Acute Asthma Exacerbation: Recognition and Initial Management
Assessment of the Child with Acute Asthma
Determine the severity of the attack:
- Mild
- Moderate
- Severe
- Life-threatening
Key Indicators:
- Too breathless to talk or eat?
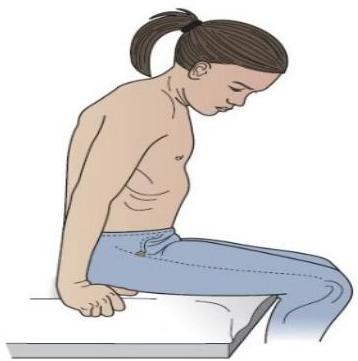
- Increased work of breathing: Tachypnoea (severe if >30 breaths/min)
- Chest recession:
- Moderate - some intercostal recession
- Severe - use of accessory neck muscles
- Life-threatening - poor respiratory effort
- Auscultation:
- Wheeze
- Silent chest - poor air entry in life-threatening
- Pulse: Severe – >120 beats/min
- Level of consciousness: altered in life-threatening
- Exhaustion
- Tongue: Cyanosis in life-threatening
- Peak flow (% predicted):
- Moderate >53%
- Severe <50%
- Life-threatening <53%
- O₂ saturation:
- Moderate >52%
- Severe or life-threatening <52%
- Is there a trigger for the attack?: URTI or other vital illness, Pneumonia, Allergen (e.g. animal dander), Exercise, Cold air
Definition & Characteristics
- Episodes of progressive worsening of asthma symptoms and lung function
- May be initial presentation or occur in known asthma patients
- Usually triggered by viral infections, allergens, irritants, or medication non-adherence
- Can develop gradually (days) or rapidly (minutes to hours)
Status Asthmaticus
A severe asthma exacerbation that progresses rapidly and does not respond to standard acute therapy. Requires aggressive management and often hospitalization to prevent respiratory failure.
Initial Assessment
Rapidly evaluate severity through vital signs, work of breathing, mental status, and ability to speak in complete sentences.
Management Basics
- Oxygen & Bronchodilators: Administer oxygen to maintain and SABA via nebulizer or MDI with spacer.
- Early Corticosteroids: Give systemic corticosteroids within first hour for all but mildest exacerbations.
Diagnostic Evaluation During Acute Exacerbations
Blood Gases
Indicated for severe exacerbations or inadequate response to initial therapy:
- Normal or elevated PaCO₂ (>40 mmHg) indicates severe airflow obstruction and fatigue
- Hypoxemia is common but may improve with supplemental oxygen
- Respiratory alkalosis is typical in early stages
- Normalized pH with elevated PaCO₂ suggests impending respiratory failure
Electrolytes
Assess for abnormalities that may complicate therapy:
- Hypokalemia (from β-agonists or prior diuretic use)
- Hyperglycemia (from stress response or corticosteroid administration)
- Elevated BUN/creatinine (from dehydration)
Chest Imaging
Not routinely indicated but consider when:
- Initial presentation in adults
- Suspicion of pneumothorax or pneumonia
- Life-threatening exacerbation
- Failure to respond to therapy
- Significant chest pain or asymmetric findings

Assessment of Acute Asthma Exacerbation Severity
| Feature | Mild-moderate | Severe | Life threatening |
|---|---|---|---|
| General | oxygen saturation 92% and above in air PEFR > 50% predicted of best | cannot complete sentences in one breath or too breathless to talk or eat/feed oxygen saturation < 92% in air PEFR < 50% predicted or best | cyanosis silent chest poor respiratory effort fatigue or exhaustion agitation or reduced level of consciousness raised carbon dioxide |
| Under 6 years | heart rate < 140/min respiratory rate < 40/min | heart rate > 140/min respiratory rate > 40/min | |
| 6 years and over | heart rate < 125/min respiratory rate < 30/min | heart rate > 125/min respiratory rate > 30/min |
Severity assessment guides treatment intensity, location of care, and frequency of monitoring. Patients may not present with all features of a single severity category, and clinical judgment remains essential.
Acute Exacerbation: Treatment Approach
Bronchodilator Therapy
- SABA (albuterol/salbutamol): 4-8 puffs via MDI with spacer q20min for 1 hour OR 2.5-5mg via nebulizer q20min for 1 hour
- Ipratropium bromide: Added for severe exacerbations or poor initial response to SABA
- Frequency: Initially continuous or q30-60min, then q1-4h based on response
Corticosteroids
- Oral route preferred: Prednisone/prednisolone
- IV route: For patients unable to take oral medications or with absorption concerns
- Early administration: Within first hour for moderate to severe exacerbations
Adjunctive Therapies
- Oxygen: Titrate to maintain SpO₂ 93-95% (94-98% for children)
- IV Magnesium sulfate: Single dose of 2g over 20min for severe exacerbations with incomplete response to initial therapy
- IV Aminophylline: Generally not recommended in standard care; consider only under specialist supervision for life-threatening cases unresponsive to maximal therapy
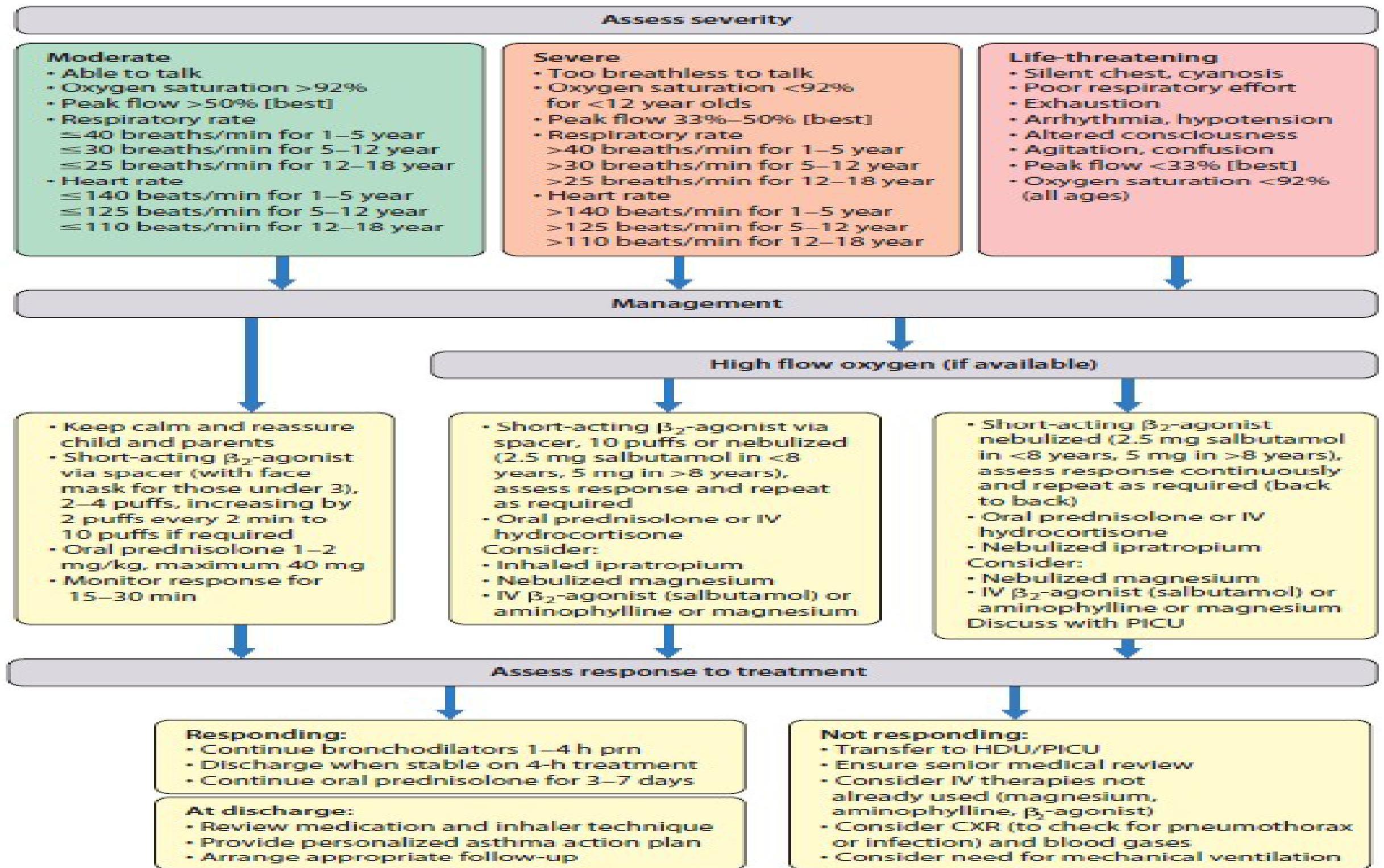 Figure 17.14 Management of acute asthma. (Adapted and modified from: The Scottish Intercollegiate Guideline Network/British Thoracic Society, July 2019.)
Figure 17.14 Management of acute asthma. (Adapted and modified from: The Scottish Intercollegiate Guideline Network/British Thoracic Society, July 2019.)
Acute Exacerbation Management Algorithm
- Initial Assessment
- Evaluate symptom severity, vital signs, work of breathing, mental status, and response to initial treatment.
- Initial Treatment
- SABA, oxygen if hypoxemic, and systemic corticosteroids for all but mildest cases. Add ipratropium for severe cases.
- Reassessment (15-30 min)
- Evaluate response to treatment. Determine if escalation of care is needed based on clinical improvement and objective measures.
- Disposition Decision
- Discharge with follow-up plan if good response. Intensify therapy and continue monitoring if partial response. Consider ICU for poor/deteriorating response.
Monitor patients closely for signs of deterioration, including increasing work of breathing, decreasing mental status, worsening PEF/FEV₁, or development of silent chest (severe bronchospasm with minimal air movement).