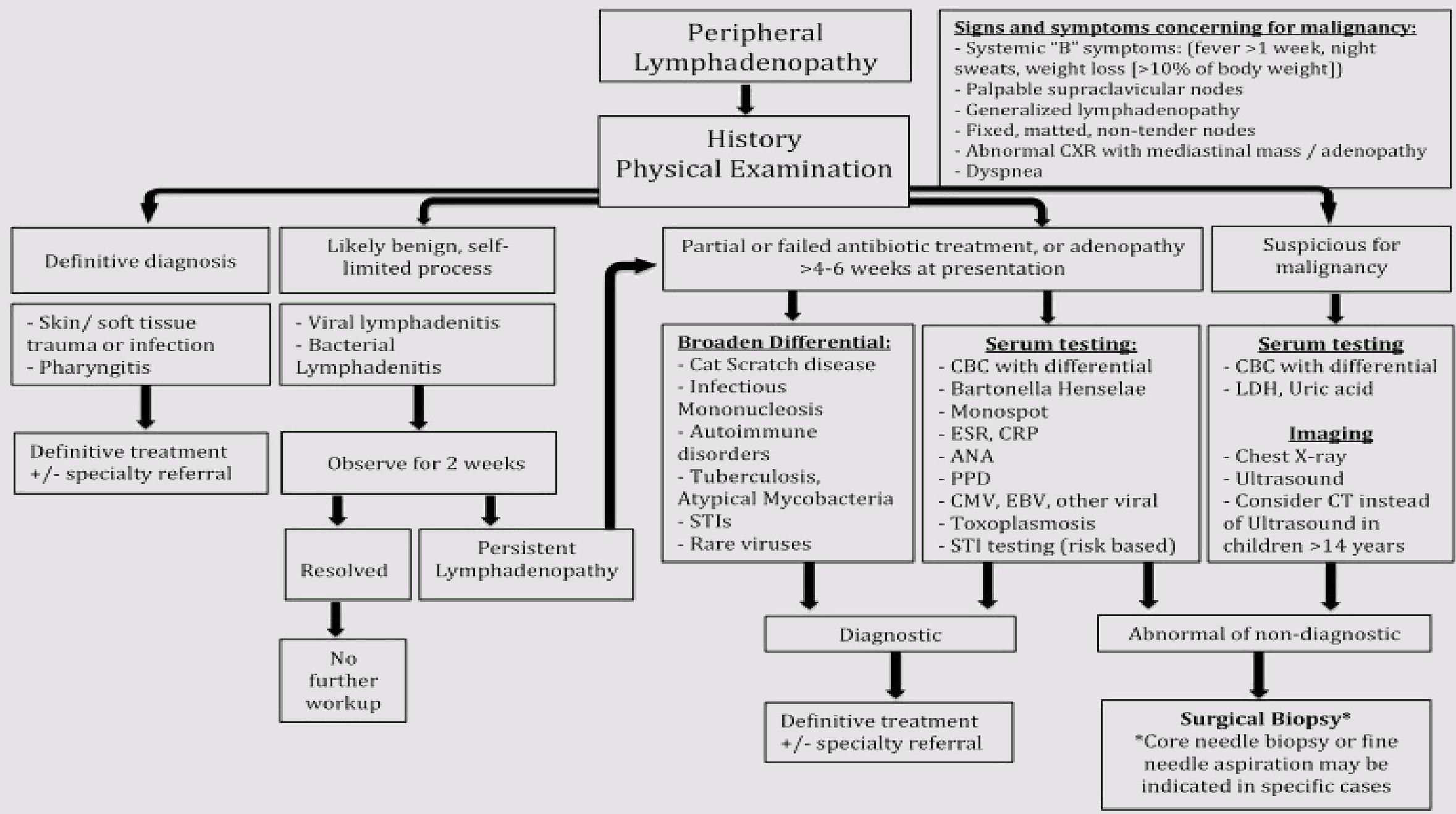
CLINICAL APPROACH TO LYMPHADENOPATHY
Important Questions
- Is it a lymph node?
- What is the character of enlarged lymph node?
- Is the lymph node enlarged?
- Localized VS generalized
History
- Characteristics of the lymph node(s). Onset, size, duration? Is it painful or erythematous? Generalized or local? Associated symptoms?
- Recent infections. Has this child had a recent infection that may explain a lymphadenopathy? Upper respiratory tract symptoms? Any respiratory symptoms? Rashes? Changes in bowel movements or voiding patterns? Any bone or joint pain? Changes in vision? Headaches?
- Constitutional symptoms? Fever, night sweats, weight loss?
- Associated other systemic symptoms
- Skin lesions or trauma? Cat scratch? Animal/insect bites? Other open wounds? Dental abscesses?
- General health. Has this child been hospitalized in the past? Any ongoing medical conditions? Any surgeries? Any visits to the Emergency department?
- Recent Travel & Exposures. Could the child have picked up an infection while traveling? Has the child been in contact with infected individuals? Viral respiratory exposures such as EBV/CMV? TB exposure?
- Immunization status. MMR?
- Medications. Carbemazepine or phenytoin? There are a wide variety of medications which can cause lymphadenopathy.
- Allergies.
- In adolescents, it is also important to ask about IV drug use and obtain a sexual history.
- Cats. Think of toxoplasmosis and bartonella
- Food. Ingestion of unpasteurized animal milk (brucellosis), or undercooked meats (toxoplasmosis, tularemia)
Age Factors
- Lymph node enlargement in children less than 5 years most likely infectious
- Histiocytosis can cause lymphadenopathy in children < 3 years
- Large lymph node in neonate most likely related to congenital infection
- Likelihood of malignant lymphoma increases in adolescents
Location Factors
- Supraclavicular lymphadenopathy is always abnormal and the chances of malignancy are high
Size Factors
- Size of the enlarged lymph node aids in determining the need for further evaluation
- Axillary and cervical > 1 cm
- Inguinal > 1.5 cm
- Epitrochlear > 0.5 cm
- Anywhere > 2 cm
Characteristics
- Usually develops over weeks or months.
- Nontender, discrete, firm, rubbery, often immobile
Physical Exam
- Children often have easily palpable nodes enlarged in response to infection.
- Nodes that are usually palpable include anterior cervical, inguinal, and axillary regions.
- Perform a complete physical exam “general appearance, vital signs and growth parameters.”
- Are they febrile? Plot them on the appropriate growth chart; have they lost weight?
- Then perform a complete systematic physical exam.
- Always pay special attention to the area of the enlarged node for a focus of infection.
Head and Neck
Examine closely for:
- Scalp infection (e.g. seborrheic dermatitis, tinea capitius)
- Conjunctivitis injection
- Oropharynx for pharyngitis, dental problems, HSV ginivostomatitis
- Ears for acute otitis media
Abdomen
Examine closely for:
- Hepatosplenomegaly (this is actually considered part of your lymph node exam!)
- Abdominal masses (e.g. neuroblastoma)
Skin
Examine closely for:
- Any rashes
- Petechiae, purpura, ecchymoses (e.g. thrombocytopenia)
Lymph Node Exam
When palpating a lymph node it is important to consider the following:
- Size (measure them)
- Location
- Fixation
- Consistency
- Tenderness
DIFFERENTIAL DIAGNOSIS
Differential Diagnosis of Systemic Generalized Lymphadenopathy
| INFANT | CHILD | ADOLESCENT |
|---|---|---|
| COMMON CAUSES | ||
| Syphilis | Viral infection | Viral infection |
| Toxoplasmosis | EBV | EBV |
| CMV | CMV | CMV |
| HIV | HIV | HIV |
| Toxoplasmosis | Toxoplasmosis | |
| Syphilis | ||
| RARE CAUSES | ||
| Chagas disease | Serum sickness | Serum sickness |
| Leukemia | SLE, JIA | SLE, JIA |
| Tuberculosis | Leukemia/lymphoma | Leukemia/lymphoma |
| Reticuloendotheliosis | Tuberculosis | Hodgkin disease |
| Lymphoproliferative disease | Measles | Lymphoproliferative disease |
| Metabolic storage disease | Sarcoidosis | Tuberculosis |
| Histiocytic disorders | Fungal infection | Histoplasmosis |
| Plague | Sarcoidosis | |
| Langerhans cell histiocytosis | Fungal infection | |
| Chronic granulomatous disease | Plague | |
| Sinus histiocytosis | Drug reaction | |
| Drug reaction | Castleman disease |
Sites of Local Lymphadenopathy and Associated Diseases
CERVICAL
- Oropharyngeal infection (viral or group A streptococcal, staphylococcal)
- Scalp infection/infestation (head lice)
- Mycobacterial lymphadenitis (tuberculosis and nontuberculous mycobacteria)
- Viral infection (EBV, CMV, HHV-6)
- Cat-scratch disease
- Toxoplasmosis
- Kawasaki disease
- Thyroid disease
ANTERIOR AURICULAR
- Conjunctivitis
- Other eye infection
- Facial cellulitis
- Otitis media
- Viral infection (especially rubella, parvovirus)
SUPRACLAVICULAR
- Malignancy or infection in the mediastinum (right)
- Metastatic malignancy from the abdomen (left)
- Lymphoma
- Tuberculosis
EPITROCHLEAR
- Hand infection, arm infection
- Lymphoma
- Sarcoid
- Syphilis
INGUINAL
- Urinary tract infection
- Venereal disease (especially syphilis or lymphogranuloma venereum)
- Other perineal infections
- Lower extremity suppurative infection
HILAR
- Tuberculosis
- Histoplasmosis
- Leukemia/lymphoma
- Hodgkin disease
- Metastatic malignancy
- Sarcoidosis
AXILLARY
- Cat-scratch disease
- Arm or chest wall infection
- Malignancy of chest wall
- Leukemia/lymphoma
- Brucellosis
ABDOMINAL
- Malignancies
- Mesenteric adenitis (measles, tuberculosis, Yersinia, group A streptococcus)
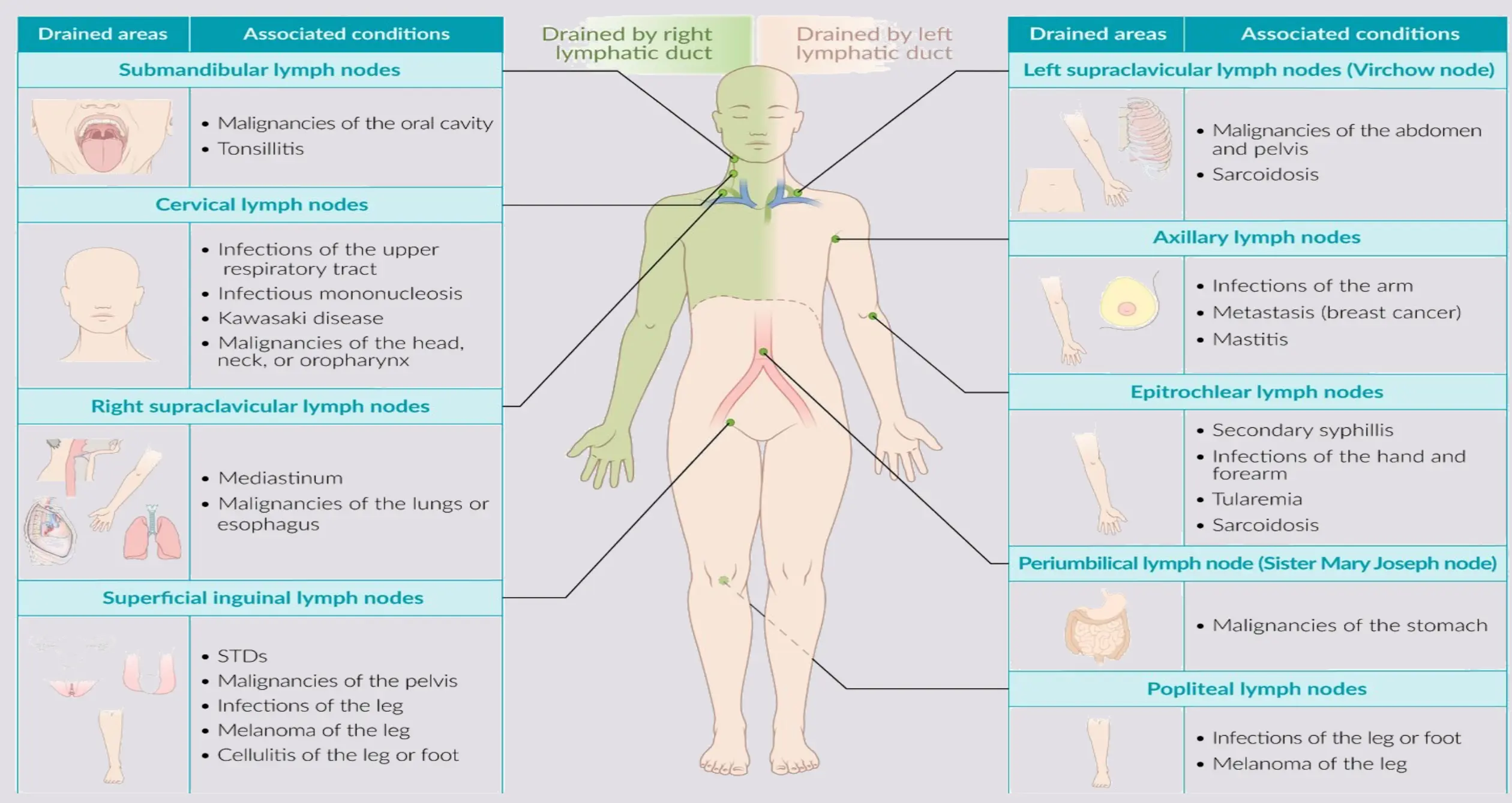
Drainage Patterns and Associated Conditions
RED FLAGS AND WORRISOME FINDINGS Z
Comparison of Findings
| Less concerning findings | Worrisome findings which increase risk of malignancy |
|---|---|
| localized | Generalized adenopathy |
| < 1-2 cm (depending on location) | > 2 cm |
| Cervical, inguinal and axillary | Occipital, auricular, supraclavicular epitrochlear or posterior cervical nodes |
| erythema | Matted |
| tender | Non tender |
| warm | Firm |
| fluctuant | Systemic symptoms |
Red Flags List z
- Weight loss
- Bone pain
- Drenching night sweats
- Indications of possible malignancy
- Firm, non-mobile nodes
- Non-tender nodes
- Lymph nodes that are greater than 2 cm in size
- Lymph nodes that are progressively enlarging
- Involvement of axillary nodes in the absence of local infection or dermatitis
- Involvement of supraclavicular nodes
- Hepatomegaly / splenomegaly
- Bruising on non-bony surfaces
EMERGENCY DEPARTMENT REFERRAL Unwell with fever and lymphadenopathy
Additional Warning Signs
- Lymph node size >2 cm
- Node increasing in size over 2 weeks
- No decrease in node size after 4-6 weeks
- Node not returned to baseline after 8-12 weeks
- Abnormal chest X-ray
- Presence of a supraclavicular node
- Presence of systemic signs and symptoms
- Fever
- Weight loss
- Night sweats
- Hepatosplenomegaly
INVESTIGATIONS AND IMAGING
Investigations
- Complete blood count, peripheral blood smear
- Erythrocyte sedimentation rate (non-specific)
- Rule out infectious causes: Monospot, CMV, EBV, & toxoplasma, bartonella titres, TB skin test, Anti-HIV test, CRP, ESR
- Hepatic and renal function + urinalysis (systemic disorders that can cause lymphadenopathy)
- Lactate dehydrogenase, uric acid, calcium, phosphate, magnesium if malignancy suspected
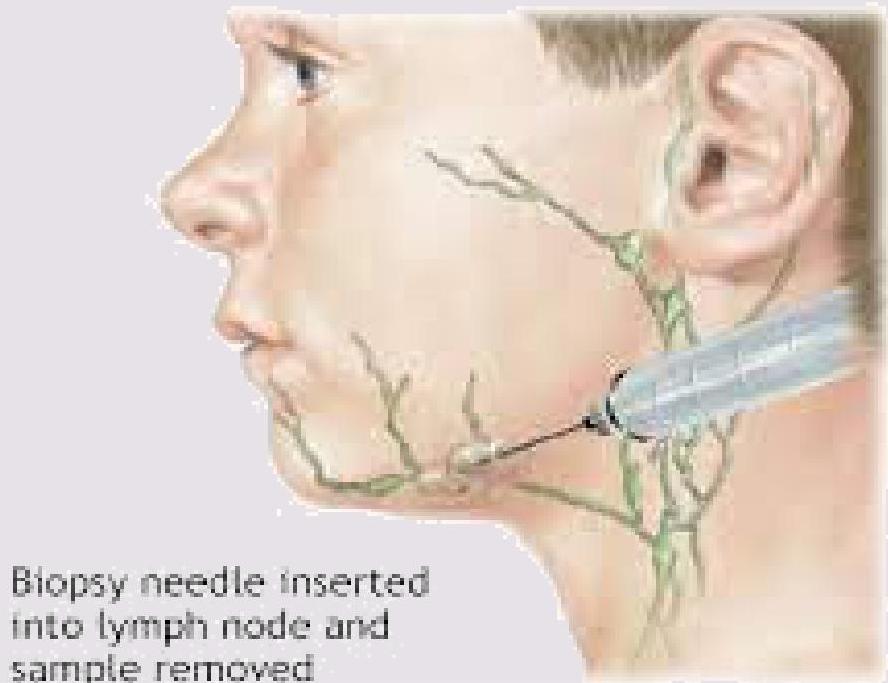
- Bone marrow, liver biopsies, CT or US guided lymph node biopsy
Imaging Studies Z
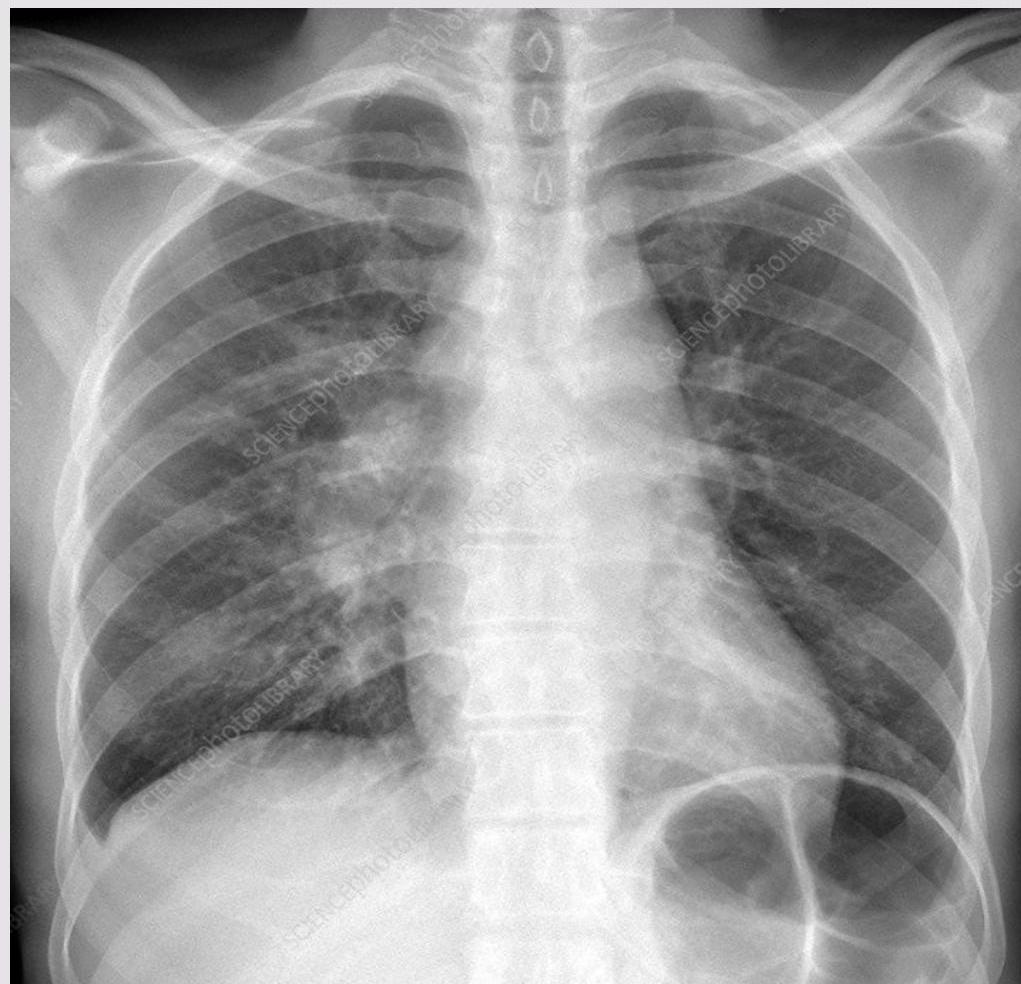
- Chest X-ray: This study will help determine the presence of mediastinal adenopathy and underlying pulmonary diseases including tuberculosis, coccidioidomycosis, lymphomas, and neuroblastoma.
- Ultrasound of the lymph node
- CT of the chest and/or abdomen: Supraclavicular adenopathy is highly associated with serious disease in the chest and abdomen.
- Nuclear medicine scanning: is helpful in the evaluation of lymphomas.
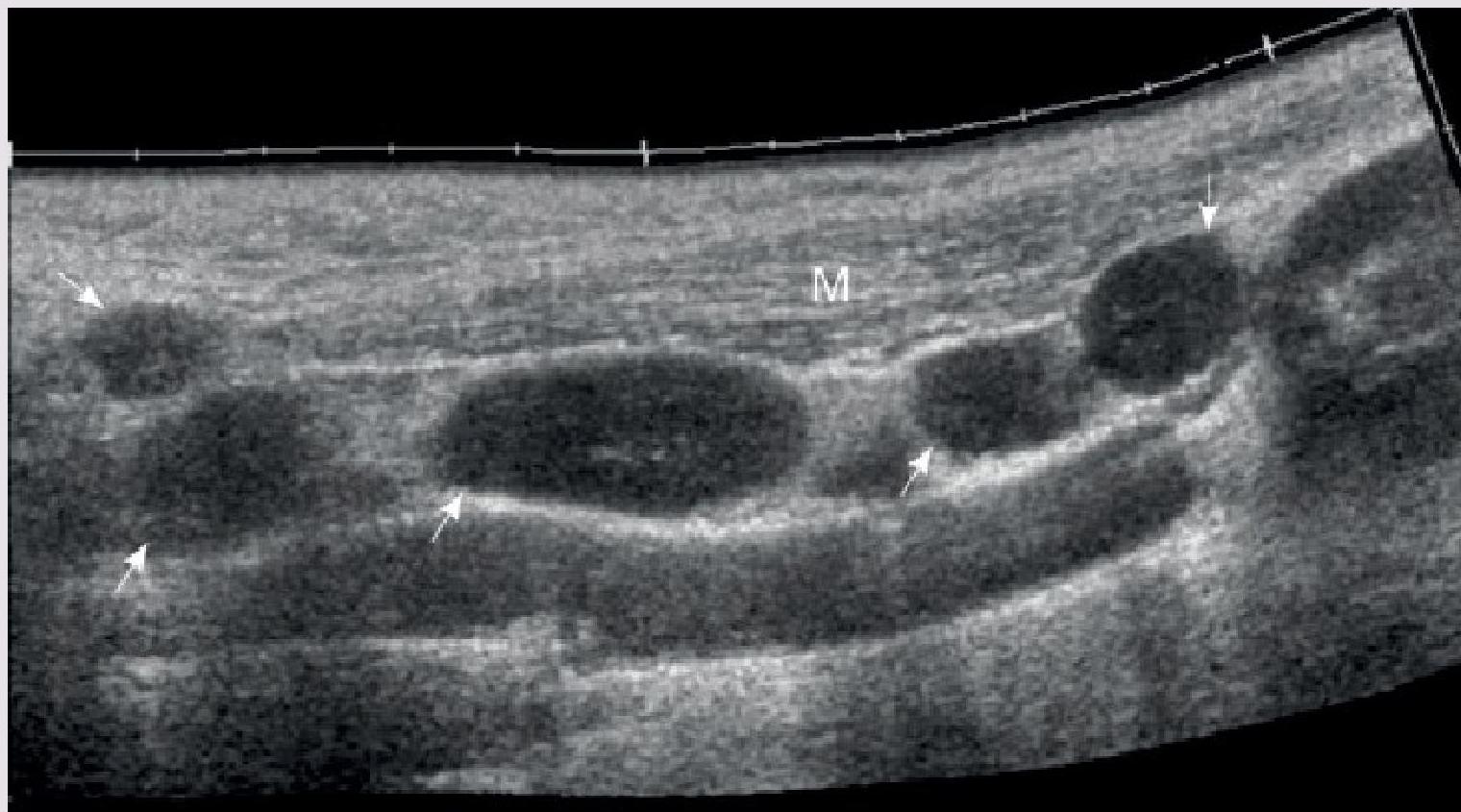 Multiple enlarged lymph nodes (arrows) along the sternocleidomastoid muscle (M) Z
Multiple enlarged lymph nodes (arrows) along the sternocleidomastoid muscle (M) Z
 Lymph node tuberculosis. Z
Lymph node tuberculosis. Z
BIOPSY CRITERIA
Size
-
2 cm
- Increasing over 2 weeks
- No decrease in size after 4 weeks
Location
- Supraclavicular
Consistency
- Hard
- Matted
- Rubbery
Associated features
- Abnormal CXR
- Fever
- Weight loss
- Hepatosplenomegaly
MANAGEMENT AND REFERRAL
Emergency Department Referral
- Unwell with fever and lymphadenopathy

General Paediatrics Referral
- Any red flags
- History and physical examination do not suggest an infectious cause
- Potentially infectious nodes have not responded to a course of antibiotics
Treatment (Management of acute adenitis)
- ☐ Well: oral antibiotics for 10 days, with review in 48 hours.
- ☑ Flucloxacillin
- ☑ Severe penicillin hypersensitivity: Erythromycin or other macrolide
- ☐ Neonates, unwell or failed oral Rx: refer for IV antibiotics
CONCLUSION
Take Home Messages
- Enlargement of one or more lymph nodes < 1 cm in diameter, particularly in cervical, occipital, and inguinal regions, is a common finding in otherwise healthy children
 The Take-Home Message
The Take-Home Message