ARRHYTHMIA
DR MANSOUR ALQURASHI
Objectives
At the end of this session students should be able to:
- Distinguish the normal from abnormal rhythms.
- Understand the pathophysiologic basis of arrhythmia.
- Differentiate ventricular from supraventricular arrhythmias.
- Recognize different types of supraventricular arrhythmias.
- Recognize the different types of heart block.
- Be familiar with strategies of arrhythmia management.
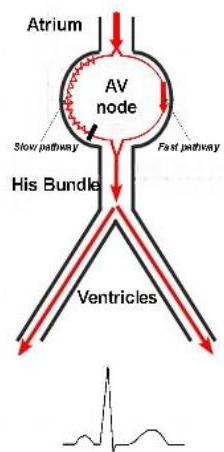
Basics
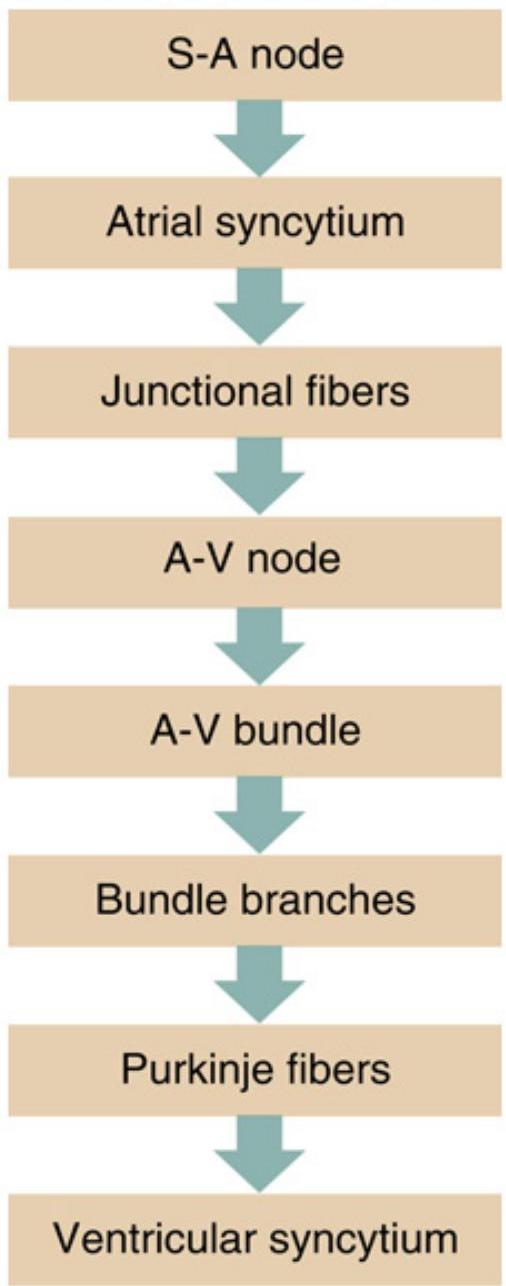
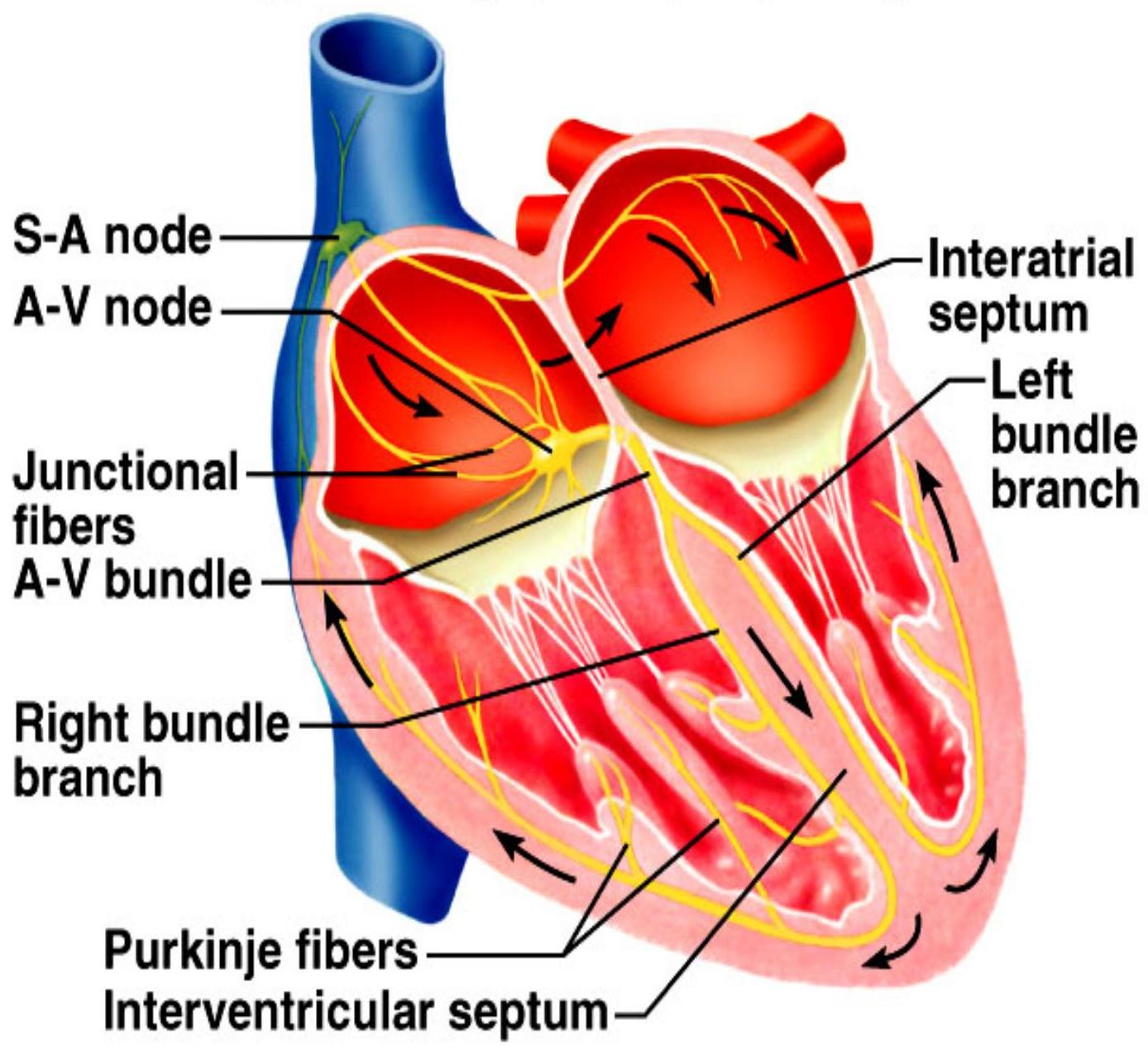
Conduction System Hierarchy
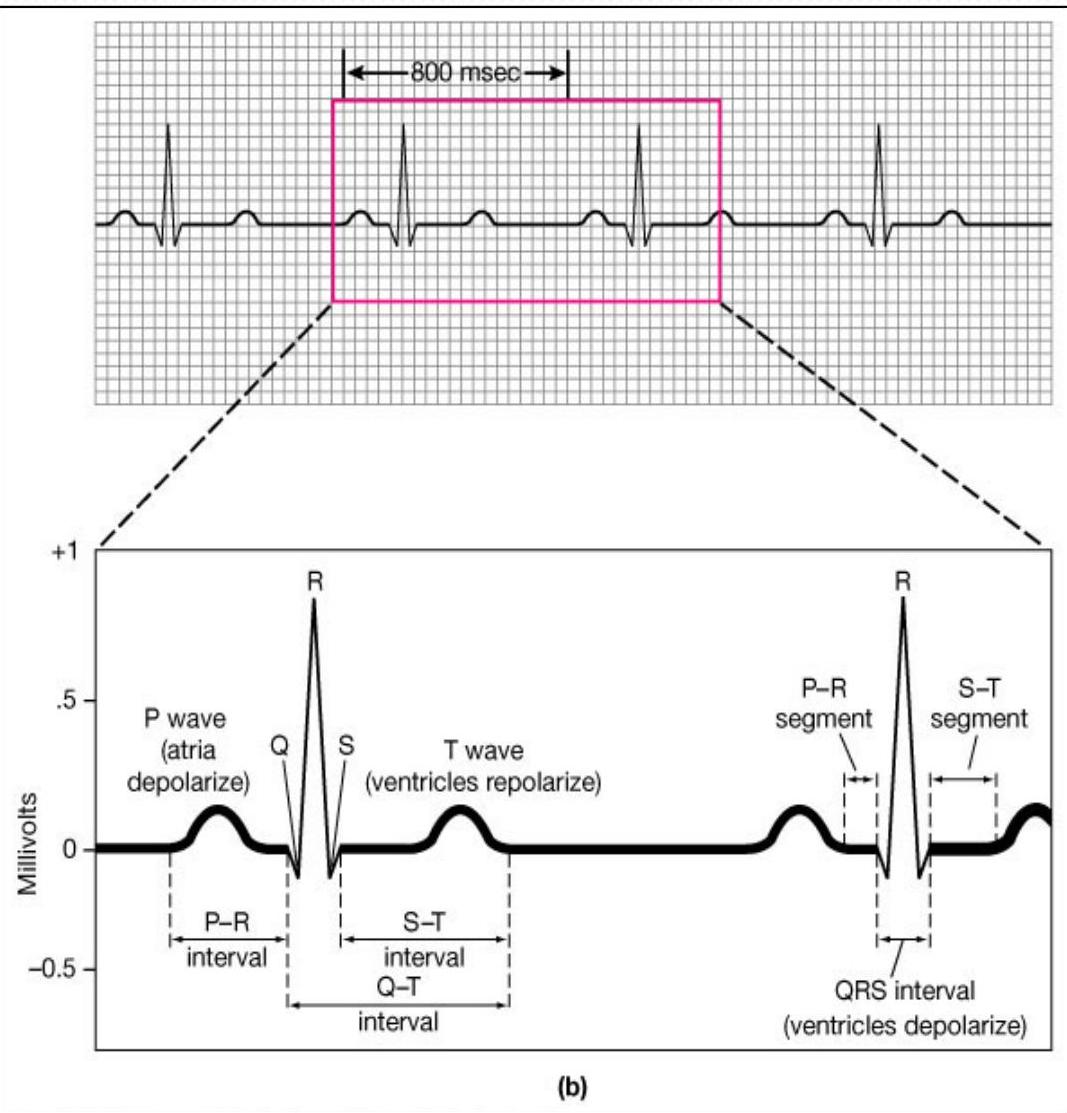
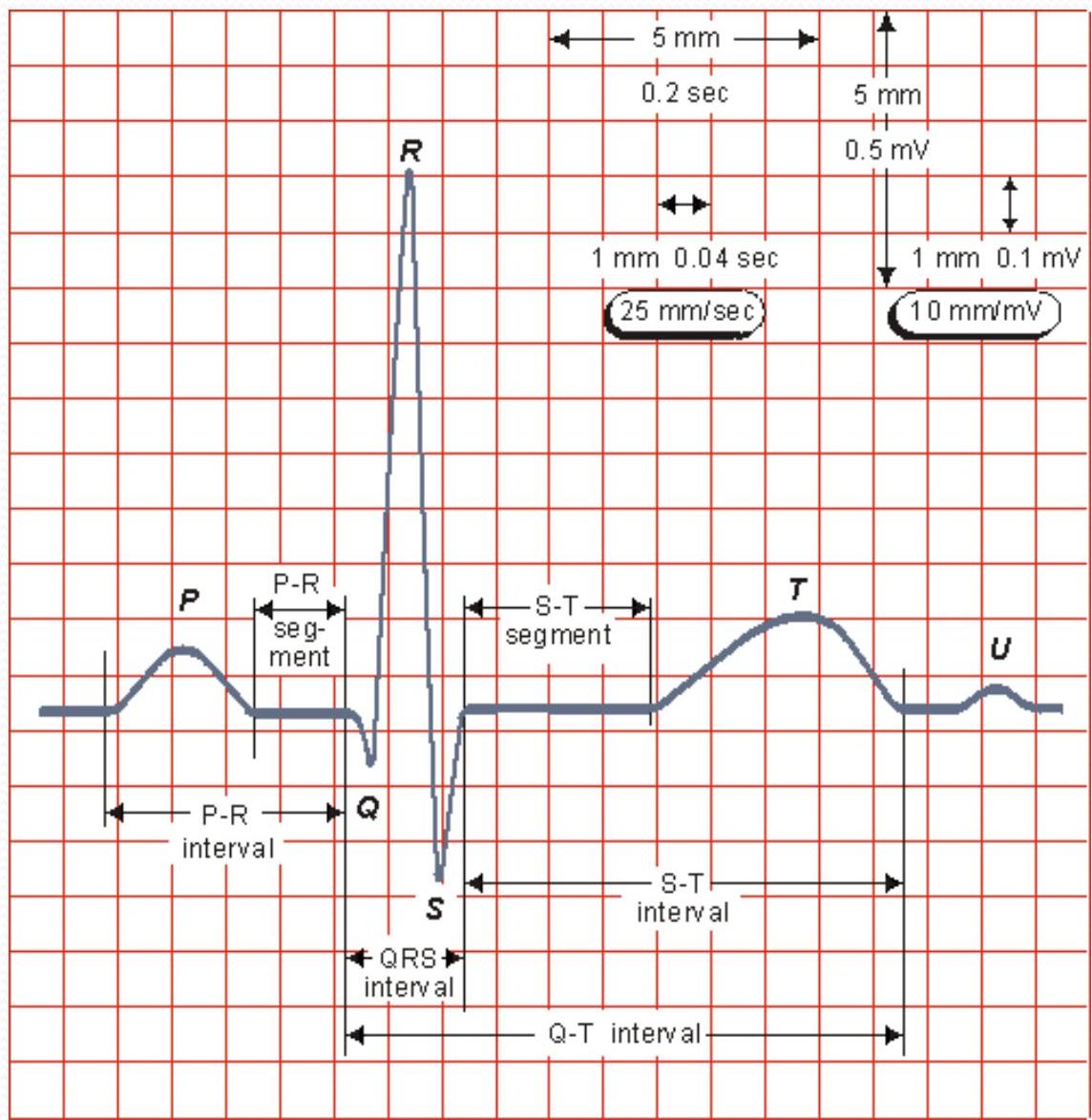
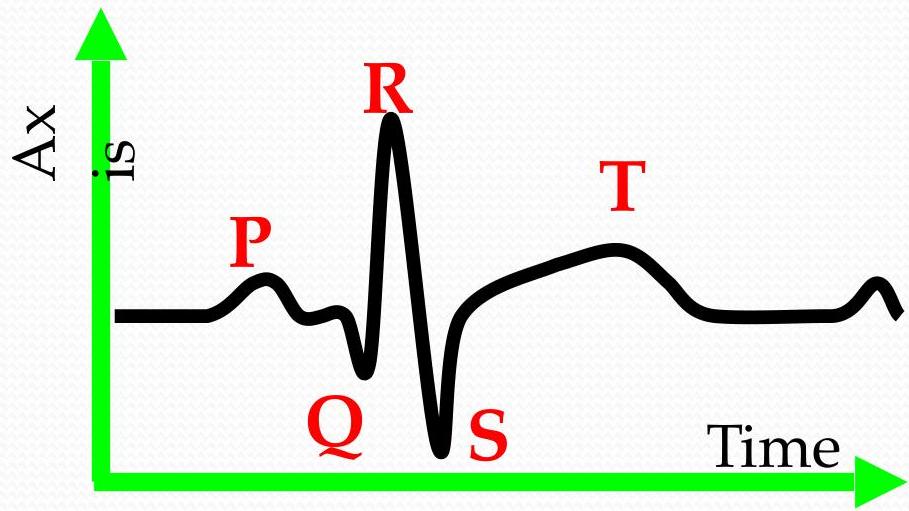
Basic ECG Elements
| Basic elements | Joining Segments | Duration Interval |
|---|---|---|
| P wave | PR segment | PR interval |
| QRS | ST segment | QT interval |
| T wave | TP segment | ST interval |
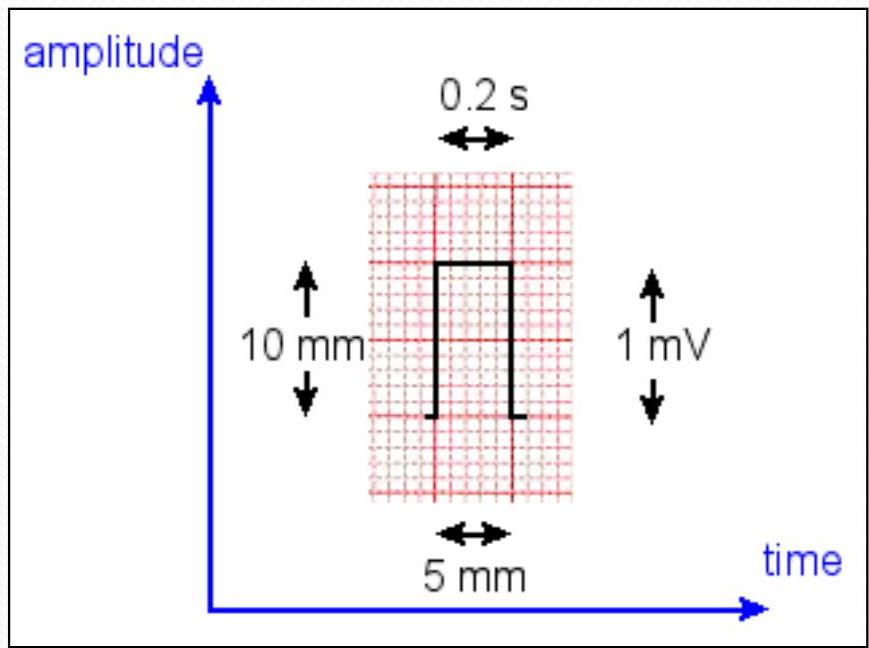
2 Dimensions
QRS
- 2 ss in adult
- 2.5 ss in children
PR interval
- 3 ss in children
- 5 ss in adult
Classification of Arrhythmia
| Variable | Classes | Classes | Classesx |
|---|---|---|---|
| Rate (Regular: 300 / No. of big bow between) | Tachycardia B.R. | Bradycardia | |
| Morphology | Narrow complex (Coming from above the ventricle) | Wide complex (Coming from ventricle) | |
| Origin | Supra-ventricular (Above AV node) | Junctional (at right AV side) | Ventricular (below AV node) |
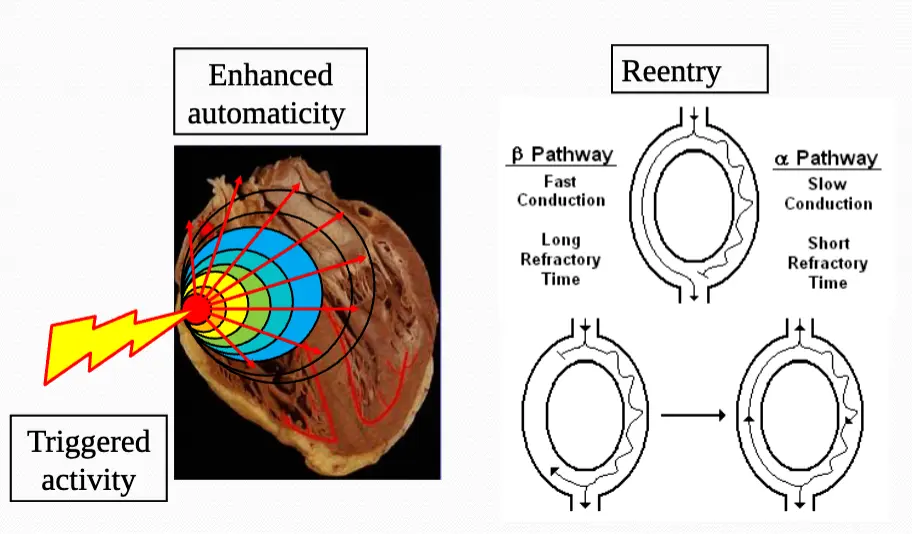
| Mechanism | Reentrant | Automatic | Triggered |
| P-QRS relationship | 1st degree AV block | 2nd degree AV block | 3rd degree AV block |
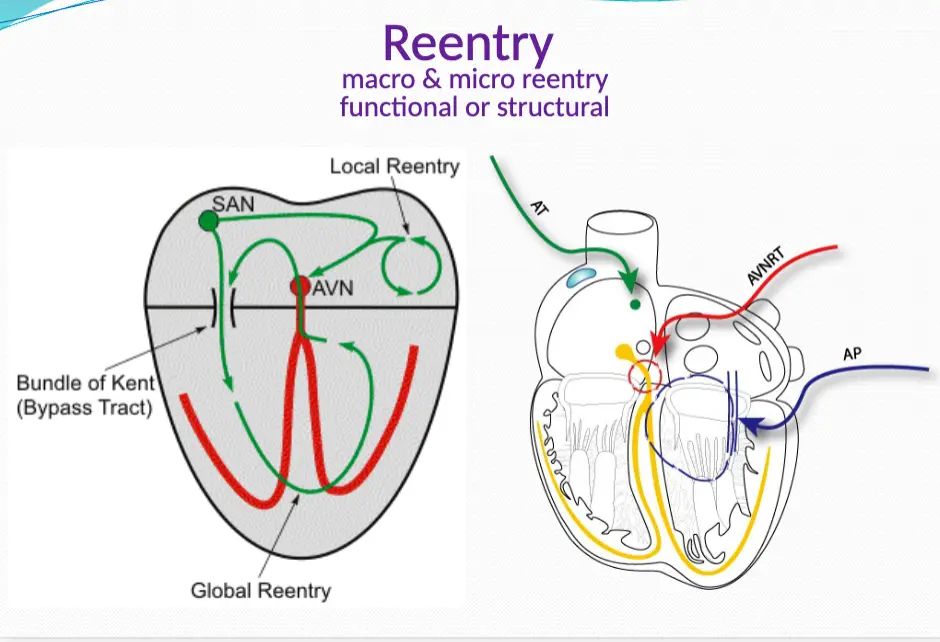
Mechanisms of Arrhythmia
Rhythm Analysis
(P-QRS)
| Rhythm (P waves & QRS) | ||
|---|---|---|
| Present | Sinus / non sinus | abnormal P wave means it’s not from sw node cualt come from AV node or from ventricular |
| Absent | Real / technical |
| Rate (P waves & QRS) | ||
|---|---|---|
| Calculation | QRS x 10 irregular 1500 no small scar between low QRS | |
| Slow | Appropriate/inappropriate | |
| Fast | Narrow/wide complex |
| Regularity (P waves & QRS) | ||
|---|---|---|
| Regular R - R | equal | |
| Irregular | Group beating or haphazard |
| P wave morphology & QRS morphology | ||
|---|---|---|
| Axis | up/down P waves, extreme axis | |
| Duration & Axis | Normal or wide (RBBB, LBBB), sup. axis |
| P-QRS relationship | ||
|---|---|---|
| Normal | 1:1, normal PR interval | |
| Abnormal | Ratio, duration (fixed, variable, unrelated) |
| Others (PR & QT intervals) | ||
|---|---|---|
| Normal | ||
| Abnormal | Long or short |
Sinus Rhythms
Normal Sinus Rhythm
- sinus
- 300 divided by each block for HR
- no. big spin
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| 60-100 bpm | Regular | Before each QRS, identical | .12 to .20 | <.12 |
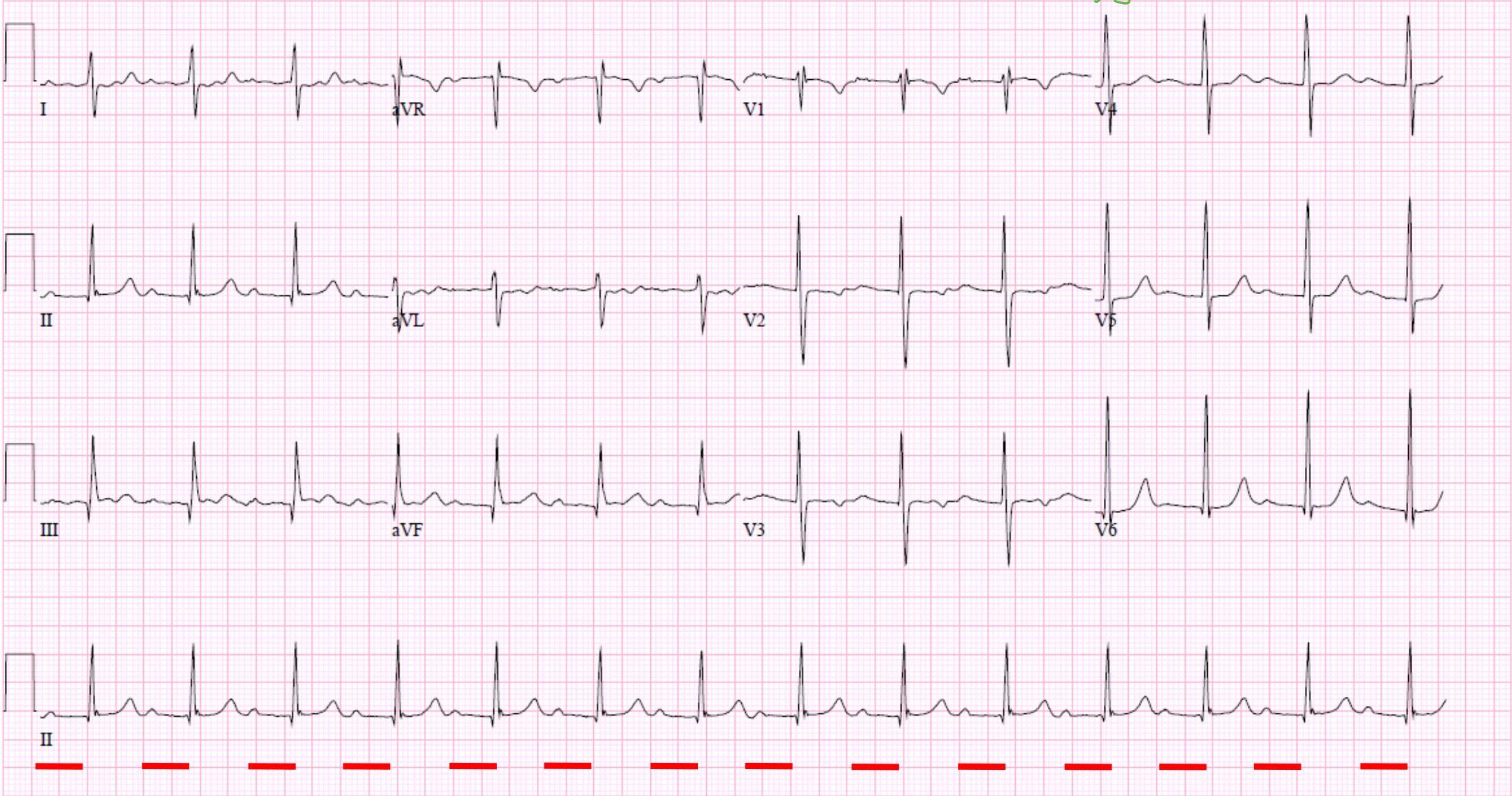
Sinus Tachycardia
- Sinus , Requireur
Features:
- P wave normal shape
- HR
- Varibality: “the sinus coming from SA nodes”
- HR > 300 in fetus > 250 in neonate > 180 in pediatric
- Regular: “the sinus coming from ectopic focus”
- R - R wave are fixed
- terminate immediately after valsova maneuver or carotid massage
Clinical Scenario:
- if some one with shock and has tachycardia
- How to know which is first.
- conect the ECG
- if sinus tachy → shock causes tachy (also if there cause for the shock: Diarrhea, vomiting…)
- if SUT → SUT complicated by shock or V tach
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| > 100 bpm | Regular | Before each QRS, identical | .12 to .20 | <.12 |
Sinus Bradycardia
- p^2 degree usually
- ⇐ Tachyon
- rarely cause Brady
Differential Diagnosis (child with Dec HR before doing ECG):
- Sinus Bradycardia
- 2nd, 3rd degree Heart block
- junctional rhythm
Causes:
- Sepsis - Dithaura
- B Blocker

| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| < 60 bpm | Regular | Before each QRS, identical | .12 to .20 | <.12 |
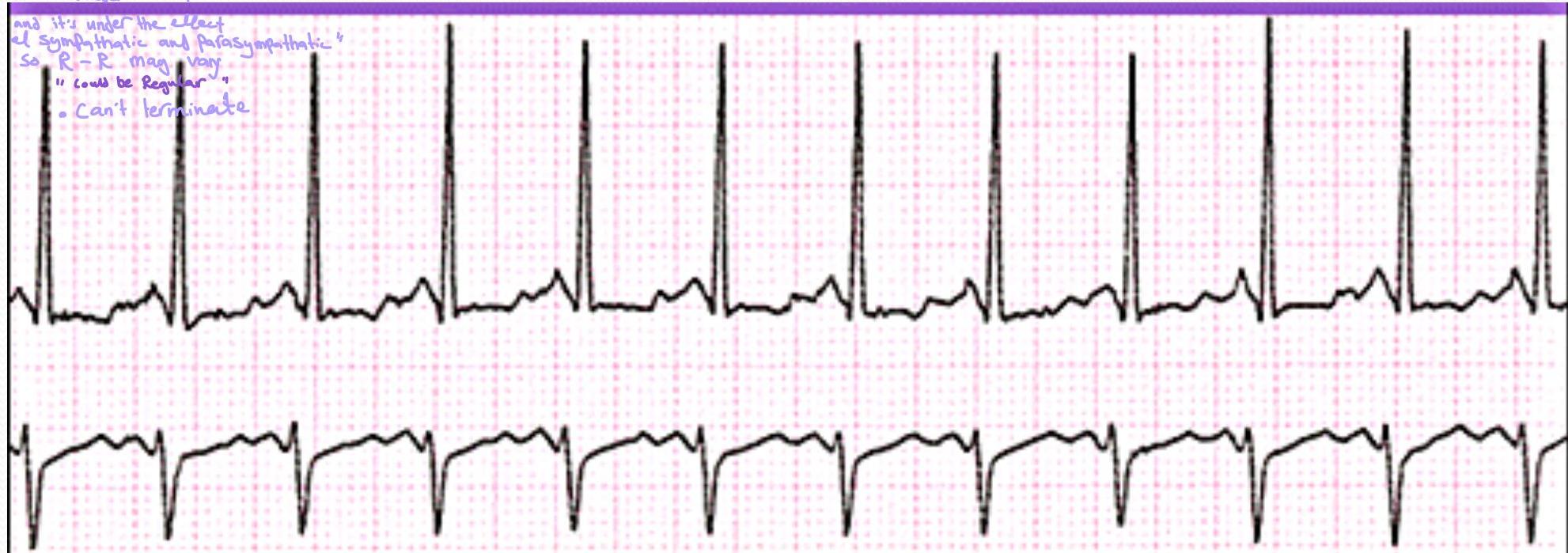
Sinus Arrhythmia
- Cuz SA notes under the effect of sympathetic and parasympathetic so HR may change due to different causes.
- (normal or abnormal?)
- (normal variation
- Sinus, irregular
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| Usually 60-100 bpm | Irregular | Before each QRS, identical (Sinus) | .12 to .20 | <.12 |
Notes:
- normal
- anything stimulate the heart
- Smoking
- Anti-histamine
- coffee
- abnormal P wave shape
- Coming earlier so P wave will be close to the previous QRS
- Compansatory Phase “R-R become pralong”
- It’s no treatment will heal by itself only advice the family to avoid rigers
Supraventricular Arrhythmias
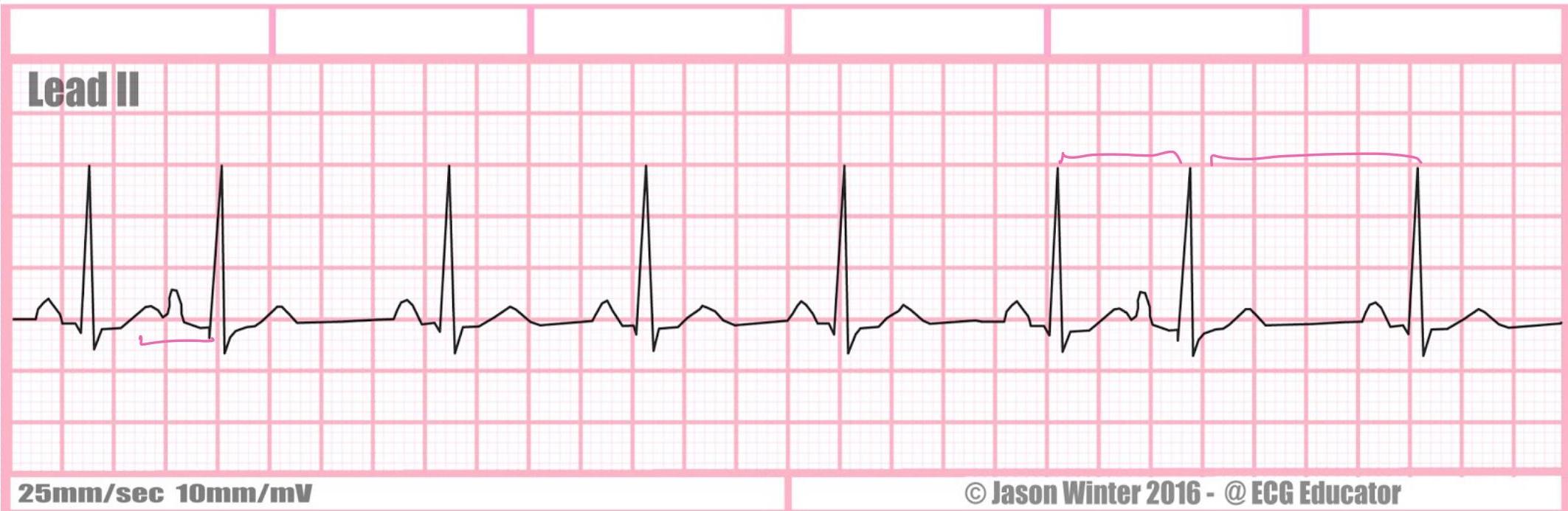
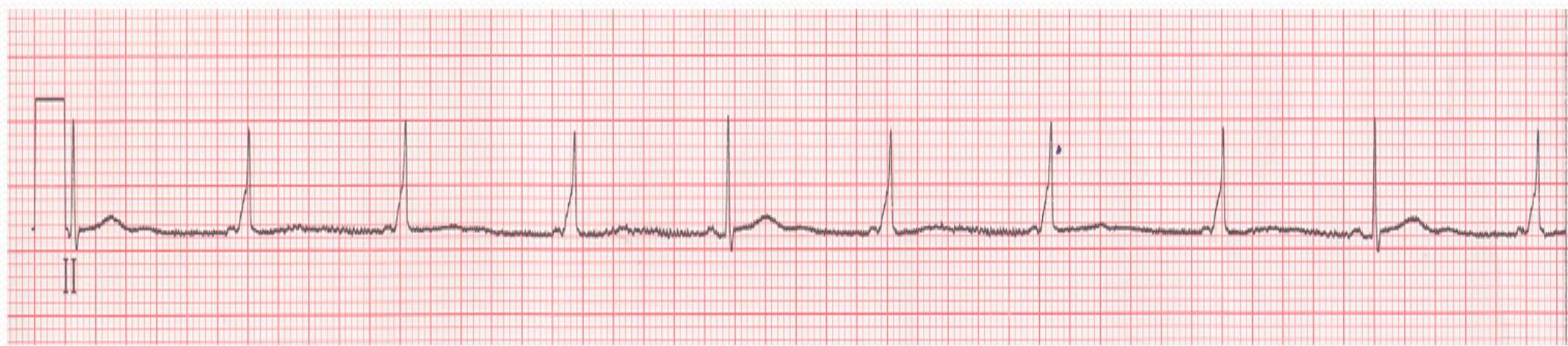
Premature Atrial Contraction (PAC)
Lead II
- short pralanges
- ectopic focus from Atrium
- 25 mm/sec 10 mm/mV

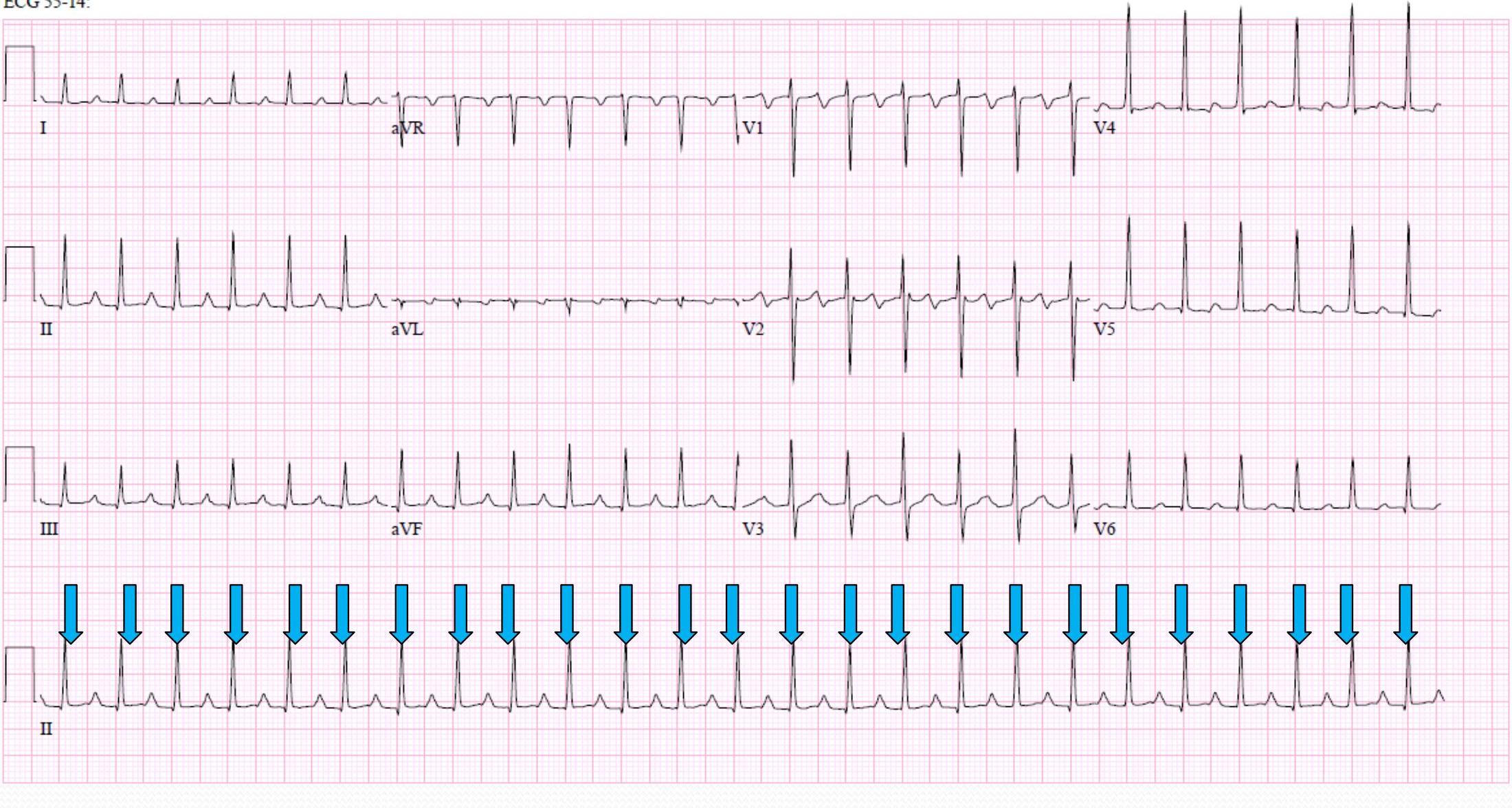
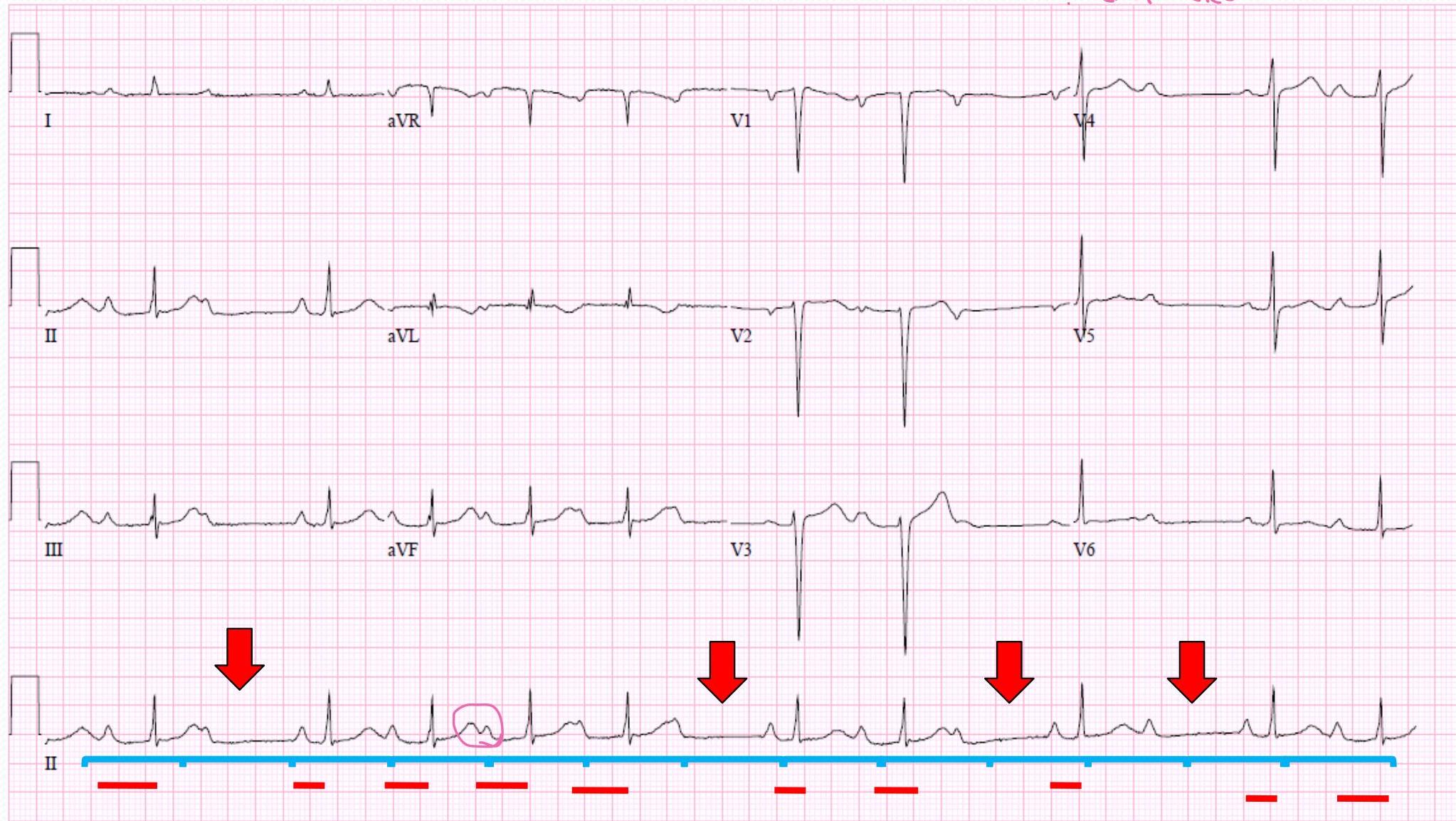
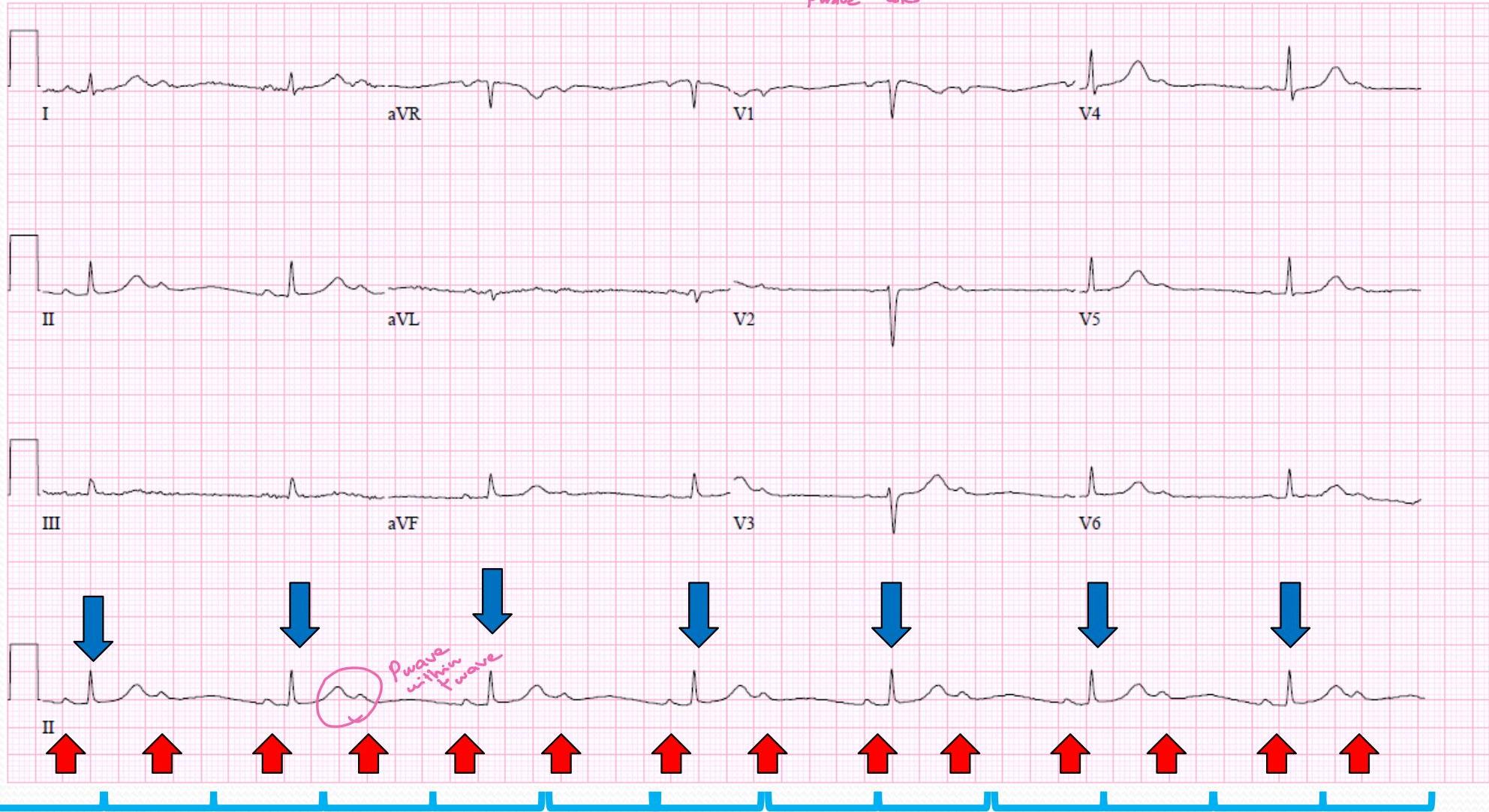
Atrial Flutter
- Saw tooth appearance
Causes:
- myocarditis
- IHD
- Cardiomyopathy
- caffiene?
- energy drinks?
Treatment:
- tft: Cardioversion or medications
- Close 1 out: Artylbric
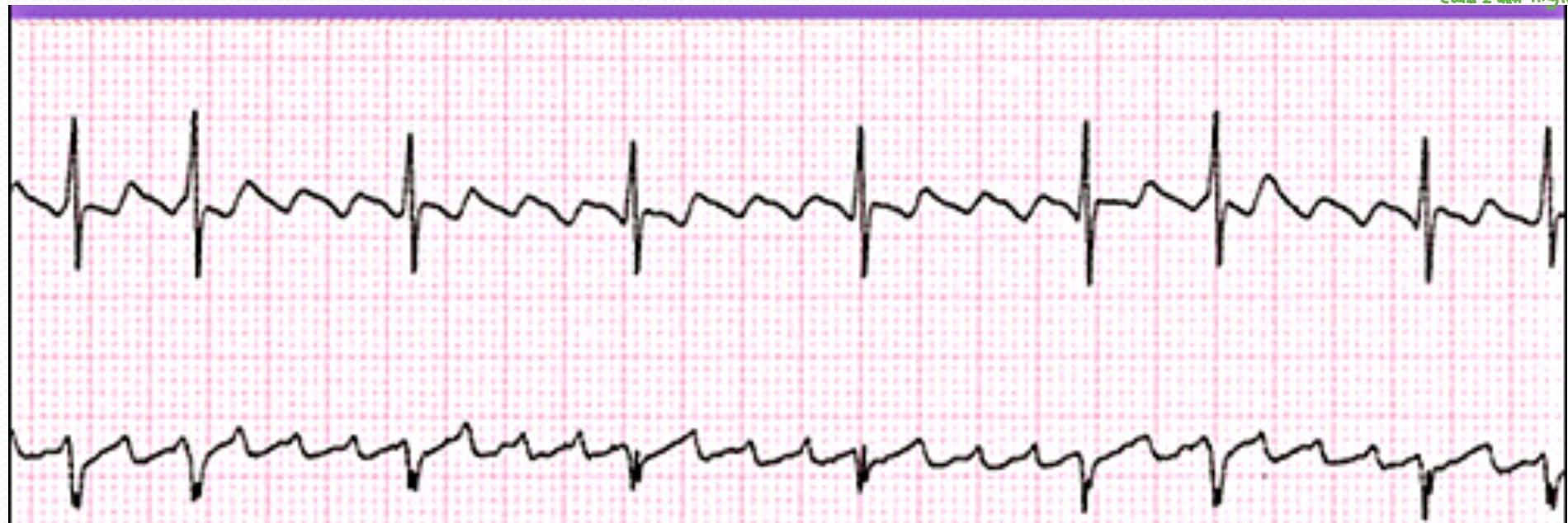
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| A: 220-430 bpm | Regular or variable | Sawtoothed appearance | N/A | <.12 |
| V: <300 bpm |
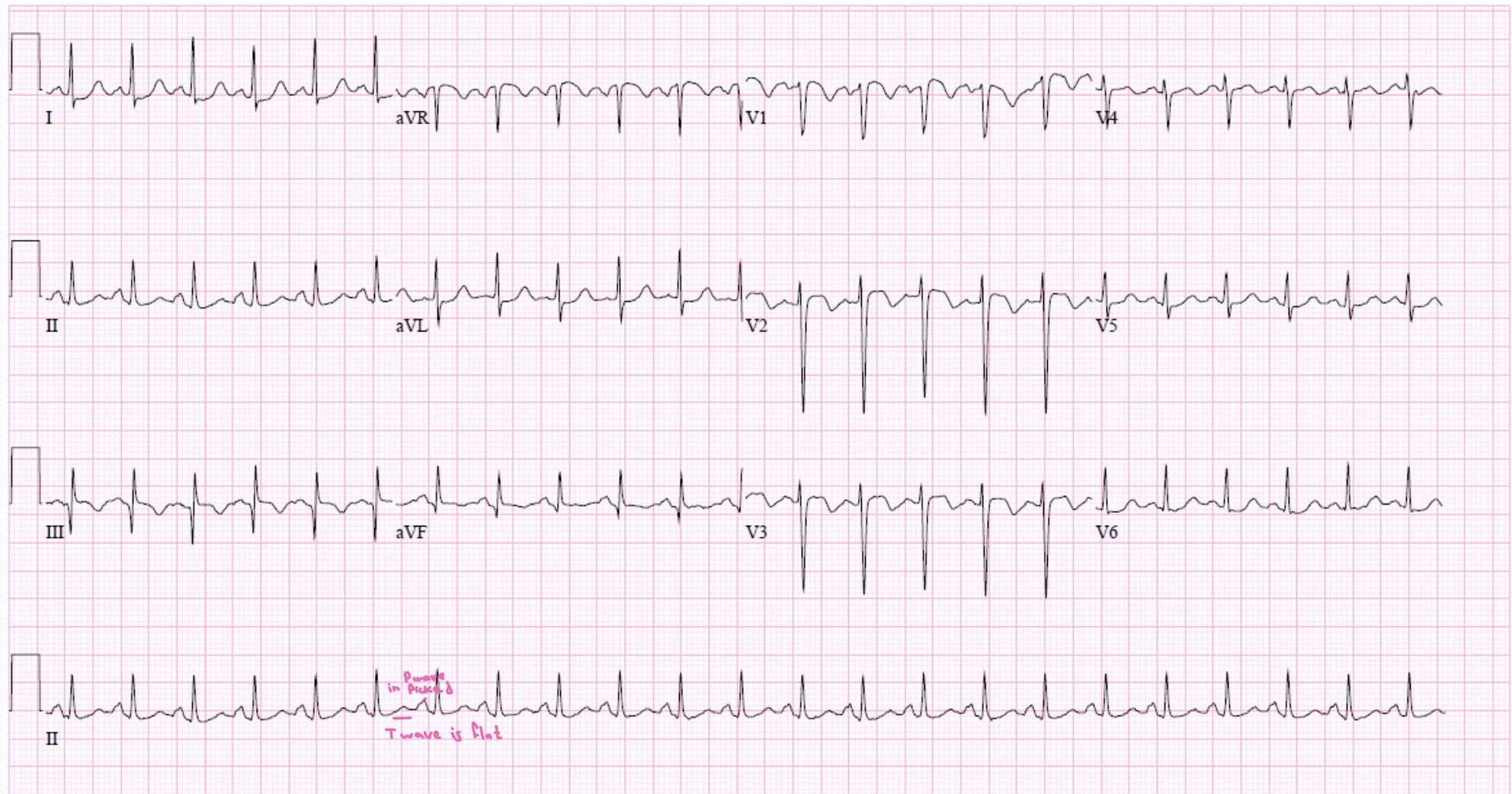
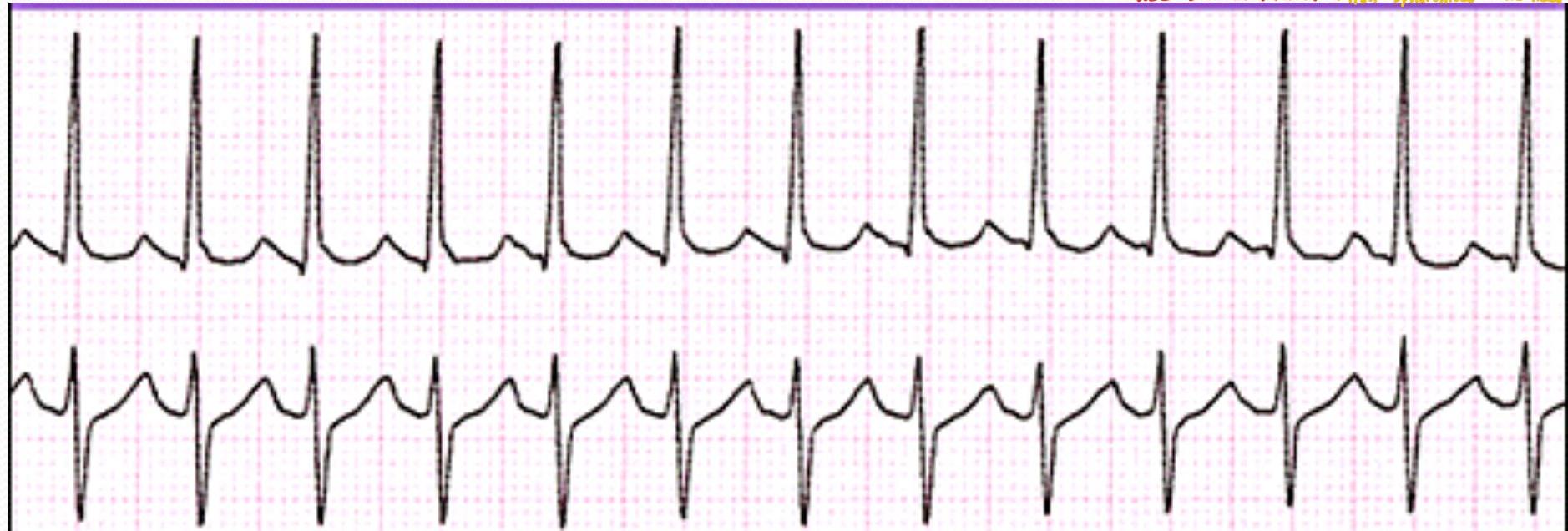
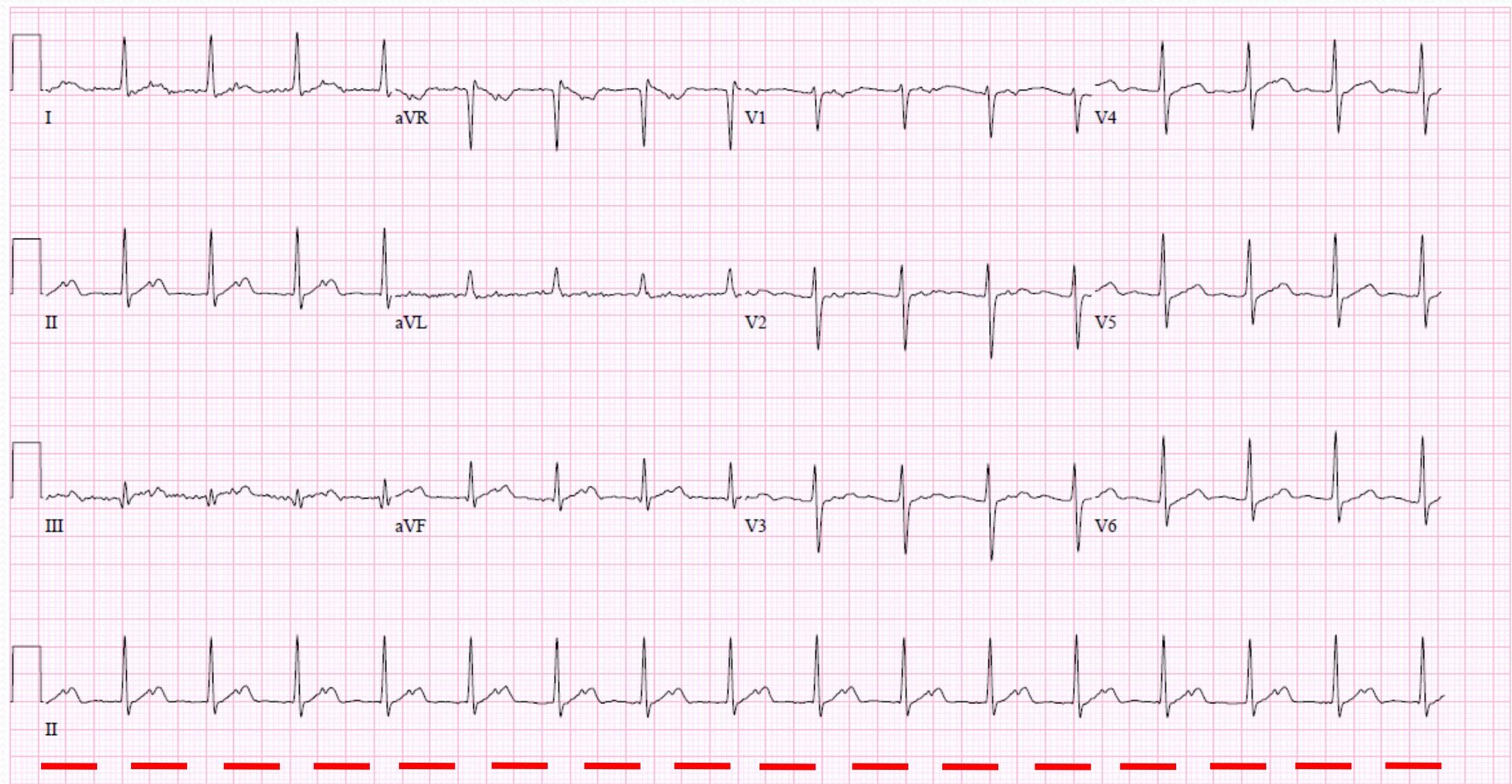
Atrial Fibrillation
Causes:
- myocarditis
- IHD
- Myopathy
- (in adult associate with mixed stenosis & chronic) / in children usually acute
Treatment:
- Att: Anti-Hepatotic - BB / CCB to show down HR - Class 1 anti-amythmic
- work on ectopic focus
- (att: Cardioresistance of medications class 1 anti-amythmic)
| I | aVR | V1 | V4 |
|---|---|---|---|
| II | aVL | V2 | V5 |
| III | aVF | V3 | V6 |
| II | only shaking no contraction |
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| A: 350-650 bpm | Irregular | Fibrillatory (fine to course) | N/A | <.12 |
| V: Slow to rapid |
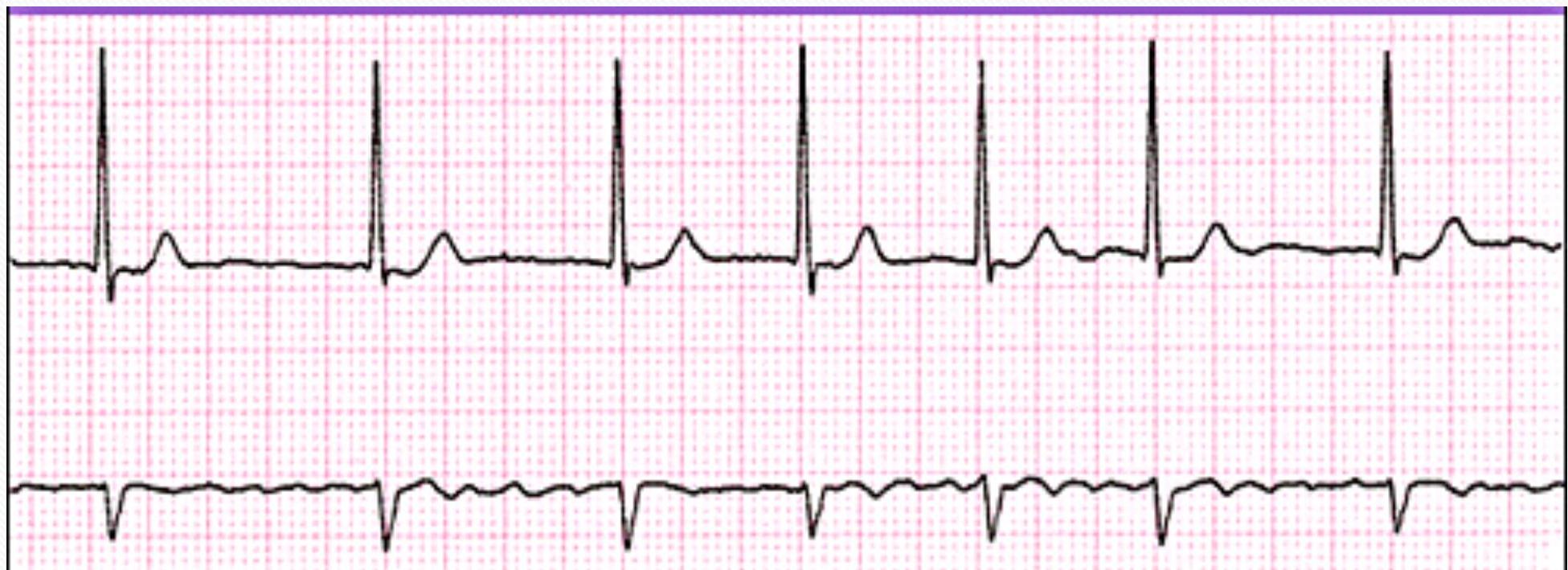
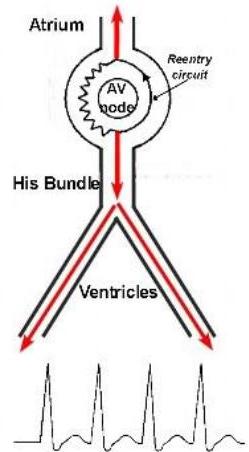
Paroxysmal Supraventricular Tachycardia (SVT)
(AV nodal reentrant tachycardia)

Causes:
- WBW Syndrom
- ectopic focus
- IHD - Cardiomyopathy
- myocarditis
- sepsis
(Paroxismal SVT / AVNRT):
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| 140-250 bpm | Regular | Abnormal P before each QRS (difficult to see) | <.20 | <.12 |
TABLE 2. Clinical Signs and Symptoms Associated With Sinus Tachycardia and SVT
| Sinus Tachycardia | SVT | |
|---|---|---|
| Heart rate (bpm) | Infants, below 220 Children, below 180 | Infants, above 220 Children, above 180 |
| Beat-to-beat interval | Variable | Fixed |
| P waves | Visible; normal axis | Not visible or abnormal axis Usually hidden in QRS or ST segment |
| Onset | Gradual | Abrupt |
| Termination | Gradual | Abrupt |
| Response to vagal maneuvers | Rate slows gradually, then returns | Tachycardia terminates abruptly (if successful) |
| Response to cardioversion | No conversion | Conversion |
| Fever | Strongly suspected when fever is present | 2%-3% of patients have fever on presentation |
| Presentation with shock | Possible | Possible |
treatment
- Tet:
- Valsava manuver
- Cold shower
- Carotid massage
- Blocker
- more frequent you can use BB
- at hospital:
- Adenosin is pit not in shock
- & in shock: shock / Cardioverison “sponsorized” need sedation
- The only 2 cases that we can use Debiritalium
AV Blocks
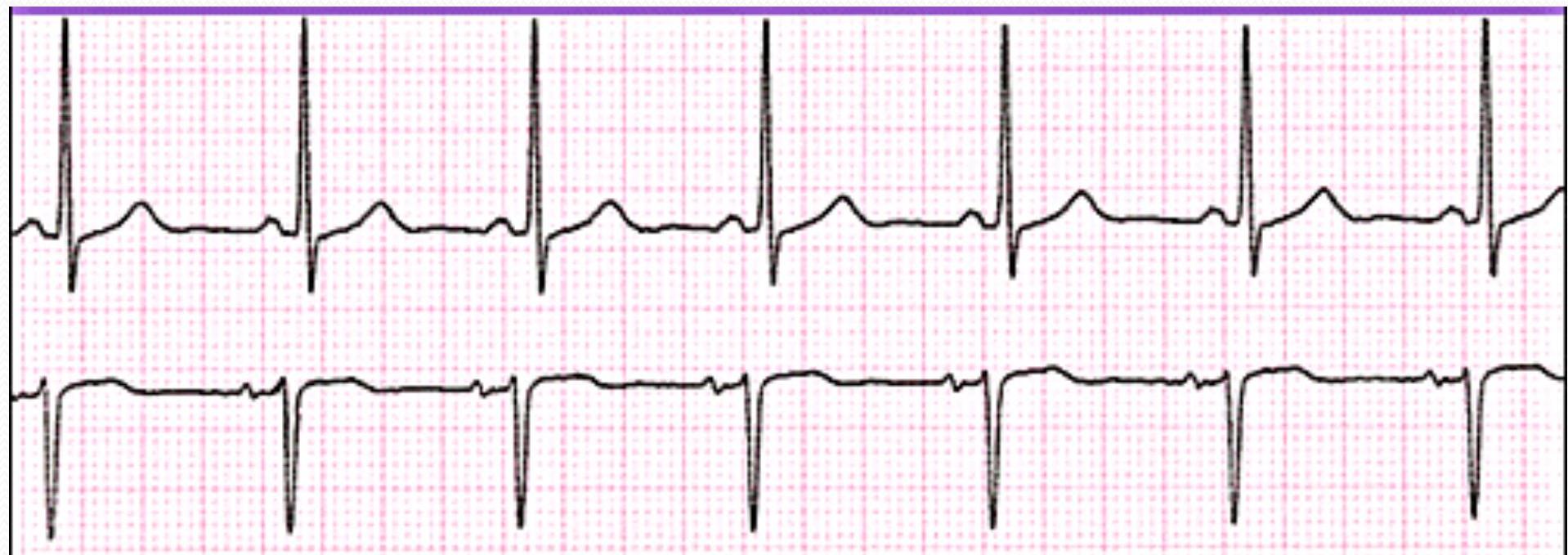
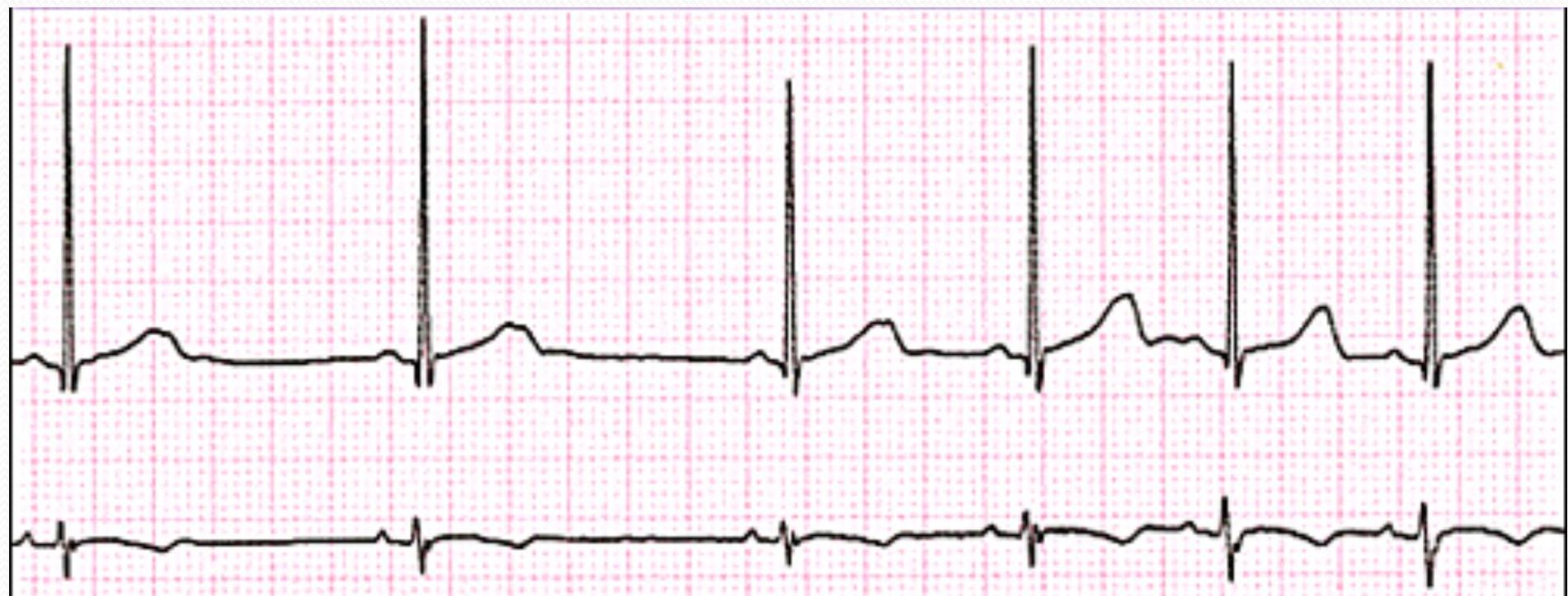
First Degree AV Block
- Regular
- Prolong QR interview
Causes:
- could be normal in children
- Rheumatic fever
- hypokalemia, hypocalcemia
- IHD
Second Degree AV Block (Type I / Wenckebach)
- same causes ↑
- Progressive Prolongation PR interval
- VA: B agnisf
- Atropin
- Dopamin
| P Wave | PR Interval (in seconds) | QRS (in seconds) | Characteristics |
|---|---|---|---|
| Conduction intermittent | Increasingly Prolonged | <.12 | QRS dropped in a repeating pattern |
Second Degree AV Block (Type II)
- 197: B agent
- Atropin
- Dopamin
- Block 2:1
- Person aR
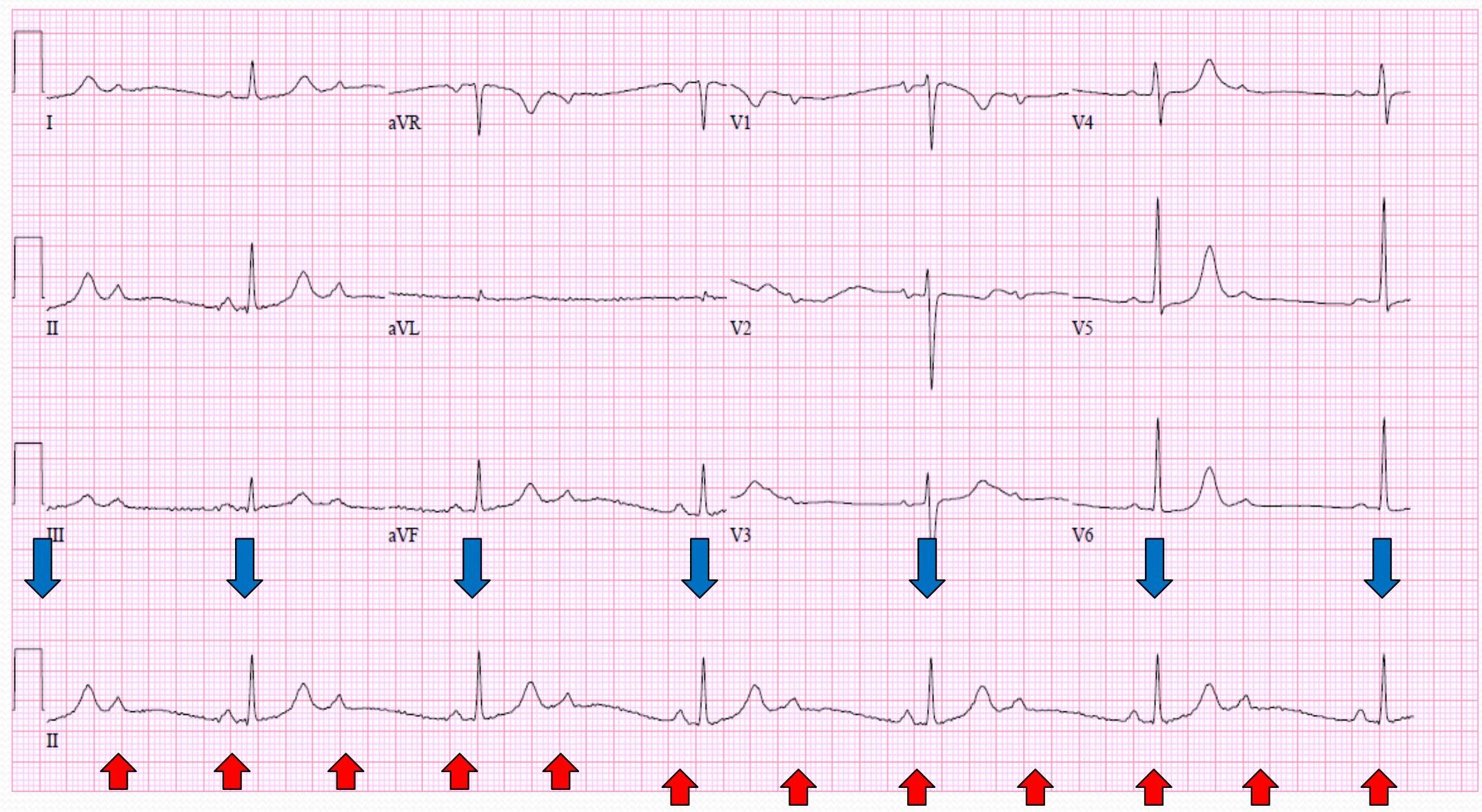
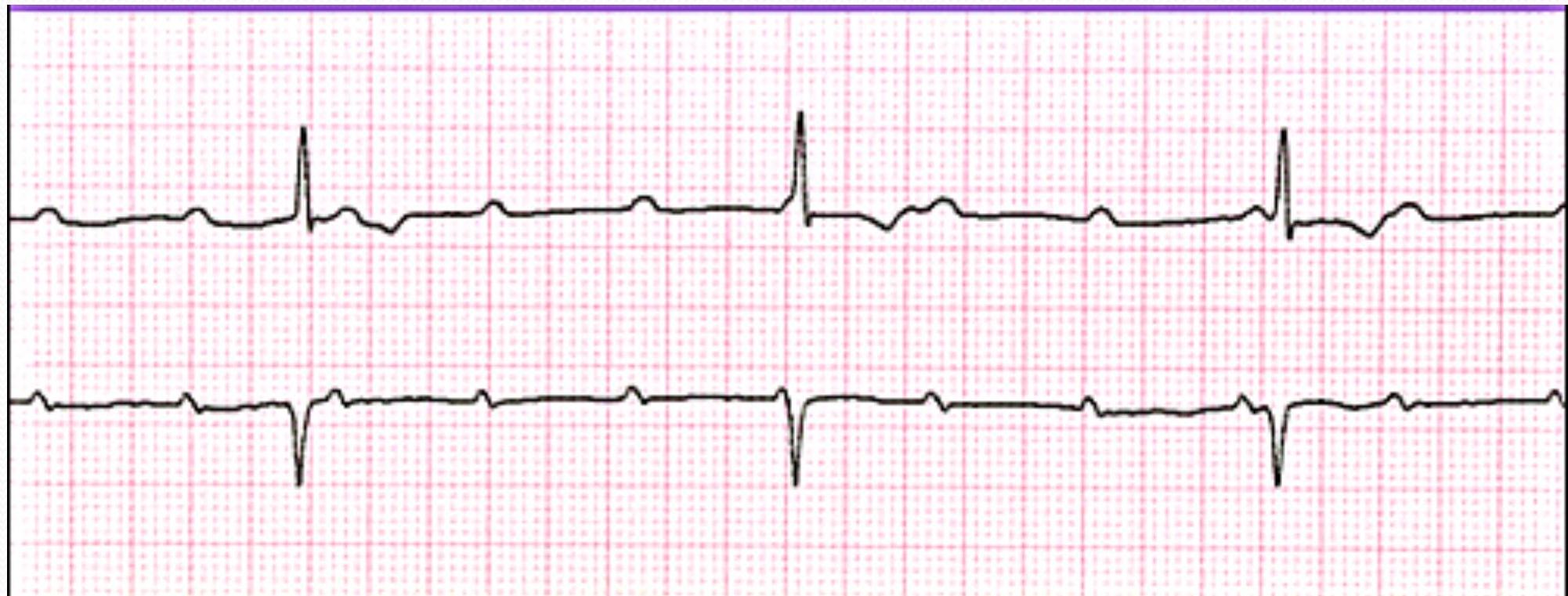
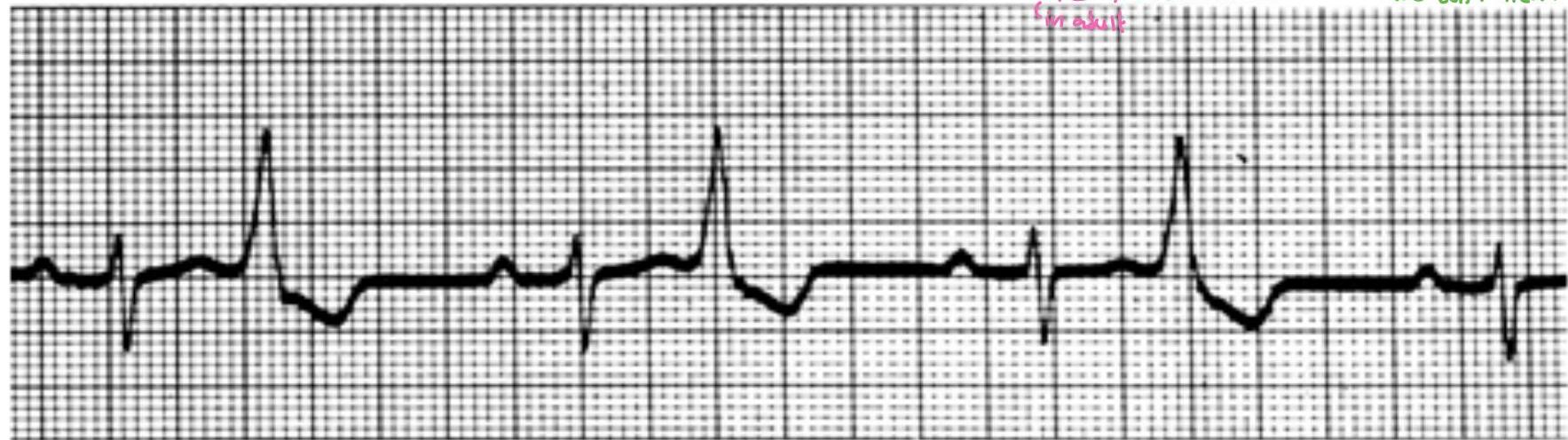
Third Degree AV Block (Complete Heart Block)
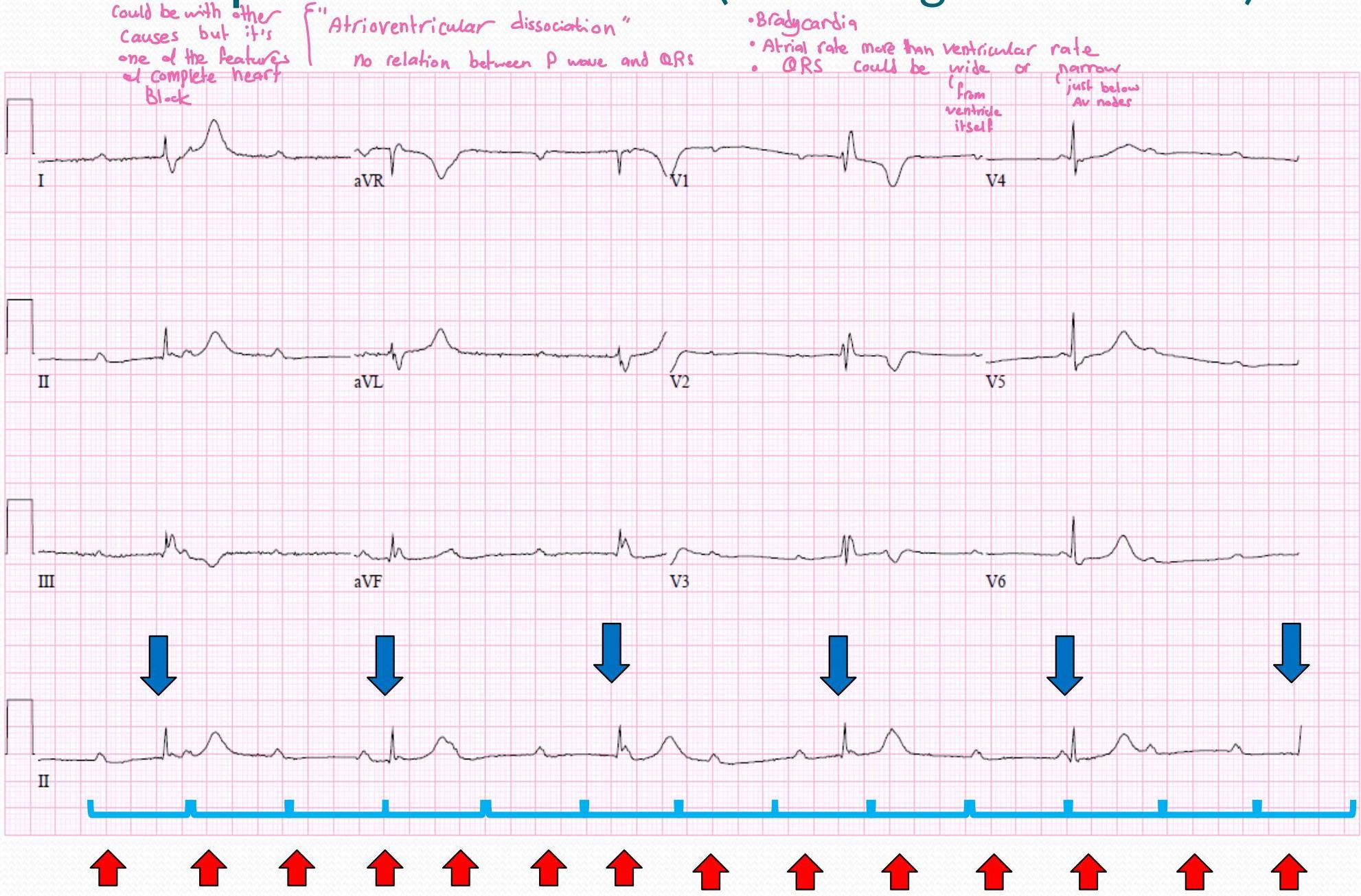
- could be with other causes but it’s one of the features of complete heart block
- “Atrioventricular dissociation” no relation between P wave and QRS
- Bradycardia
- Atrial rate more than ventricular rate
- QRS could be wide or narrow (from ventricle itself, just below AV nodes)
Causes:
- SLE in the mother antibodies will skip the placenta
- Rheumatic Carbitis
- IHD
- Digitalis
Treatment:
- ett: Race maker
| P Wave | PR Interval (in seconds) | QRS (in seconds) | Characteristics |
|---|---|---|---|
| Normal but not related to QRS | None | N/A | No relationship between P&RS |
Ventricular Arrhythmias
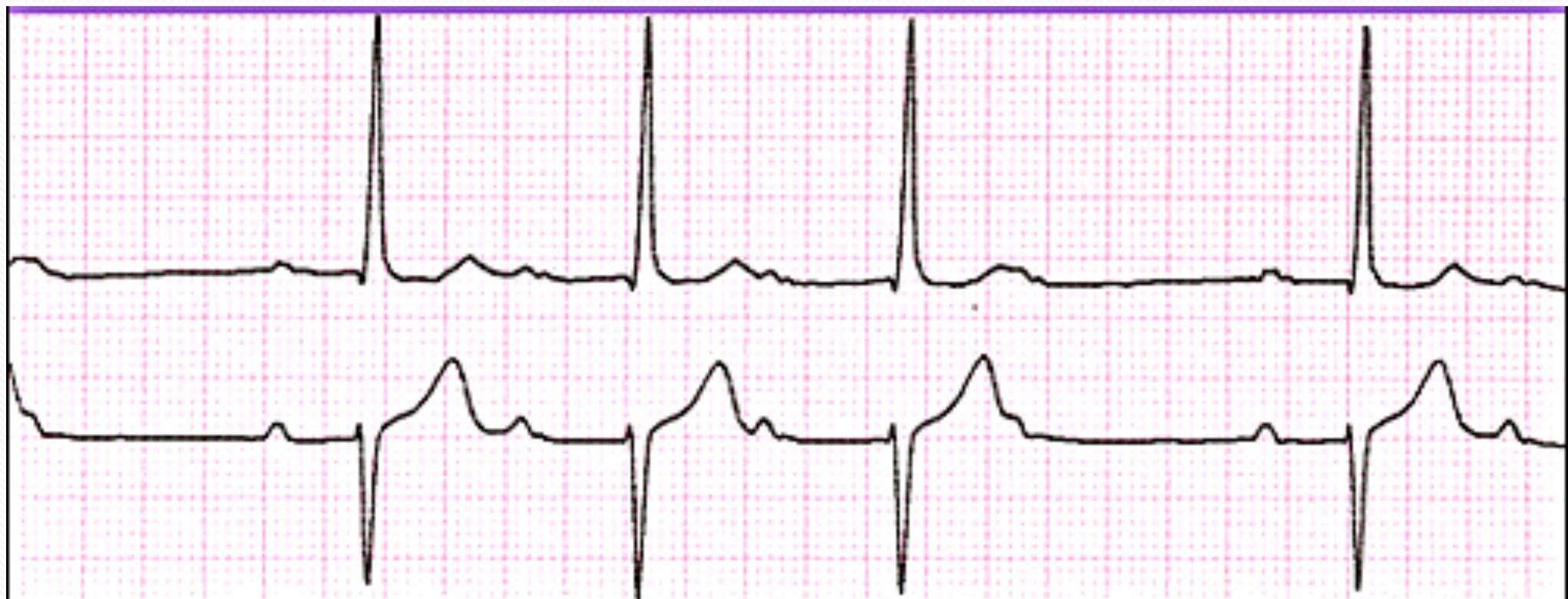
Premature Ventricular Contractions (PVCs) Y
Bigeminal Pattern
- 1:1
- no P wave
- wide QRS coming from ventricle
- “Regularly Irregular” Rhythm
- How to pick PVC clinically: Drop Pests
Causes:
- IHD, coffee, tea
- we don’t treat
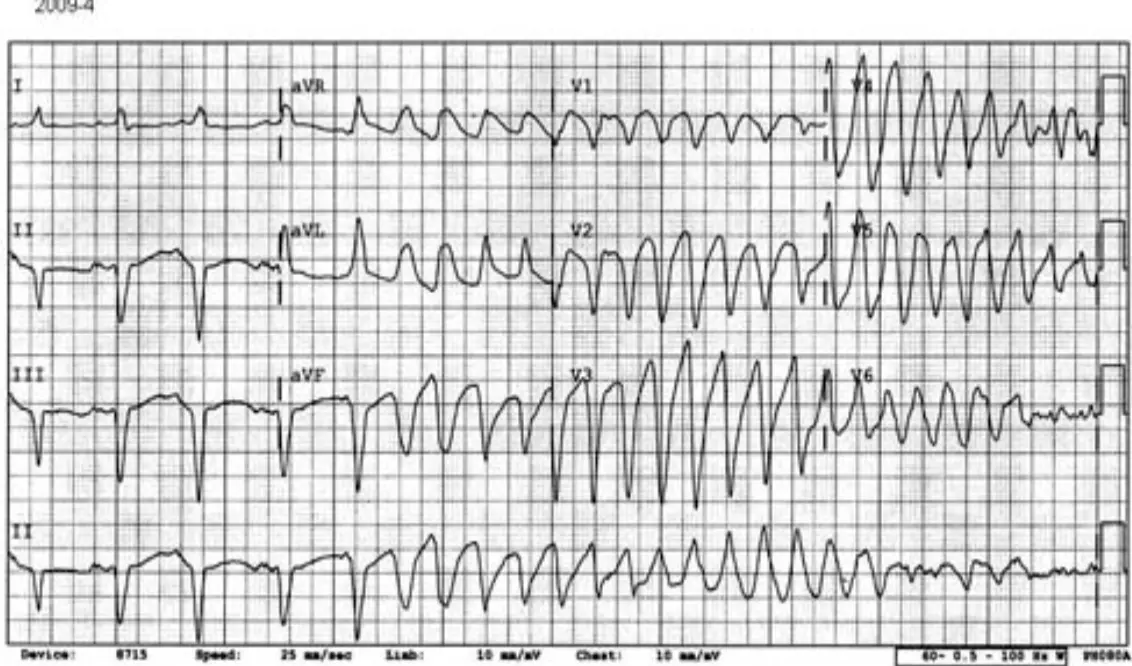
Ventricular Tachycardia (VT)
What do you notice?
- no Pwowe
- wide QRS → v Tach
- monomorphic
- Rates range from 100-250 beats/min
- Non-sustained or sustained
- P waves often dissociated (as seen here)
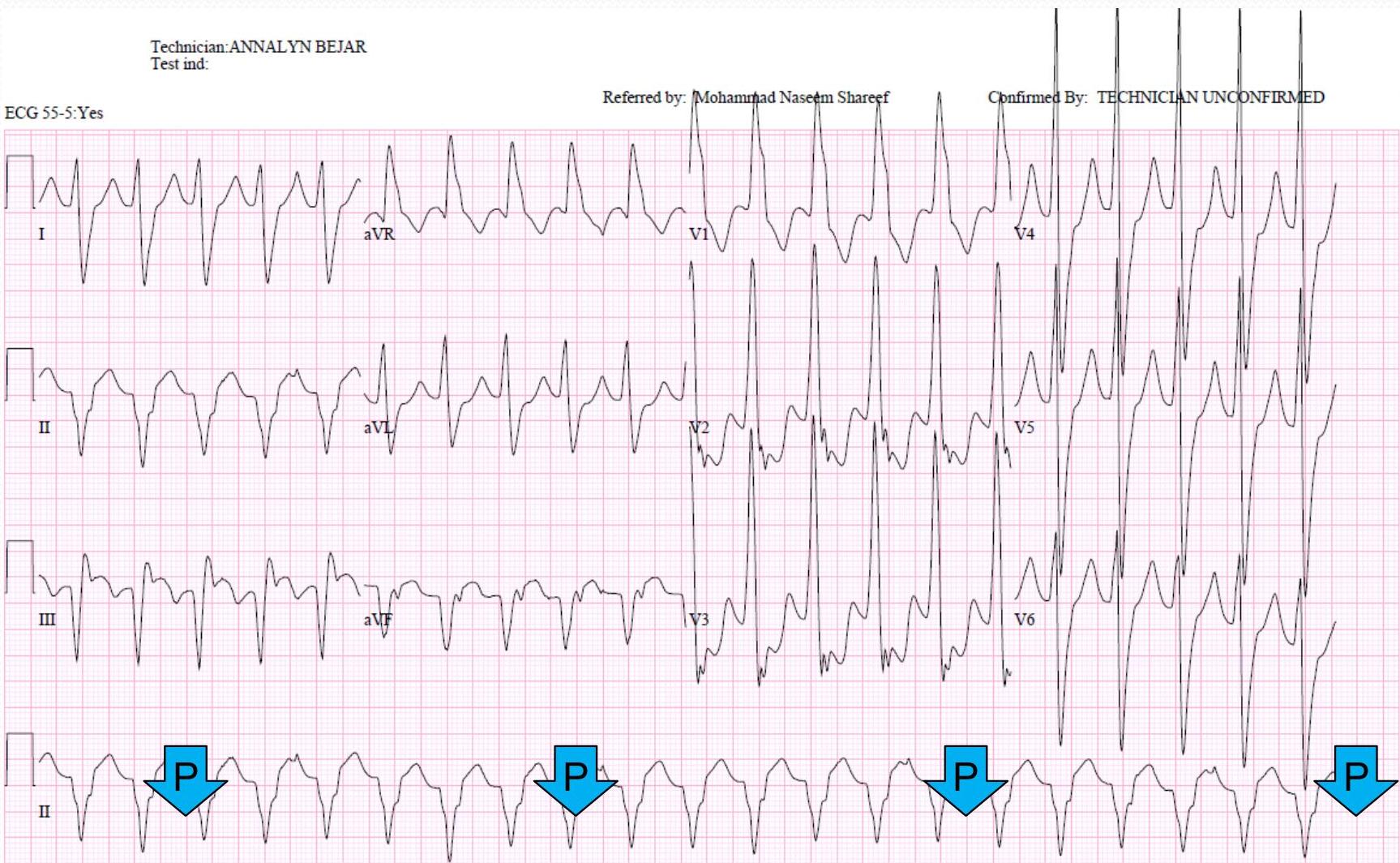
Monomorphic VT
What is the mechanism?
Treatment:
- ekt: Amidoron → IV line in lcu pn
- still more: Puls → cardioversion
- no Puls → defib
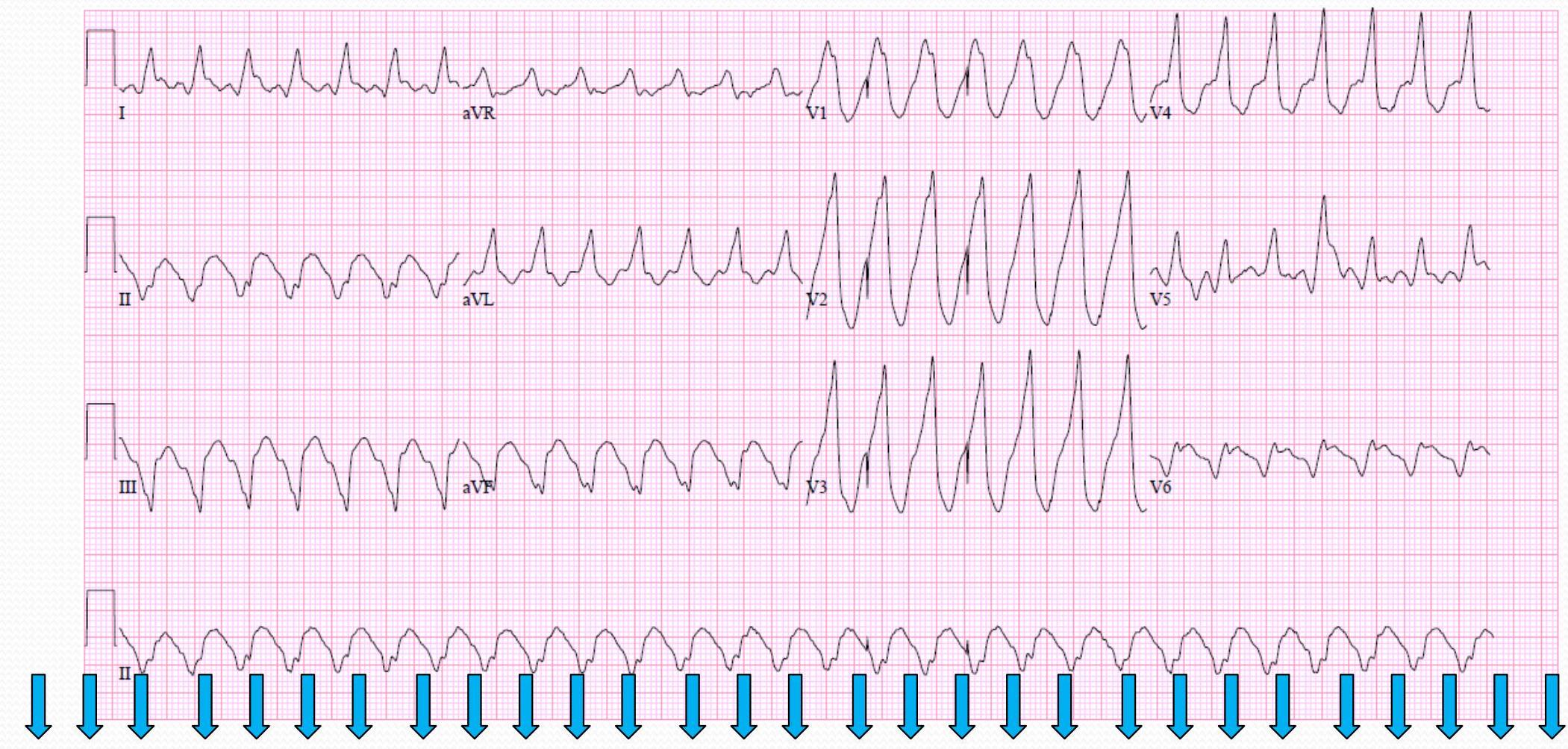
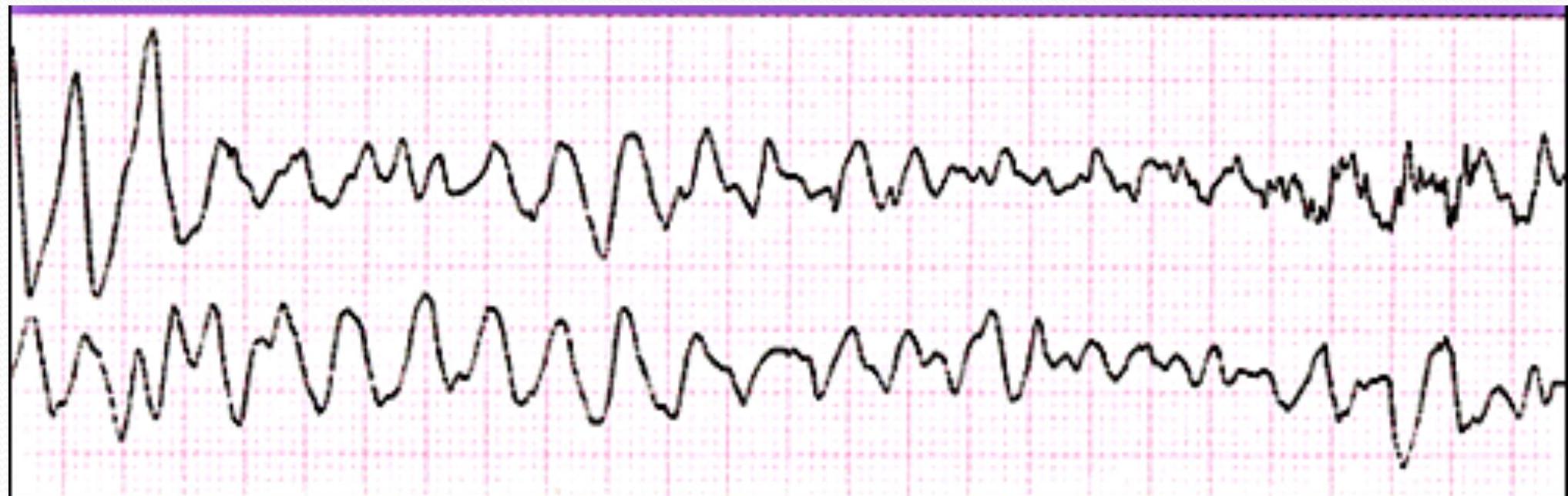
Polymorphic VT
What is the mechanism?
- no P wave
- wide QRS
 25mm/s 10mm/mV 40Hz 005C 12SL 231 CID: 10
EID:40 EDT: 08:41 03-NOV-2004 ORDER:
25mm/s 10mm/mV 40Hz 005C 12SL 231 CID: 10
EID:40 EDT: 08:41 03-NOV-2004 ORDER:
True side Point
- xtt: Mg Sulfate
- aller trail of
- Carbination
- Polymorphic V each
Ventricular Fibrillation
Treatment:
- ett:
- ICU for any resone - Amidaron → IV Line in ICU PIR
- ER
- still there’s Puls → Carbioversion
- no Puls → Defibrillation
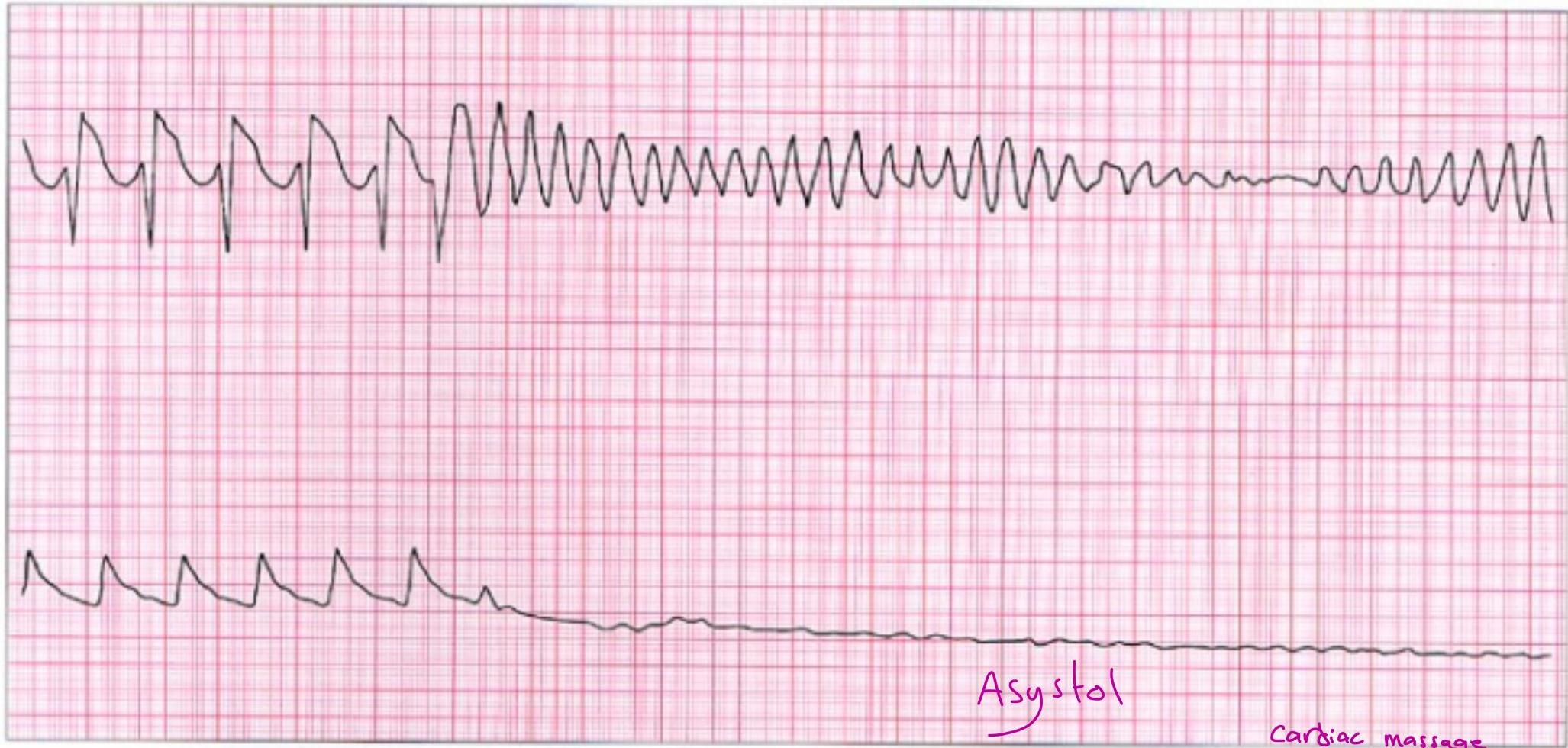
| Heart Rate | Rhythm | P Wave | PR interval (in seconds) | QRS (in seconds) |
|---|---|---|---|---|
| 300-600 | Extremely irregular | Absent | N/A | Fibrillatory baseline |
Asystole
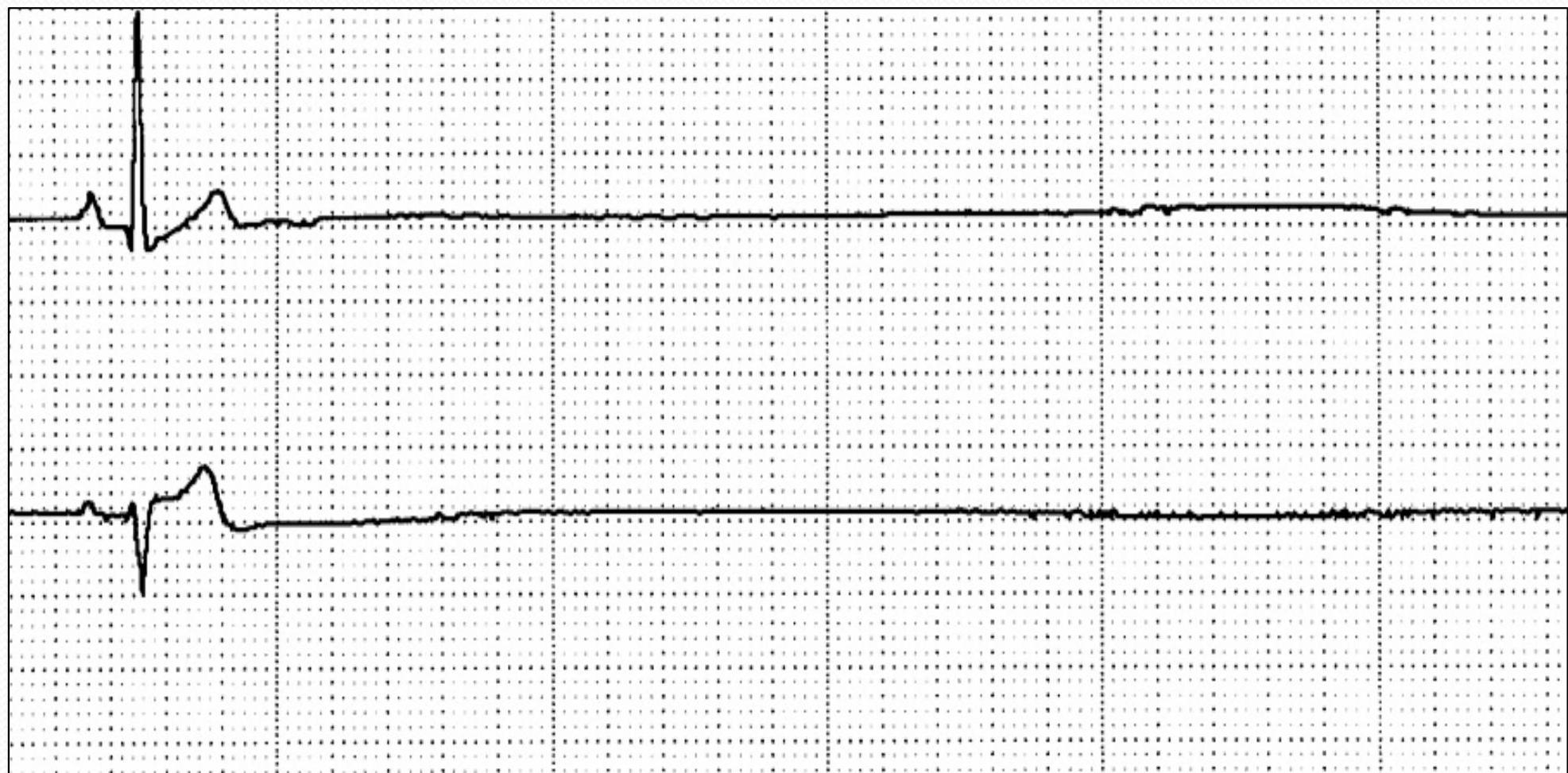
Syndromes
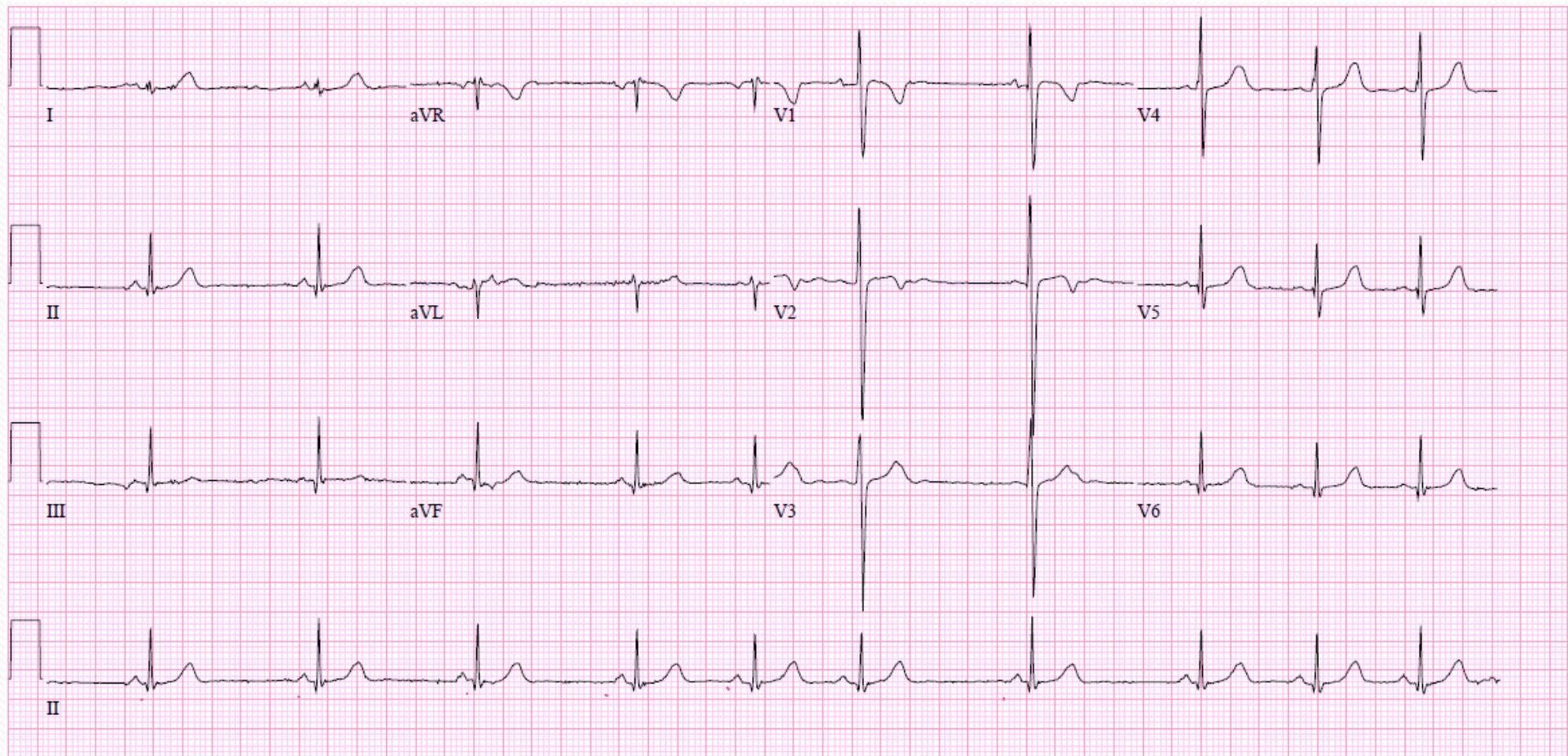
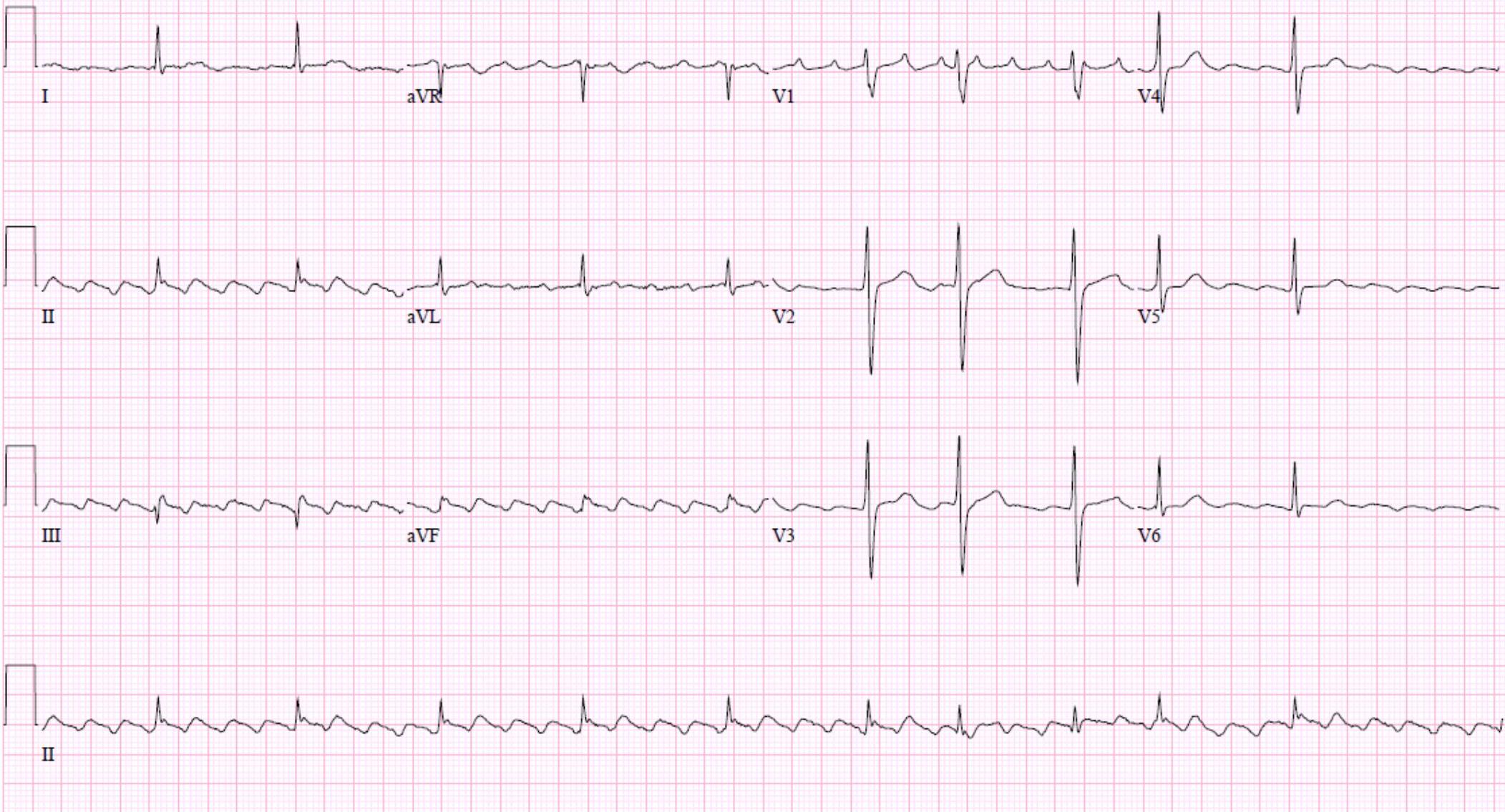
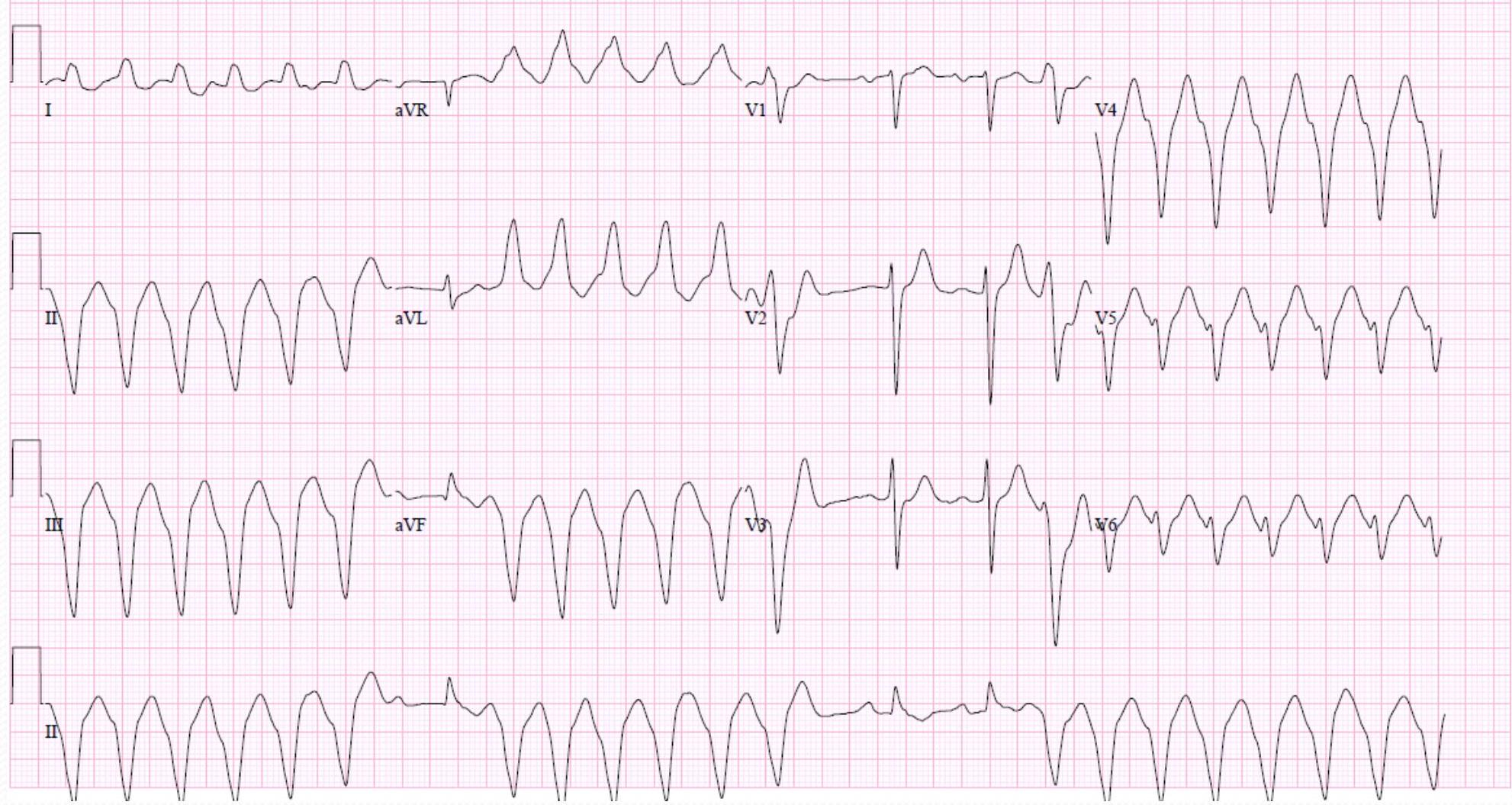
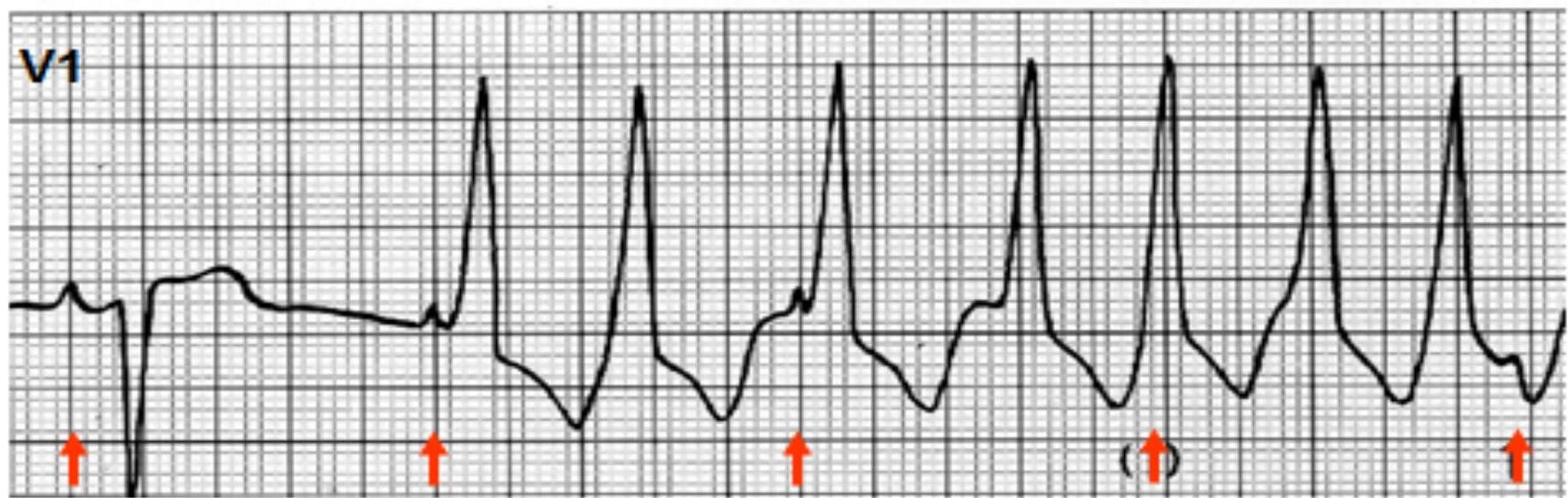
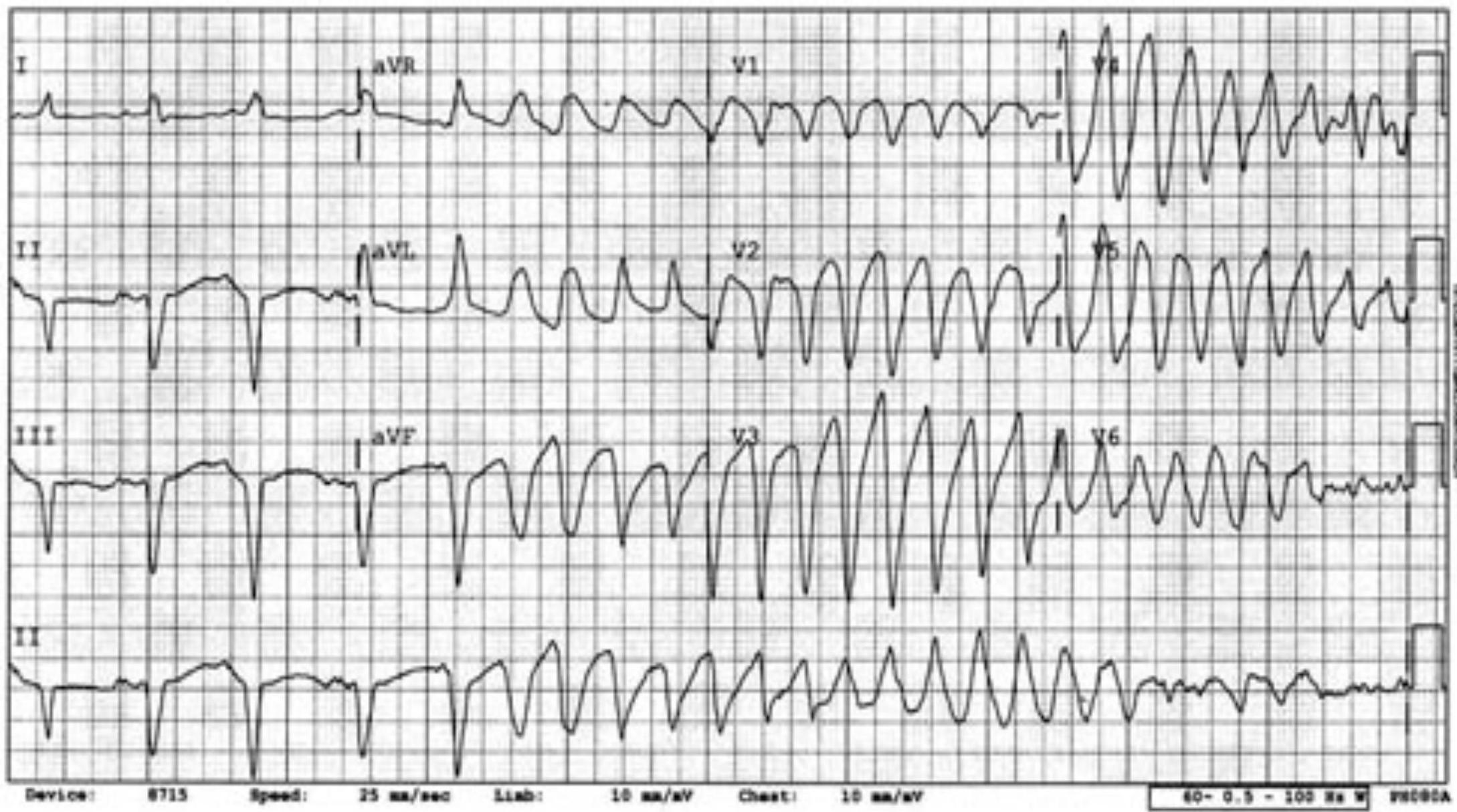
Brugada Syndrome
- 12-lead electrocardiogram (ECG) from a patient with the Brugada syndrome shows downsloping ST elevation
- V tachycardia
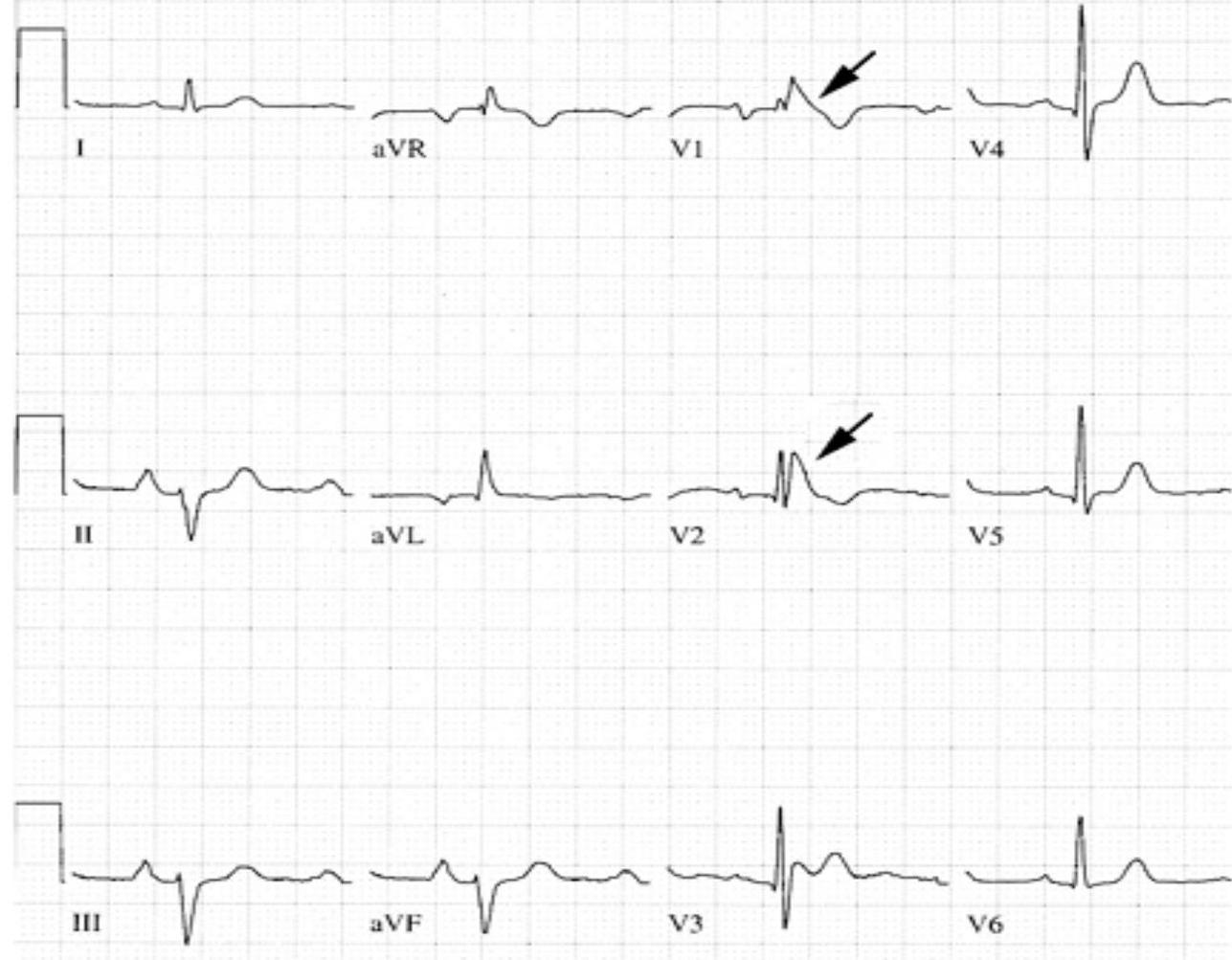
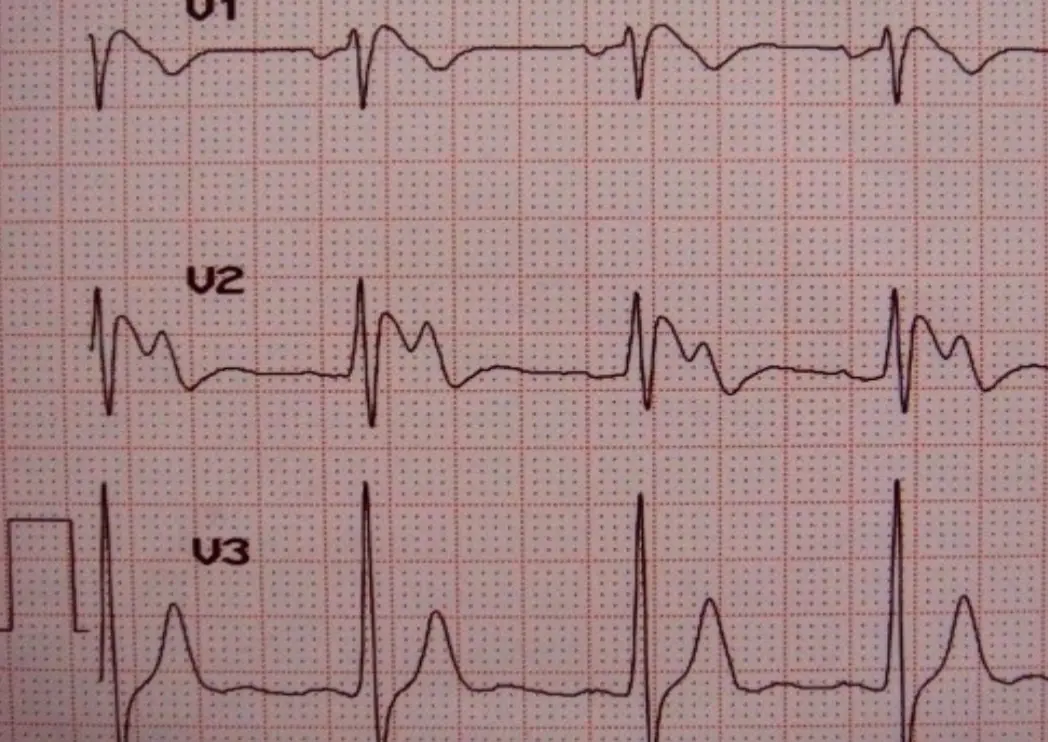
- ST segment elevation and T wave inversion in the right precordial leads V1 and V2 (arrows); the QRS is normal. The widened S wave in the left lateral leads (V5 and V6) that is characteristic of right bundle branch block is absent.
- Courtesy of Dr Rory Childers, University of Chicago.
- UpToDate
 Loc 55545-5000 25 mm/sec 10.0 mm/mV - W 0.50-40
Loc 55545-5000 25 mm/sec 10.0 mm/mV - W 0.50-40
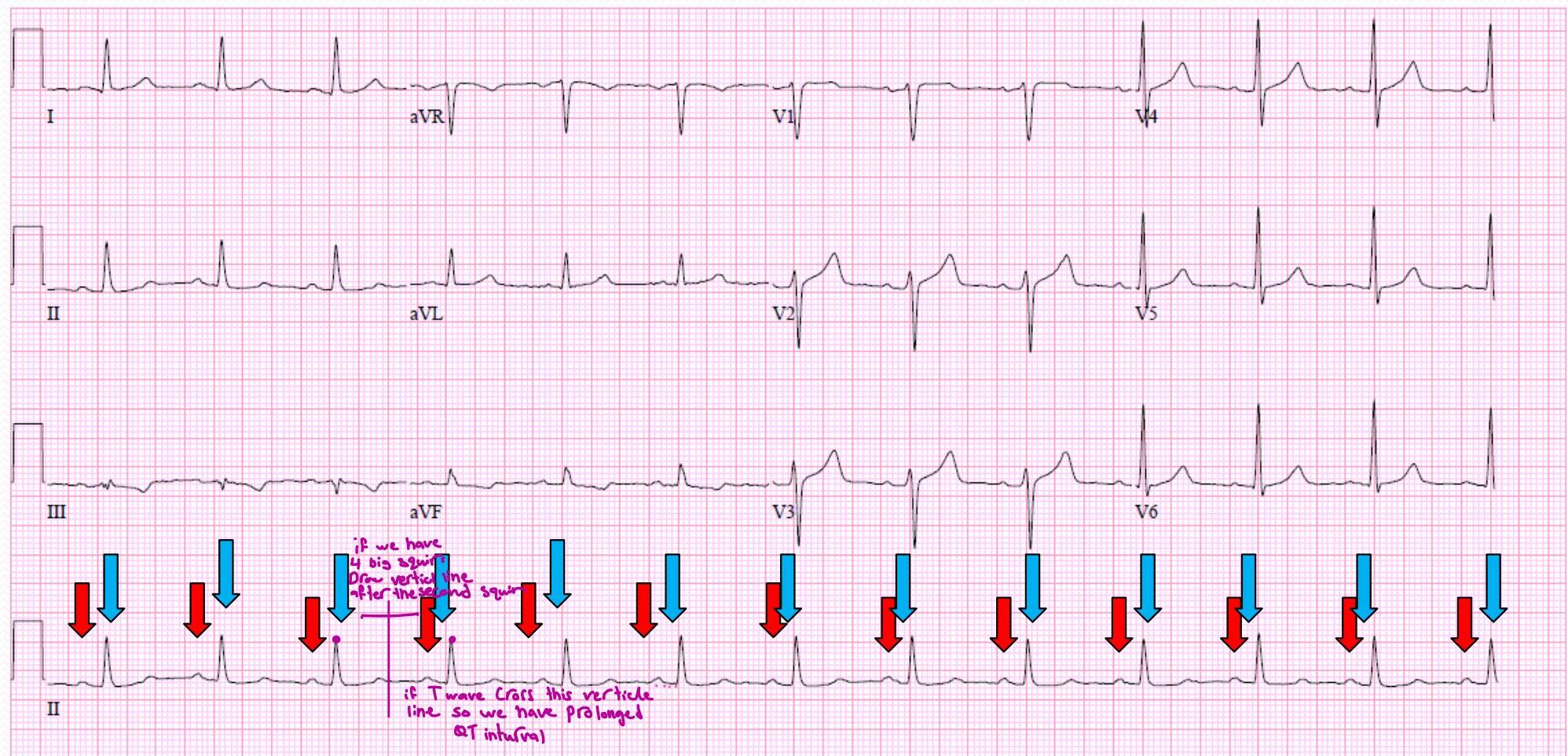
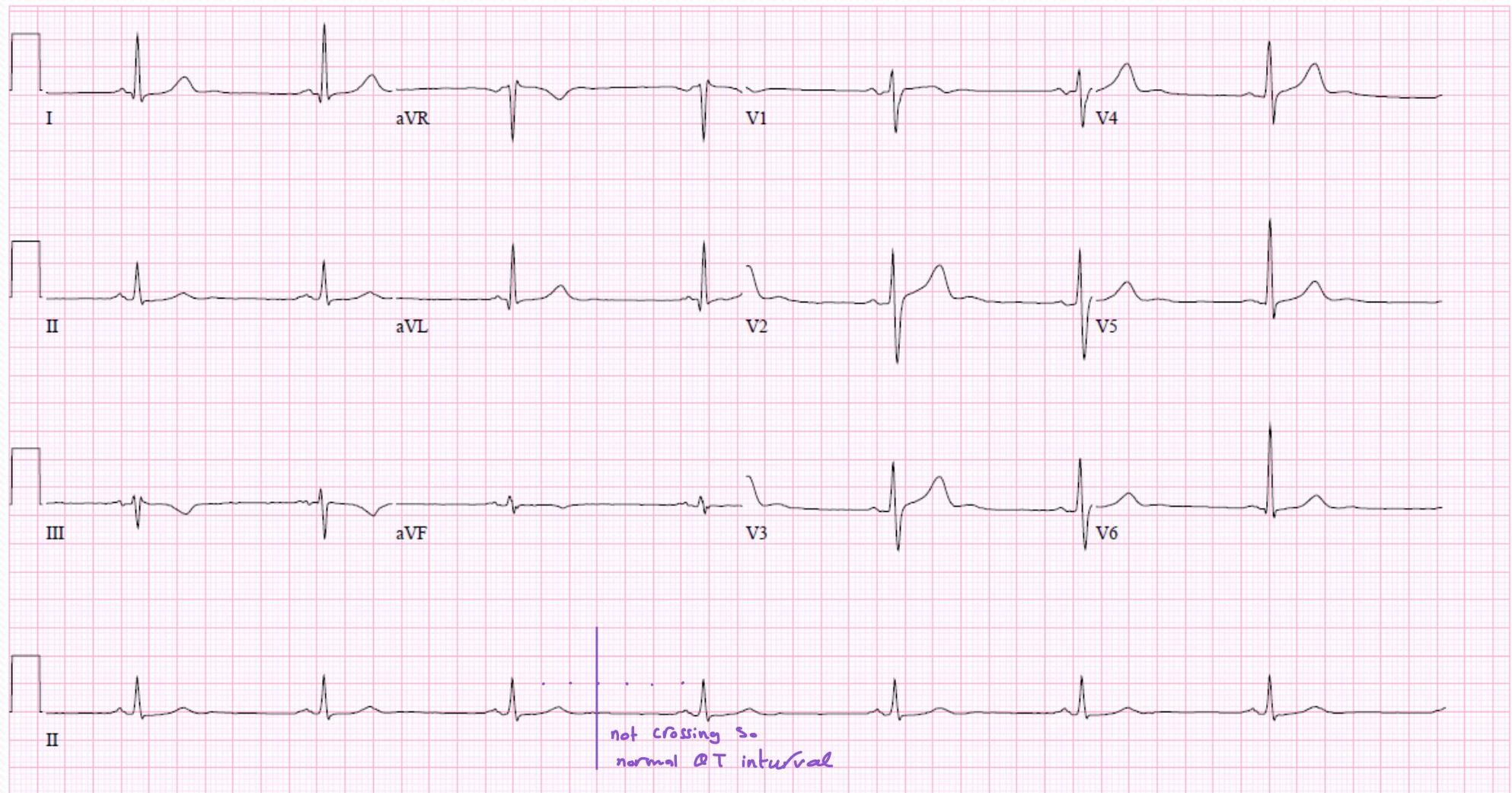
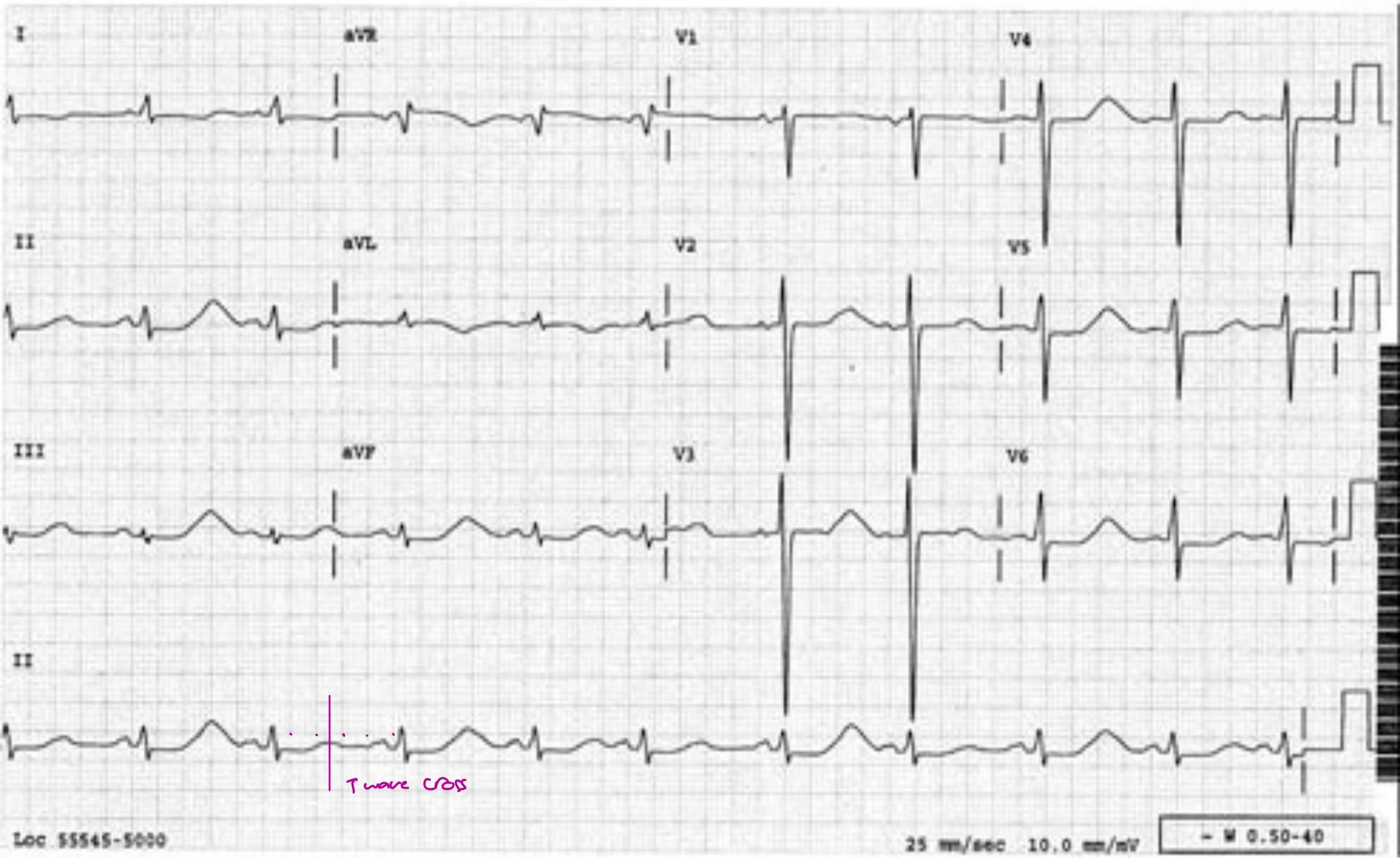
Long QT Syndrome (Jervell-Nielson-Lange)
Causes:
- hypothyroidism
- ↓ mg⁺ ↓ Ca⁺ ↓ Na⁺
- macrolides “Erythromycin”
- Glucosamine “sokimalarina”
Congenital:
- ↓ subba Death
- ↓ Definess
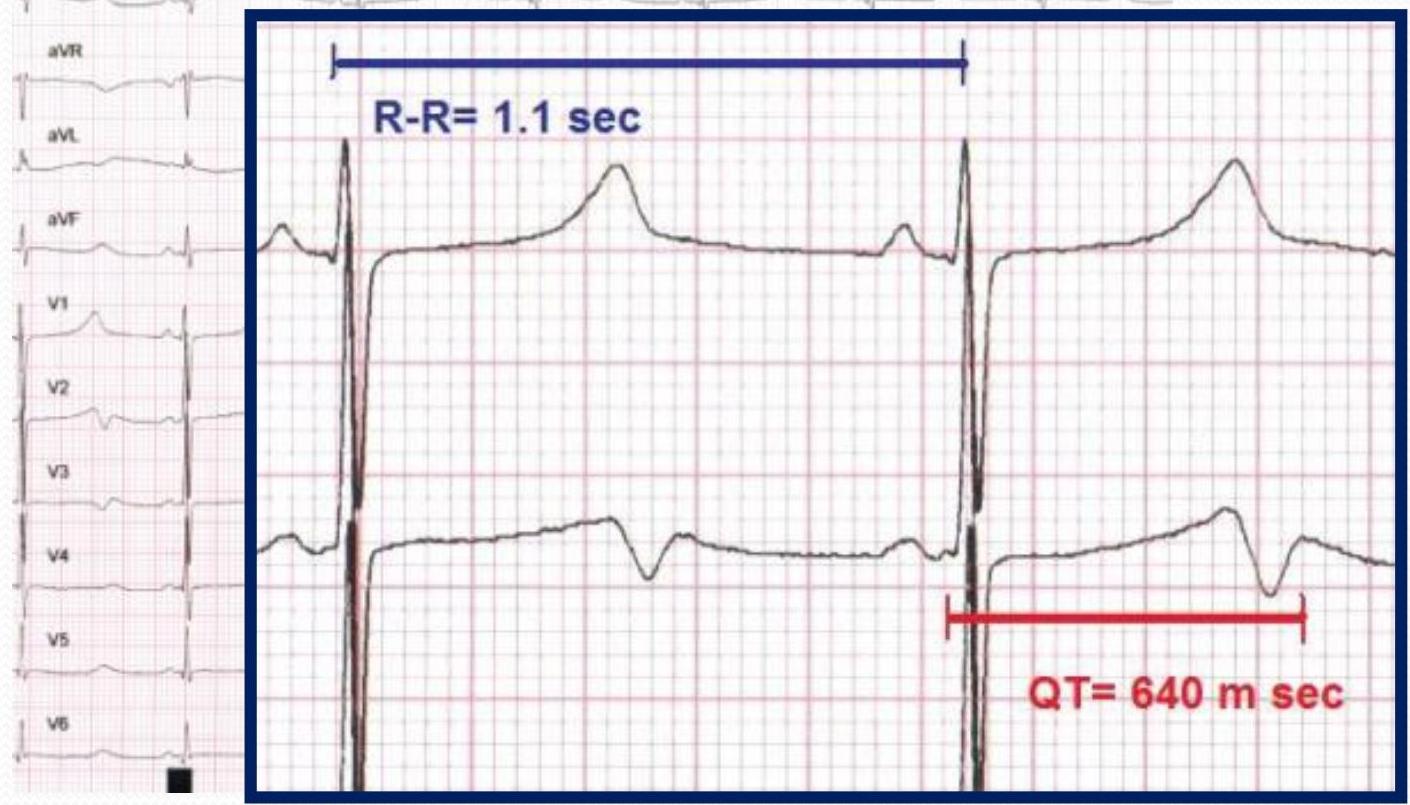
**QT
(sec)
- significant
-
450 m sec is
Wolff-Parkinson-White (WPW) Syndrome
- WBW
-
- wide QRS
- -delta wave
- short P-R interval




Complications:
- SVT
- V each in adult
Treatment:
- Lift: if SVT treat it as SVT
- if recurrent * electrophysiotherapest * if persistent (burn the exercise electrical focus
Tores de pointes
Management
Arrhythmia Management
Aim:
- Hemodynamic stability
- Prevent complications
- Symptomatic relief
Strategies:
- Restoration of normal rhythm
- Slowing of tachyarrhythmia
- Augmenting the slow rhythm
Options:
- Pharmacological agents
- Electrical cardioversion
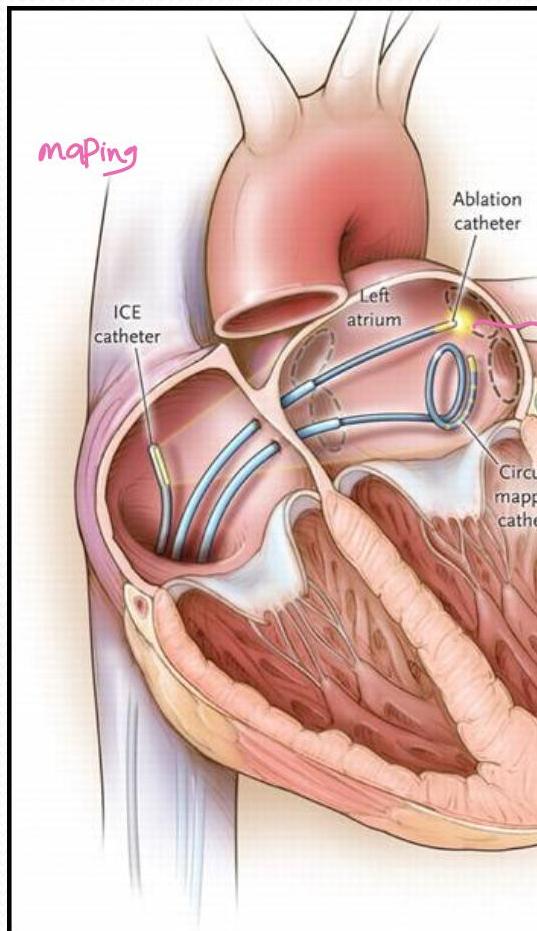
- Transcatheter ablation
- Device implantation
Logistics:
- Emergency versus elective management
- Electrophysiology lab
Emergency Cardioversion



وفي أنفسِكُمْ آفَلا تَجِدُونَ