Epidemiology of Childhood Asthma
Global and Regional Prevalence
Asthma is one of the most common chronic diseases in children worldwide, with significant geographic variation:
- The prevalence in Saudi children ranges from 8% to 25%, representing a significant burden on healthcare systems.
- Global prevalence continues to rise, especially in developing countries adopting Western lifestyles.
Demographic Patterns
Sex Distribution
Differs depending on age of onset:
- Males > Females before puberty
- Females > Males after puberty
Age of Onset
Typically begins in childhood:
- ~80% of cases begin before age 6
- Peak incidence at 3-6 years of age
Etiology: A Multifactorial Disease
Childhood asthma results from a complex interplay between:
- Inherent biological and genetic vulnerabilities
- Environmental exposures and triggers
Primary Risk Factors
- Family history of asthma (particularly maternal)
- Personal history of allergic conditions
- Atopic dermatitis in early life
- Prenatal factors (maternal smoking, diet)
Common Triggers
- Environmental allergens: pollen, dust mites, pet dander
- Viral respiratory infections: especially RSV, rhinovirus
- Physical factors: exercise, cold air, laughter
- Irritants: tobacco smoke, air pollution, strong odors
- Medications: NSAIDs, beta-blockers
- Comorbidities: GERD, chronic sinusitis, obesity
- Psychological stress
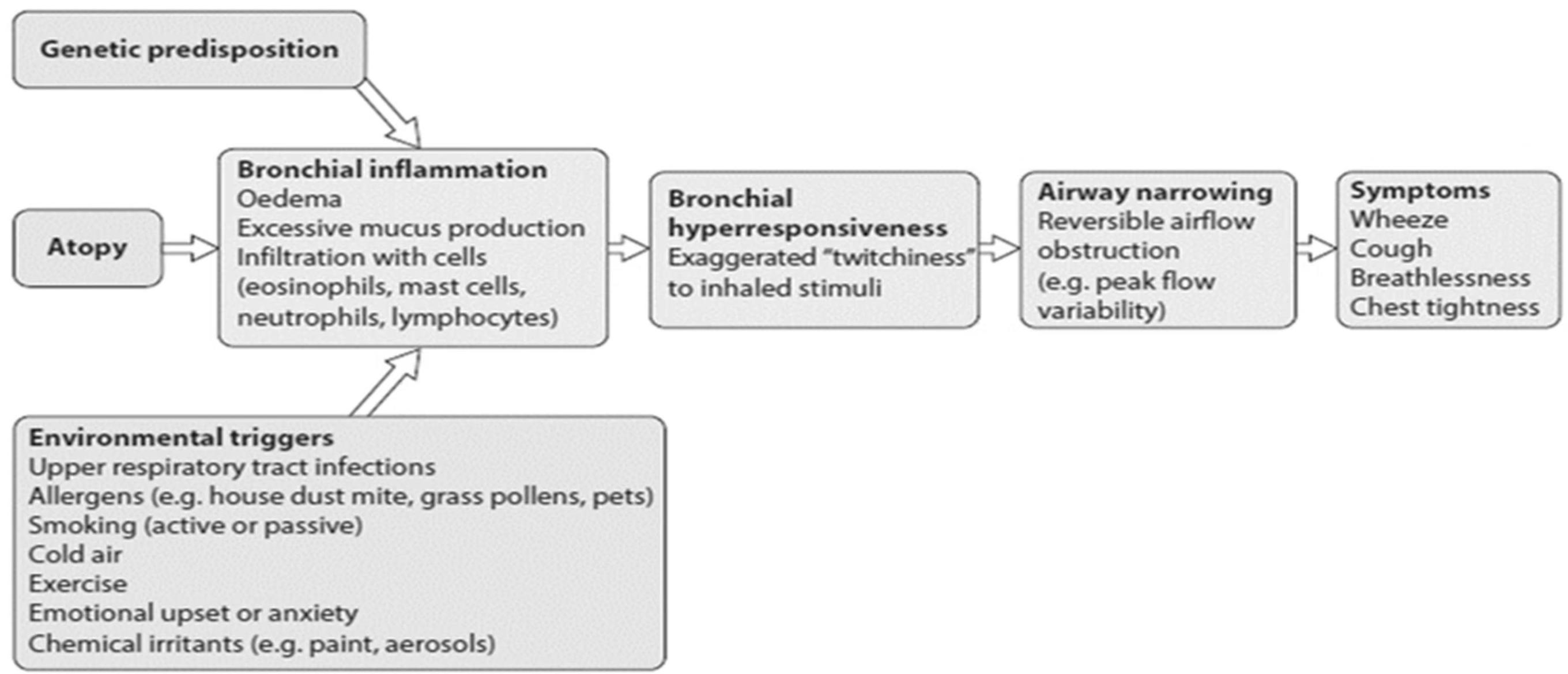
 Diagram showing relationship between genetic predisposition and environmental factors in asthma development
Diagram showing relationship between genetic predisposition and environmental factors in asthma development
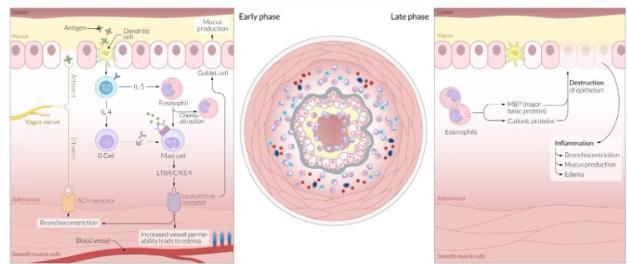
Pathophysiology: Inflammatory Cascade
Key Mechanisms in Asthma Pathophysiology
- Allergen Exposure
- Initial sensitization to allergens activates dendritic cells and T-helper lymphocytes
- Inflammatory Response
- Release of cytokines (IL-4, IL-5, IL-13) and recruitment of inflammatory cells (eosinophils, mast cells)
- Airway Effects
- Bronchoconstriction, mucus hypersecretion, airway edema, and eventual airway remodeling
This chronic inflammatory process leads to airway hyperresponsiveness and variable airflow limitation that produces the characteristic symptoms of asthma.
Asthma is an inflammatory disease driven by T-helper type 2 cells (Th2-cell) that manifests in individuals with a genetic predisposition.
Inflammatory cells (mast cells, eosinophils, T lymphocytes, neutrophils), chemical mediators (histamine, leukotrienes, platelet-activating factor, bradykinin), and chemotactic factors (cytokines(IL-3, IL-4, IL-5, IL-13), eotaxin) mediate the underlying inflammation found in asthmatic airways.
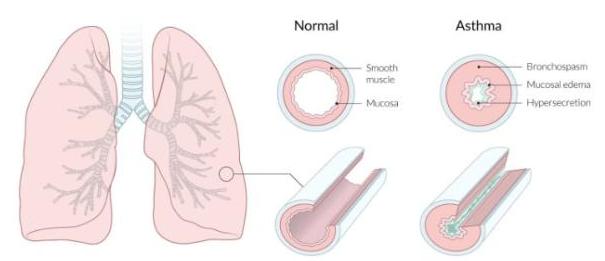
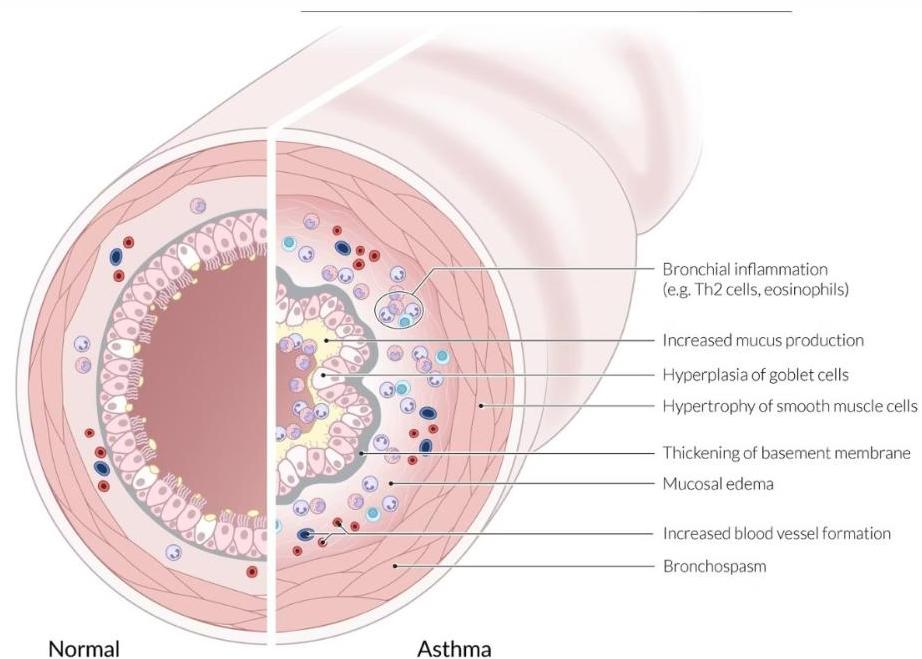
Airway Changes in Asthma
Structural and Functional Changes
Asthma involves multiple physiological alterations in the airways:
- Bronchial smooth muscle hypertrophy and hyperreactivity
- Mucus gland hyperplasia leading to increased secretions
- Epithelial damage and basement membrane thickening
- Inflammatory cell infiltration (eosinophils, T-cells)
- Vascular permeability causing mucosal edema
These changes result in the characteristic airflow limitation that manifests as wheezing, cough, and dyspnea during exacerbations.
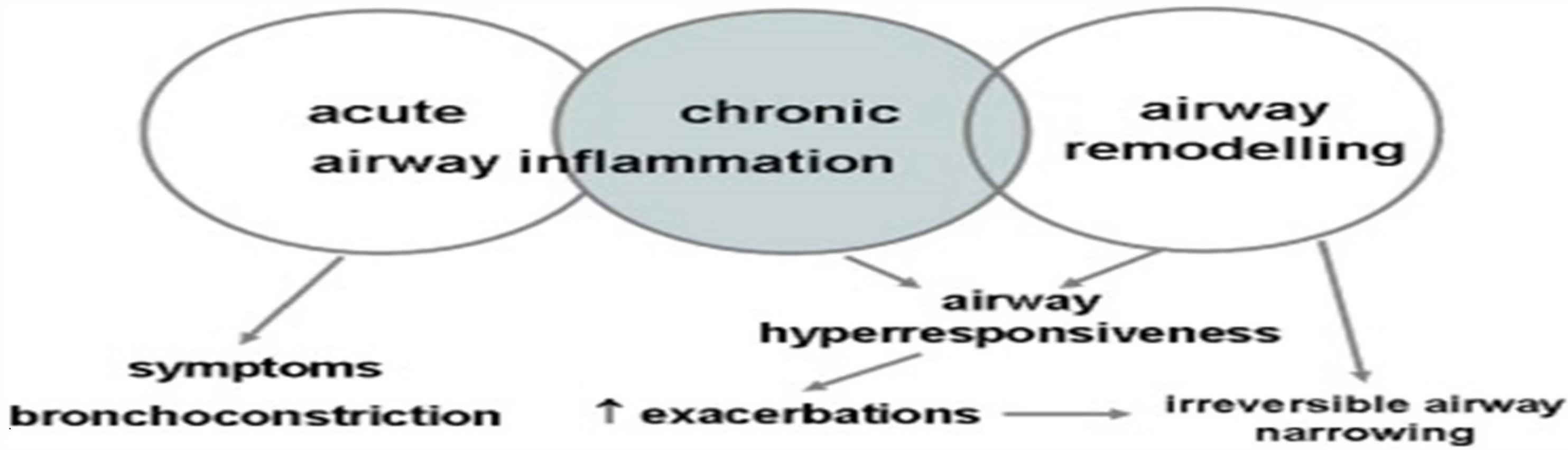
Pathophysiologic Consequences in Pediatric Asthma
Acute Effects
- Bronchoconstriction from smooth muscle contraction
- Increased mucus production obstructing airways
- Mucosal edema reducing airway diameter
- Air trapping due to expiratory airflow limitation
Chronic Effects
- Airway remodeling with subepithelial fibrosis
- Permanent changes in airway architecture
- Decreased lung function over time
- Reduced response to bronchodilators
These changes are often more reversible in children than adults, highlighting the importance of early intervention and consistent management.
Clinical Presentation of Childhood Asthma
Typical Features
These symptoms typically occur either sporadically or in response to specific triggers:
- Persistent, dry cough that worsens at night, with exercise, or exposure to triggers
- End-expiratory wheezing - generalized polyphonic expiratory wheeze with prolonged expiration
- Dyspnea - shortness of breath, especially during exacerbations
- Chest tightness - described by older children as “chest hurting”
- Prolonged expiratory phase on auscultation
- Hyperresonance to lung percussion during acute episodes
- Harrison’s sulci (indentations of the chest wall) may result from early-onset disease
☐ Intermittent dry coughing and expiratory wheezing are the most common chronic symptoms of pediatric asthma.
Atypical Presentations
- Exercise-induced asthma
- Cough-variant asthma
- Seasonal or episodic asthma
Common Comorbidities
- Allergic rhinitis
- Atopic dermatitis
- Food allergies
- Gastroesophageal reflux

Patient with Respiratory Symptoms: Age-Based Approach
Children aged ≤5 years:
- Cough
- Wheeze
- Difficulty breathing/shortness of breath
- Reduced activity
- Past/family history
- Symptoms worsen with viral infection or at night/upon waking
Children aged 6–11 years:
- Cough
- Wheeze
- Symptoms occur variably over time and intensity also varies
- Shortness of breath/chest tightness
- Symptoms triggered by exercise
- Symptoms worsen with viral infection or at night/upon waking
Assessment Steps:
- Test for atopy
- Chest X-ray could rule out structural abnormalities
- Risk profiles
- Spirometry to assess lung function
- Bronchial provocation testing
- FeNO measurement
Decision:
- Results consistent with asthma? → Treat for asthma
- History or test results not consistent with asthma? → Consider alternative diagnosis