Brief Resolved Unexplained Event (BRUE) / Apparent Life-Threatening Event (ALTE)
Brief resolved unexplained event (BRUE) is an event that occurs in infants younger than one year of age.
Definition
☐ Definition:
A BRUE includes the following characteristics:
- The infant stops breathing, has a change in muscle tone, turns pale or blue in color, or is unresponsive.
- The event occurs suddenly, lasts less than 30 to 60 seconds, and is frightening to the person caring for the infant.
- BRUE is present only when there is no explanation for the event after a thorough history and exam.
Events Which Are NOT BRUE
The following conditions and circumstances are NOT considered BRUE:
- Reflux after eating
- Severe infections (such as bronchiolitis, whooping cough)
- Birth defects that involve the face, throat, or neck
- Birth defects of the heart or lungs
- Allergic reactions
- A brain, nerve, or muscle disorder
- Child abuse
- Certain uncommon genetic disorders
Important Notes:
- A specific cause of the event is found in 50% of cases.
- In healthy children who only have one event, the cause is rarely identified.
Risk Factors for BRUE
The following factors increase the risk of BRUE:
- A prior episode when the child stopped breathing, turned pale or blue
- Feeding problems
- Recent URTI or bronchitis
- Age younger than 10 weeks
- Low birth weight
- Premature baby
- Secondhand smoke exposure
Symptoms of BRUE
These events are more likely to occur during the first two months of life and between 8 a.m. and 8 p.m.
A BRUE includes one or more of the following:
- Breathing changes — either no effort at breathing, breathing with great difficulty, or decreased breathing
- Color change — most often blue or pale (many infants turn red when crying, for example, so this does not indicate a BRUE)
- Change in muscle tone — most often they are limp, but they may become rigid
- Change in level of responsiveness
Note: Choking or gagging means the event was likely not a BRUE. These symptoms are more likely caused by reflux.
History
When evaluating a BRUE, the following historical elements are important to obtain:
- Other events like this one in the past
- Other known medical problems
- Medicines, herbs, or vitamins the infant may be taking
- Other medicines at home the child could have taken
- Complications during pregnancy, labor, at birth, or prematurity
- Siblings who also had this type of event
- Illegal drugs or heavy alcohol use in the house
- Prior reports of abuse
Medical History
☐ The following items are considered in order to decide for more investigations:
- The type of event that occurred
- How severe the symptoms were
- What was going on right before the event
- Other health problems that are present or found on physical exam
Physical Examination
A thorough physical exam will be done, checking for:
- Signs of infection, trauma, or abuse
- Low oxygen level
- Abnormal heart sounds
- Signs of birth defects that involve the face, throat, or neck that may cause breathing problems
- Signs of abnormal brain function
Testing Guidelines:
- If there are no findings to suggest a high-risk BRUE, lab tests and imaging tests are often not needed.
- If choking or gasping occurred during feeding and the infant recovered quickly, more testing will often not needed.
Risk for Recurrence / Presence of a Serious Cause
Factors that suggest a higher risk for recurrence or the presence of a serious cause include:
- Infants under 2 months of age
- Being born at 32 weeks or earlier
- More than 1 event
- Episodes lasting longer than 1 minute
- CPR by a trained provider was needed
- Signs of child abuse
Investigations
For Low Risk Infants
- Complete blood count (CBC)
- Renal profile
- Hepatic profile
- Serum calcium, magnesium, electrolytes, blood sugar
- Chest x-ray
- ECG
For High Risk Infants
☐ In addition to the low-risk investigations, the following are indicated:
- Urine or blood screen to look for drugs or toxins
- Holter monitoring / Echocardiogram
- CT or MRI of the brain
- Test for Pertussis, RSV, chlamydia or other viral Pannal
- Laryngoscopy or bronchoscopy
- Sleep study
- X-rays of the bones looking for prior trauma
- Screening for different genetic disorders
Management
Outpatient Management
☐ If the event was brief, with no signs of breathing or heart problems, and corrected on its own, the child will likely not need admission.
Admission Criteria
☐ A child may be admitted if:
- The event included symptoms that indicate a more serious cause
- Suspected trauma or neglect
- Suspected poisoning
- The child appears unwell or is not thriving well
- Need to monitor or observe while feeding
- Concern over ability of parents to care for child
Management of Admitted Infant
For admitted infants, the following will be monitored:
- Vital Signs: HR, RR, BP, Oxygen Saturation, temperature, and cardiac rhythm
- Feeding Pattern: Observation for feeding pattern, respiratory pattern, sleeping, activity, seizures, cyanosis, pallor, etc.
- Parent-Infant Interaction: Observation for mother and infant interaction and mother’s care of the infant
Home Care
Safe Sleep Recommendations
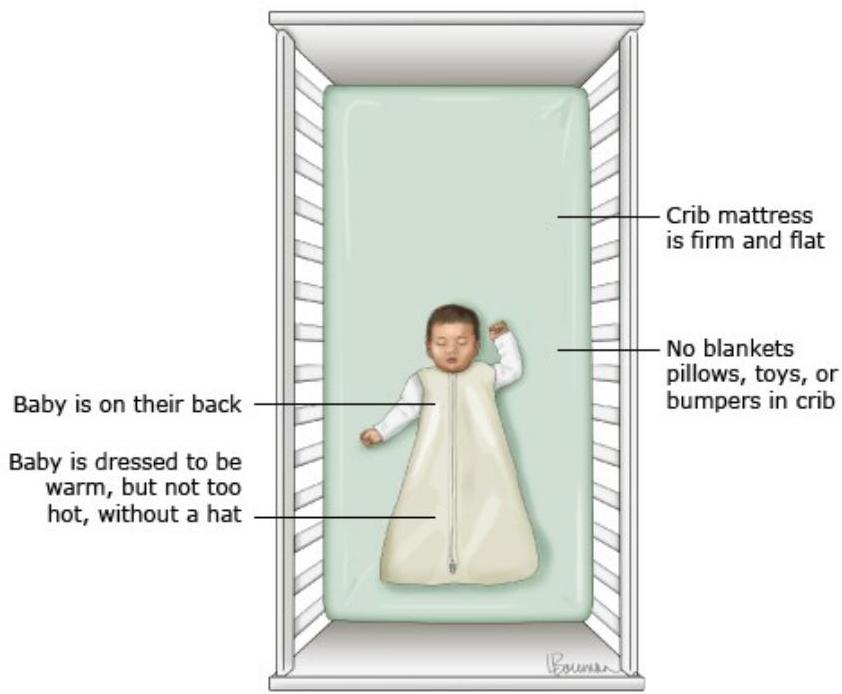
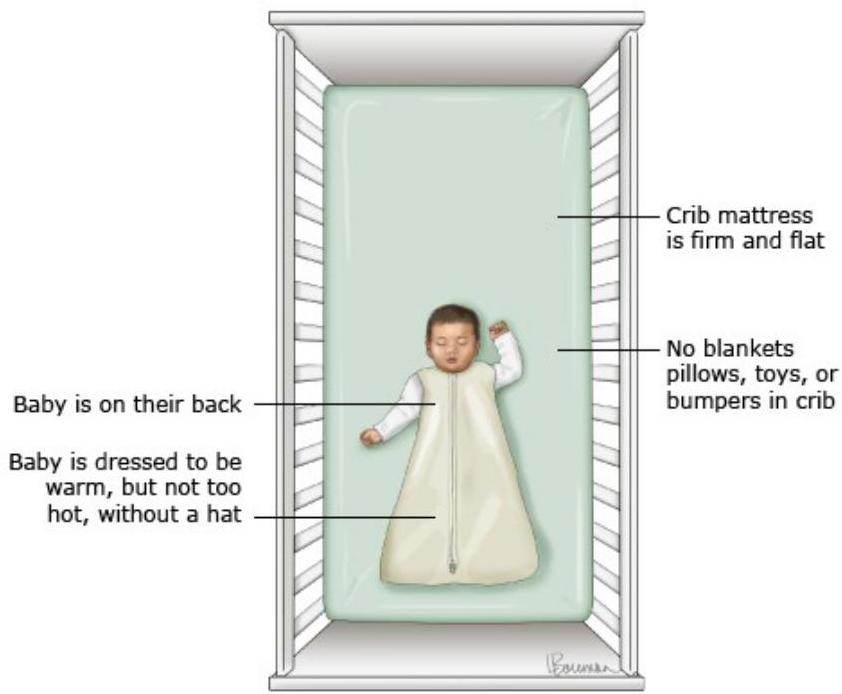
The provider may recommend caregivers:
- Place the infant on his back when sleeping or napping. His face should be free.
- Avoid soft bedding materials. Babies should be placed on a firm, tight-fitting crib mattress without loose bedding.
- Use a light sheet to cover the baby.
- Do not use pillows, comforters, or quilts.
- Avoid exposure to secondhand smoke.
All infants should be placed on their backs (supine) for every sleep. Infants should sleep on a firm sleep surface designed specifically for infants (crib, cradle, or bassinet), with no pillows, blankets, bumper pads, loose bedding, or sleep positioners[1].
Additional Home Care Recommendations
- Consider saline nose drops or using a nasal bulb if the nose is congested.
- Learn proper techniques to respond to any future events. This includes NOT shaking the infant.
- Avoid overfeeding, perform frequent burping during feedings, and hold the infant upright after feeding.
- Talk to your provider before thickening your child’s feedings or using medicines that reduce acid and reflux.
- Although not common, home monitoring devices may be recommended.
Prognosis
- Most often, these events are harmless and not a sign of more serious health problems or death.
- BRUE is unlikely to be a risk for sudden infant death syndrome (SIDS). Most victims of SIDS do not have any types of events beforehand.
- A child with risk factors for BRUE may have a higher risk for recurrence or the presence of a serious cause.

Sudden Infant Death Syndrome (SIDS)
Definition and Epidemiology
- SIDS is defined as the sudden death of an infant younger than one year of age, which remains unexplained after a thorough case investigation.
- SIDS is the leading cause of infant mortality between one month and one year of age in the United States.
Disorders That Can Mimic SIDS
General
| Condition | System |
|---|---|
| Sepsis (including meningococcemia) | General |
| Asphyxiation (accidental or deliberate) | General |
| Anaphylaxis | General |
| Metabolic decompensation | General |
| Hyperthermia | General |
| Poisoning (with toxic effects on kidney, liver, and/or brain) | General |
| Inborn errors of metabolism (may affect liver, muscle, and/or brain) | General |
Blood
| Condition | System |
|---|---|
| Sickle cell disease in crisis | Blood |
Cardiovascular System
| Condition | System |
|---|---|
| Subendocardial fibroelastosis | Heart |
| Congenital heart disease (especially aortic stenosis) | Heart |
| Myocarditis | Heart |
Respiratory System
| Condition | System |
|---|---|
| Pneumonia | Lungs |
| Bronchiolitis | Lungs |
| Tracheobronchitis (severe) | Lungs |
| Aspiration or airway obstruction | Lungs |
| Idiopathic pulmonary hypertension | Lungs |
Renal System
| Condition | System |
|---|---|
| Pyelonephritis | Kidney |
Gastrointestinal Tract
| Condition | System |
|---|---|
| Enterocolitis with Salmonella, Shigella, or pathogenic Escherichia coli | GI |
| Hepatitis | Liver |
| Pancreatitis | Pancreas |
| Boric acid poisoning | Pancreas |
| Cystic fibrosis | Pancreas |
Endocrine System
| Condition | System |
|---|---|
| Congenital adrenal hyperplasia | Adrenal |
Neurological System
| Condition | System |
|---|---|
| Encephalitis | Brain |
| Trauma (skull fracture, cerebral edema, subdural hemorrhage) | Brain |
| Child abuse (abusive head trauma, intentional suffocation) | Brain |
| Arteriovenous malformation with bleeding | Brain |
Risk Factors for SIDS
Consistently identified as independent risk factors:
Maternal Factors
- Young maternal age (under 20 years)
- Maternal smoking during pregnancy
- Late or no prenatal care
- Maternal alcohol use
Infant and Environmental Factors
- Preterm birth and/or low birth weight
- Prone sleeping position
- Sleeping on a soft surface and/or with bedding accessories such as loose blankets and pillows
- Bed-sharing (e.g., sleeping in parents’/caregivers’ bed)
- Overheating
- Sibling of an infant with SIDS / Twins
- Swaddling (older infants)
Note: Many risk factors are modifiable (usually sleeping position, sleep environment, or parental smoking).

Protective Factors
The following factors are associated with reduced risk of SIDS:
- Breastfeeding
- Room-sharing
- Pacifier use
- Fan use
- Immunizations
Note: No benefit from home monitors.
Reference
- Moon RY, Carlin RF, Hand I, Task Force on Sudden Infant Death Syndrome and the Committee on Fetus and Newborn. Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics 2022; 150:e2022057990.