Diagnostic Approach to Childhood Asthma
Diagnosing asthma in children requires a comprehensive approach incorporating multiple elements:
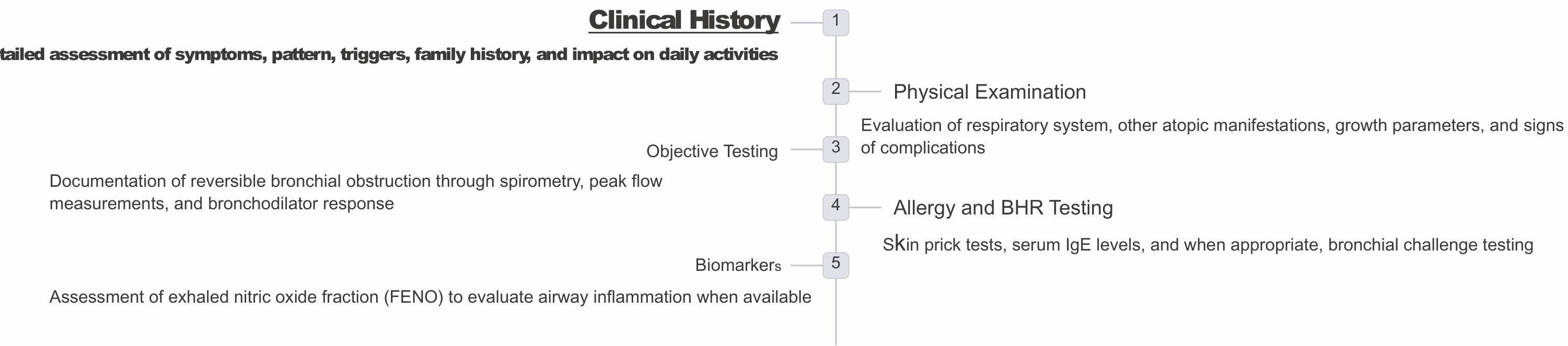
High Probability Features for Asthma Diagnosis
Key Clinical Features
- Multiple symptom types (dry cough, wheezing, shortness of breath, chest tightness)
- Symptoms worse at night and early morning
- Symptoms with non-viral triggers
- Interval symptoms between acute exacerbations
- Personal or family history of atopic disease
- Positive response to asthma therapy
Important Assessment Questions
- Frequency of symptoms?
- Specific triggers? Especially sports and activities
- How often is sleep disturbed?
- Severity of interval symptoms?
- School absences due to asthma?
- Impact on quality of life and daily functioning?
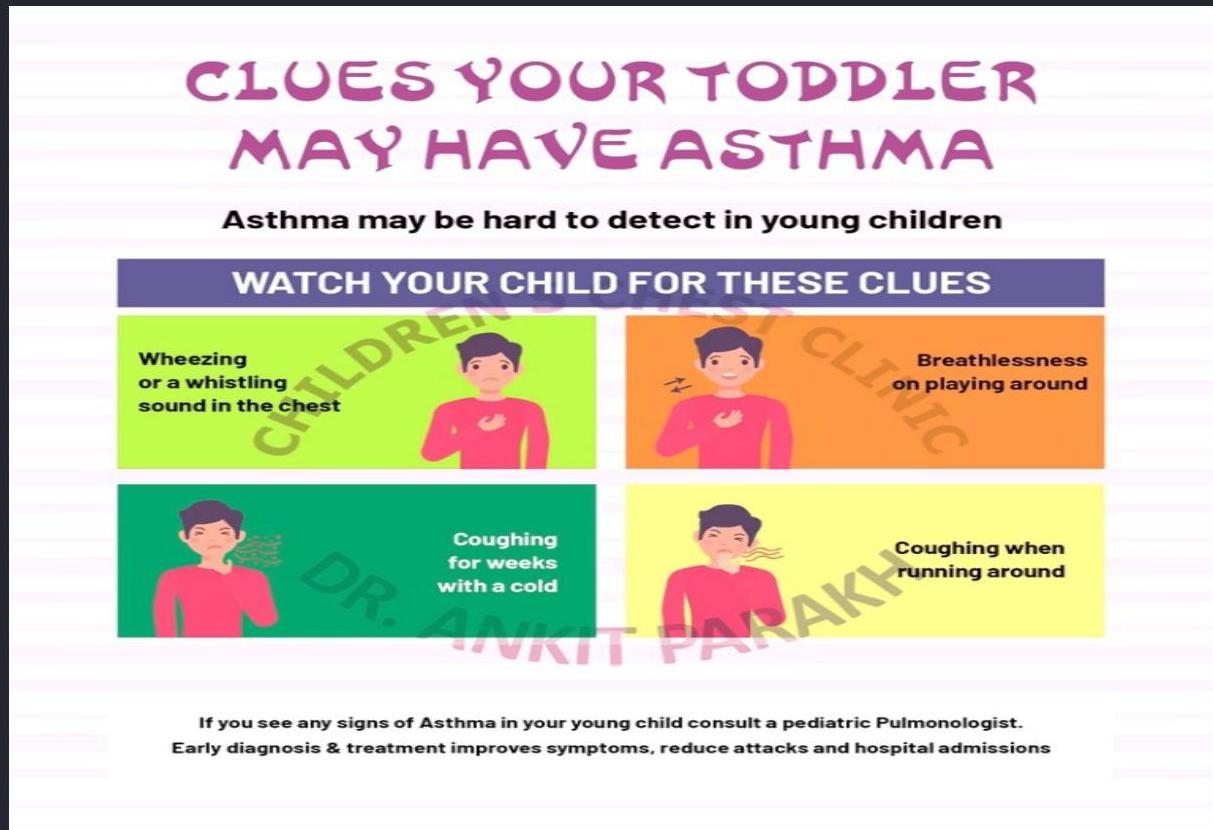
Diagnostic Features in Children ≤5 Years
Diagnosing asthma in young children presents unique challenges due to limited ability to perform objective testing and overlapping symptoms with other conditions.
Cough Patterns
- Recurrent or persistent non-productive cough
- Nocturnal cough or with exercise, laughing, crying
- Cough with exposure to tobacco smoke
- Prolonged cough in infancy without cold symptoms
- Cough persisting after viral infections
Breathing Abnormalities
- Recurrent wheezing during sleep or with triggers
- Difficult or heavy breathing with minimal exertion
- Shortness of breath with exercise, laughing, or crying
- Audible wheeze without stethoscope during exacerbations
Activity & History Clues
- Reduced activity level compared to peers
- Tires earlier during walks (wants to be carried)
- Other allergic disease (atopic dermatitis, allergic rhinitis)
- Asthma in first-degree relatives
Therapeutic Trial
- Clinical improvement during 2-3 months of controller treatment
- Symptom worsening when treatment is stopped
- Reduced need for rescue medications
Features Suggesting Asthma in Children ≤5 Years
| Feature | Characteristics suggesting asthma |
|---|---|
| Cough | Recurrent or persistent non-productive cough that may be worse at night or accompanied by some wheezing and breathing difficulties. Cough occurring with exercise, laughing, crying or exposure to tobacco smoke in the absence of an apparent respiratory infection. Prolonged cough in infancy, and cough without cold symptoms, are associated with later parent-reported physician-diagnosed asthma, independent of infant wheeze. |
| Wheezing | Recurrent wheezing, including during sleep or with triggers such as activity, laughing, crying or exposure to tobacco smoke or air pollution. |
| Difficult or heavy breathing or shortness of breath | Occurring with exercise, laughing, or crying. |
| Reduced activity | Not running, playing or laughing at the same intensity as other children; tires earlier during walks (wants to be carried). |
| Past or family history | Other allergic disease (atopic dermatitis or allergic rhinitis). Asthma in first-degree relatives. |
| Therapeutic trial with low dose ICS and as-needed SABA | Clinical improvement during 2–3 months of controller treatment and worsening when treatment is stopped. |
Wheezing Patterns in Early Childhood
Diagnosing asthma in preschool children is often difficult. Approximately half of all children wheeze at some time during the first 3 years of life. Here are three common patterns of wheezing:
1. Viral Episodic Wheezing
Wheezing occurs exclusively in response to viral infections.
2. Multiple Trigger Wheeze
Wheezing is triggered by various factors and has a higher likelihood of developing into chronic asthma over time.
3. Asthmatic Wheezing
Persistent wheezing often indicative of underlying asthma, requiring ongoing management.
Modified Asthma Predictive Index (mAPI)
For children under 3 years of age with ALL of the following:
- 4 wheezing exacerbations in past year, with 1 physician-confirmed episode
- Plus one major criteria OR 2 minor criteria
Major Criteria (1 of the following):
- Parental history (mother with childhood asthma, father with exercise-induced asthma)
- Physician-diagnosed atopic dermatitis (eczema)
- Allergic sensitization to aeroallergen (dust mite, cat, dog, mold, grass, trees, weeds)
Minor Criteria (2 of the following):
- Allergic sensitization to food milk, egg, or peanut (positive skin or blood test)
- Wheezing unrelated to colds
- Blood eosinophilia ≥4% of white blood cell count (WBC)
Positive index: 76% risk of asthma during school years
Negative index: 95% chance of not having asthma during school years
AllergyGoAway.com, JACI 2010: 126(2):212-6, updated: 2015
Differential Diagnosis of Childhood Wheezing
Not all that wheezes is asthma. Consider these important differential diagnoses in pediatric patients:
Anatomic Abnormalities
- Tracheomalacia/bronchomalacia
- Vascular rings/slings
- Laryngotracheal stenosis
- Foreign body aspiration
Infectious/Inflammatory
- Bronchiolitis
- Cystic fibrosis
- Primary ciliary dyskinesia
- Bronchopulmonary dysplasia
Other Conditions
- Vocal cord dysfunction
- Gastroesophageal reflux
- Congenital heart disease
- Immunodeficiencies
Red Flags for Alternative Diagnoses
| Red flag | Possible diagnosis |
|---|---|
| Sudden onset of symptoms | Foreign body aspiration |
| Coughing and choking when eating or drinking | Oropharyngeal dysphagia with aspiration |
| Poor growth and low BMI | Cystic fibrosis, immunodeficiency |
| Family history of males infertility | Cystic fibrosis, immotile cilia syndrome |
| Chronic rhinorrhea, recurrent sinusitis | Cystic fibrosis, immotile cilia syndrome |
| Acute onset without history of asthma in teenagers | Vocal cord dysfunction |
| Chronic wet productive cough | Bronchiectasis |
| Recurrent pneumonia | Immunodeficiency |
Diagnostic Tests for Childhood Asthma
1- Clinical Assessment
In younger children (<5 years), asthma is usually diagnosed based on history and examination alone due to limitations in objective testing capabilities.
2- Allergy Testing
Skin-prick testing for common allergens may help identify specific triggers and confirm atopic status. Serum IgE levels can provide additional supportive evidence.
3- Imaging Studies
Chest X-ray is typically normal in asthma but may reveal hyperinflation and increased bronchial markings during exacerbations. Primarily used to rule out alternative diagnoses.
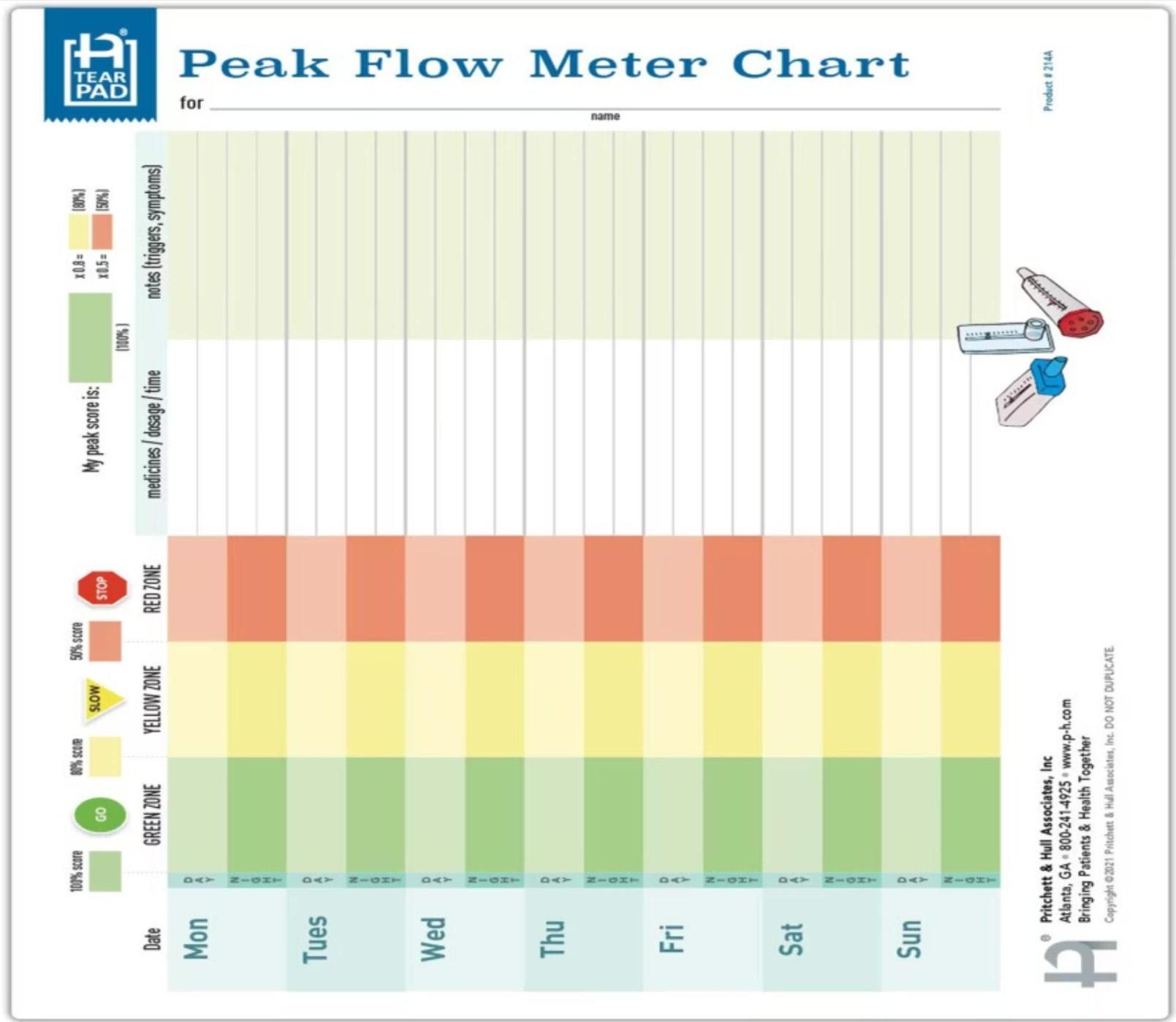
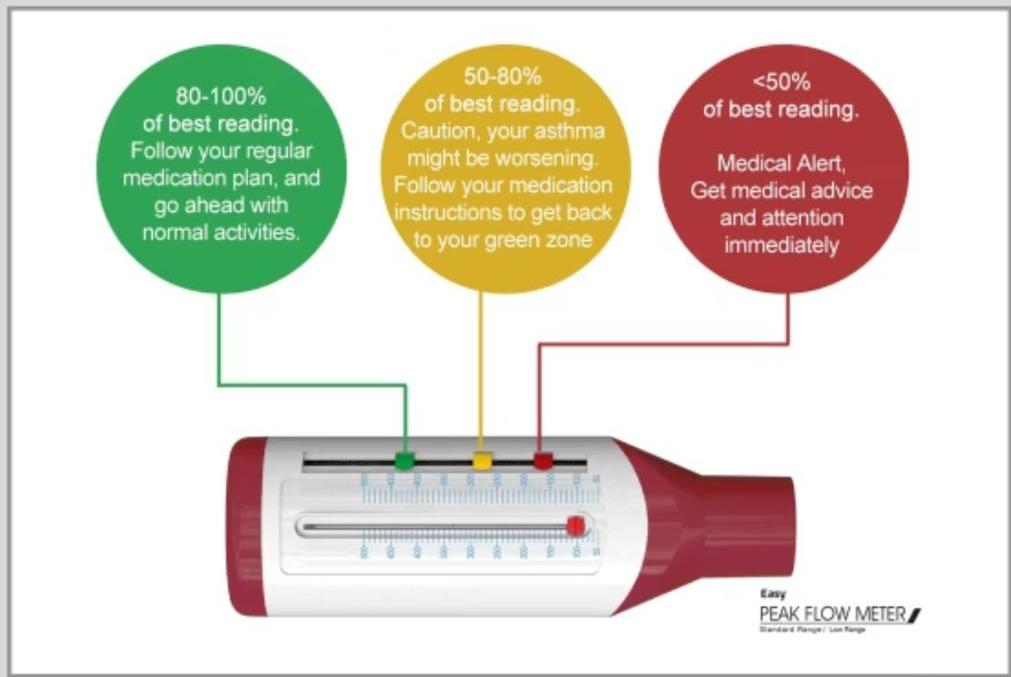
4- Peak Flow Monitoring
Peak expiratory flow rate (PEFR) is portable and helpful for serial measurements. Useful for children >5 years to monitor control and detect early exacerbations.
5- Pulmonary Function Testing
Spirometry can be performed in most children ≥5 years. Reduced FEV1, FEV1/FVC ratio, and FEF 25-75% are characteristic. Bronchodilator reversibility (≥12% improvement in FEV1) confirms diagnosis.
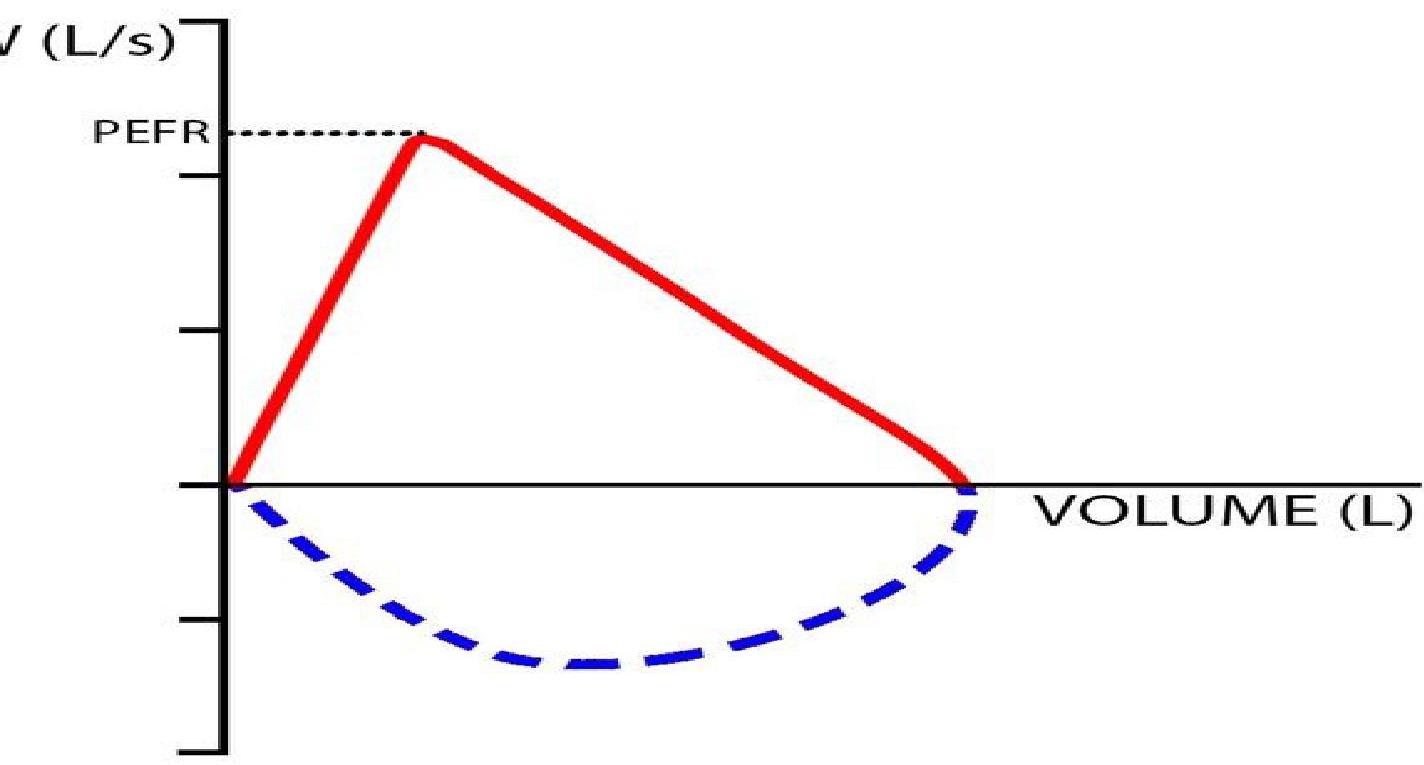
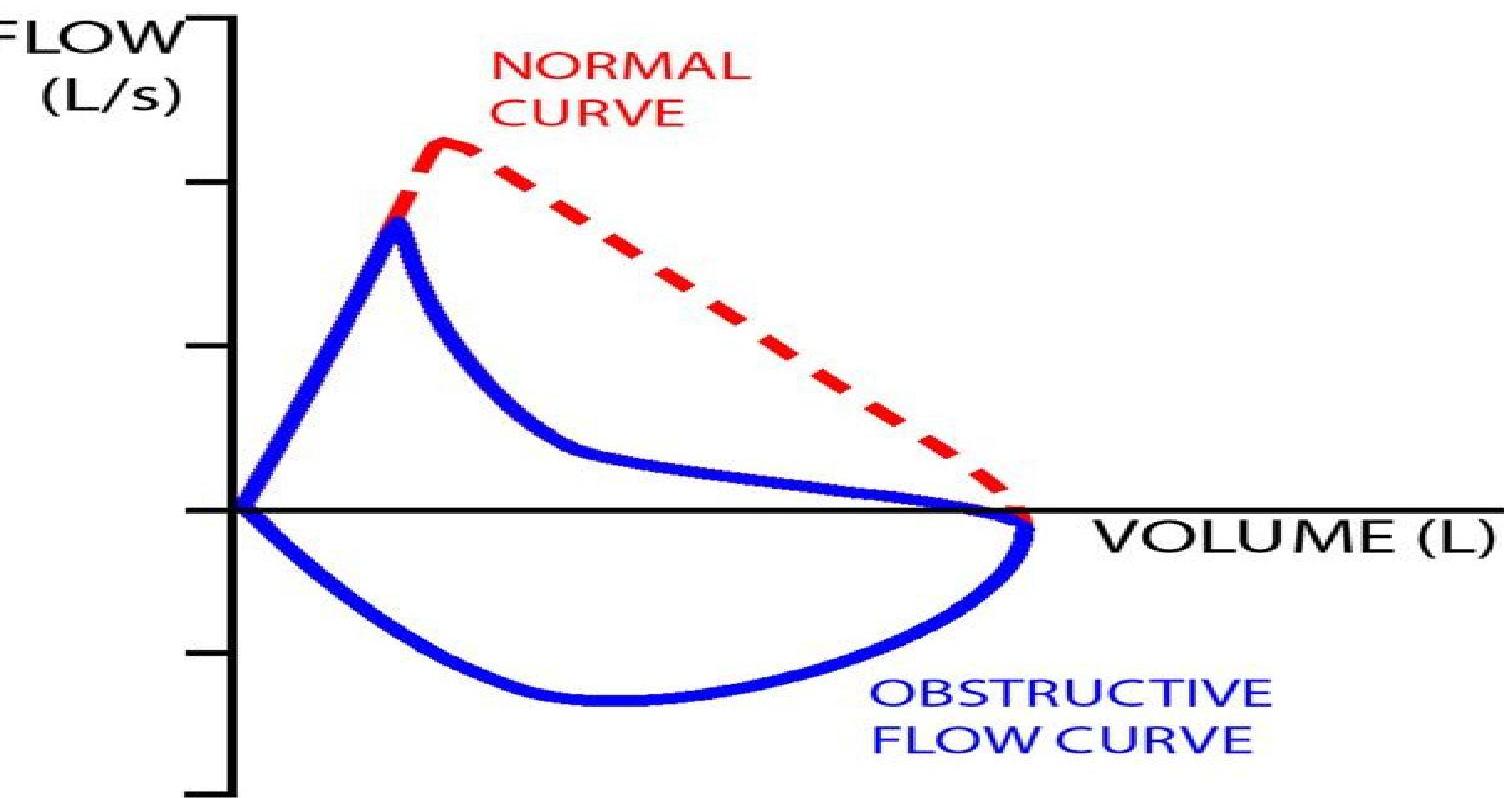
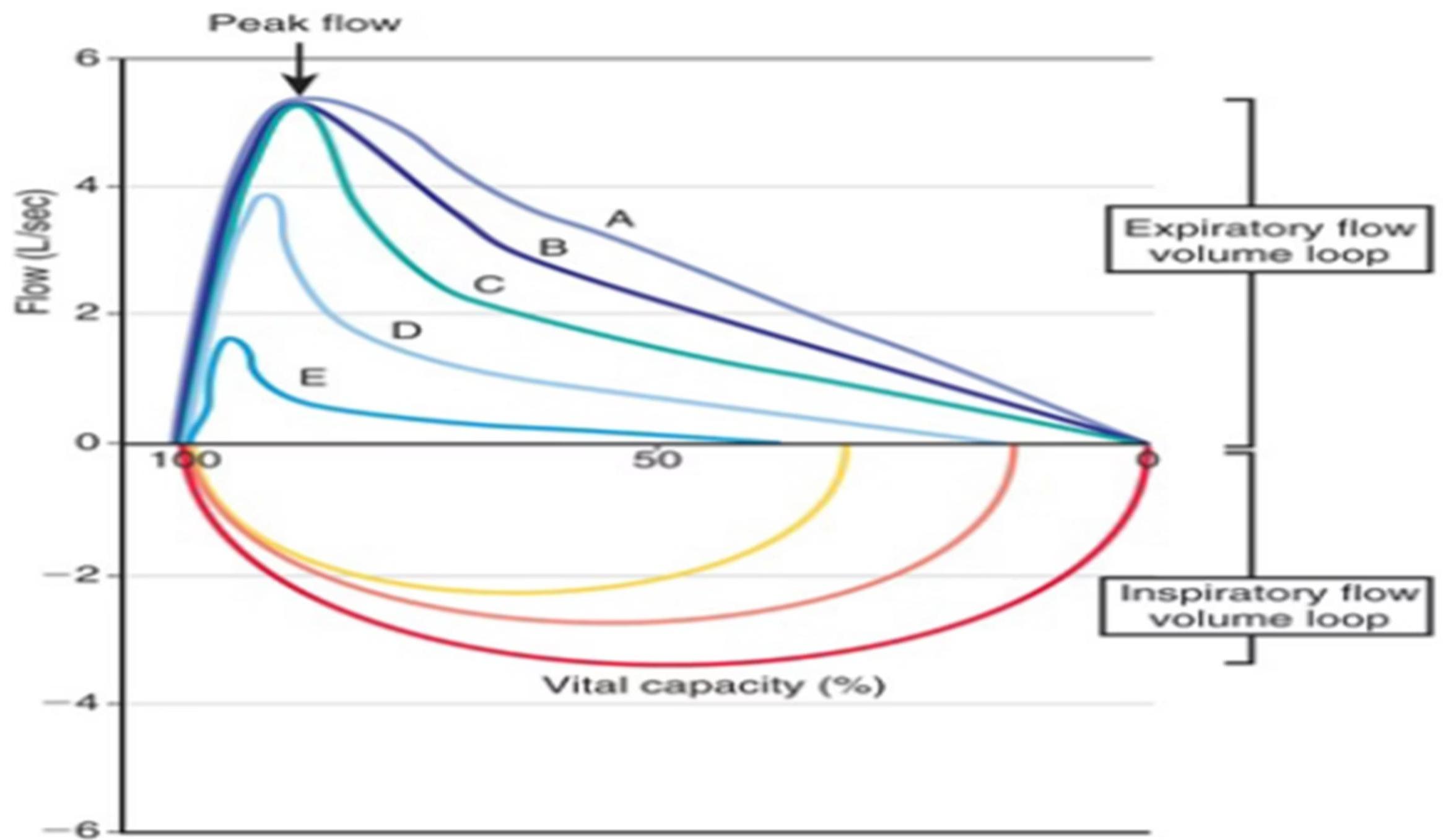 Spirometric flow-volume loops. Loop A is an expiratory flow-volume loop of a non-asthmatic person without airflow limitation. B through E are expiratory flow-volume loops in asthmatic patients with increasing degrees of airflow limitation (B is mild; E is severe). Note the “scooped” or concave appearance of the asthmatic expiratory flow-volume loops; with increasing obstruction, there is greater “scooping.”
Spirometric flow-volume loops. Loop A is an expiratory flow-volume loop of a non-asthmatic person without airflow limitation. B through E are expiratory flow-volume loops in asthmatic patients with increasing degrees of airflow limitation (B is mild; E is severe). Note the “scooped” or concave appearance of the asthmatic expiratory flow-volume loops; with increasing obstruction, there is greater “scooping.”
Spirometric volume-time curves Subject 1 is a non-asthmatic person; subject 2 is an asthmatic patient.
- Note how the FEV1 and FVC lung volumes are obtained. The FEV1 is the volume of air exhaled in the 1st sec of a forced expiratory effort.
- The FVC is the total volume of air exhaled during a forced expiratory effort, or forced vital capacity.
- Note that subject 2’s FEV1 and FEV1 :FVC ratio are smaller than subject 1’s, demonstrating airflow limitation. Also, subject 2’s FVC is very close to what is expected.
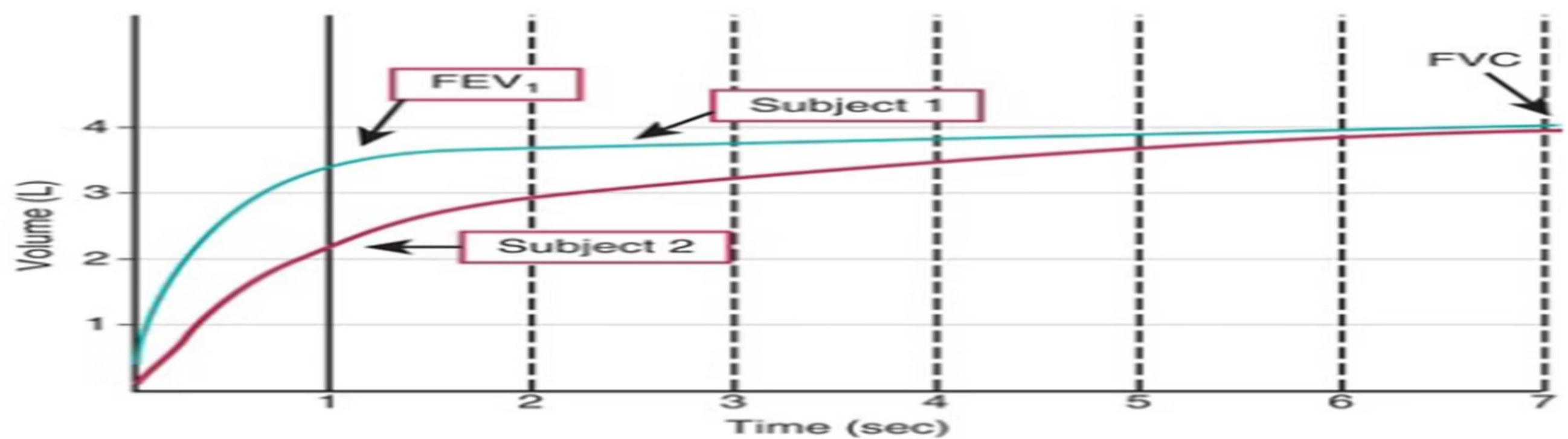
Subject 1: A non-asthmatic child
- (100% of predicted)
- FVC = 3.8 (100% of predicted)
Subject 2: An asthmatic child
- (62% of predicted)
- FVC = 3.7 (97% of predicted)

Lung Function Testing in Asthma: Objective Assessment
1. Spirometry
Airflow Limitation Parameters:
- Low FEV1 (relative to percentage of predicted norms)
- FEV1/FVC ratio < 0.80 indicates obstruction
- Reduced expiratory flow rates (FEF 25-75%)
2. Bronchodilator Reversibility
Diagnostic Criteria:
- Improvement in FEV1 of 12% or more from baseline
- Performed 15 minutes after administration of SABA
3. Fractional Exhaled Nitric Oxide (FeNO)
Inflammatory Marker:
- FeNO level of 35ppb or more suggests eosinophilic inflammation
- Useful for predicting steroid responsiveness
- May help differentiate asthma phenotypes
4. Peak Flow Variability
Measuring Variability:
- Day-to-day and/or AM-to-PM variation ≥20% indicates poor control
- Useful for home monitoring of asthma control
- Best used as a trend over time rather than absolute values
Classifying Asthma Severity: A Systematic Approach
Accurate classification forms the foundation of effective asthma management. Severity assessment guides initial treatment decisions and helps establish an appropriate baseline for monitoring.
1. Intermittent Asthma
- Symptoms < twice weekly
- Brief flare-ups (intensity may vary)
- Nighttime symptoms < twice monthly
- Asymptomatic between flare-ups
- FEV₁ ≥ 80% predicted
- Peak flow variability < 20%
2. Mild Persistent Asthma
- Symptoms 3-6 times weekly
- Flare-ups may affect activity
- Nighttime symptoms 3-4 times monthly
- FEV₁ ≥ 80% predicted
- Peak flow variability 20-30%
Classification should be reassessed at regular intervals as severity can change over time with treatment or disease progression.
3. Moderate Persistent Asthma
- Daily symptoms of cough, wheezing, chest tightness, or breathing difficulty
- Activity level affected by flare-ups
- Nighttime symptoms ≥ 5 times monthly
- FEV₁ > 60% but < 80% of predicted values
- Peak flow variability > 30%
4. Severe Persistent Asthma
- Continual symptoms throughout the day
- Frequent nighttime symptoms
- FEV₁ ≤ 60% of predicted values
- Peak flow variability > 30%
- Significant limitation of daily activities

Comprehensive Asthma Classification Framework
| Classification | Symptom Severity | Lung Function | Exacerbations Requiring Systemic Corticosteroids |
|---|---|---|---|
| Intermittent | • Symptoms ≤ 2/week • Nighttime symptoms ≤ 2/month • No interference with activities • SABA use ≤ 2 days/week • Normal between exacerbations | • FEV₁ > 80% predicted • Normal FEV₁/FVC ratio | ≤ 1/year |
| Mild Persistent | • Symptoms > 2/week (not daily) • Nighttime symptoms 3-4/month • SABA use > 2 days/week • Minor activity limitations | • FEV₁ ≥ 80% predicted • Normal FEV₁/FVC ratio | ≥ 2/year |
| Moderate Persistent | • Daily symptoms • Nighttime symptoms > 1/week • Some activity limitations • Daily SABA use | • FEV₁ 60-80% predicted • FEV₁/FVC decreased by < 5% | ≥ 2/year |
| Severe Persistent | • Continuous daily symptoms • Nightly symptoms • Extreme activity limitations • SABA use several times daily | • FEV₁ < 60% predicted • FEV₁/FVC decreased by ≥ 5% | ≥ 2/year |
SABA = Short-Acting Beta Agonist; FEV₁ = Forced Expiratory Volume in 1 second; FVC = Forced Vital Capacity