Management Strategies
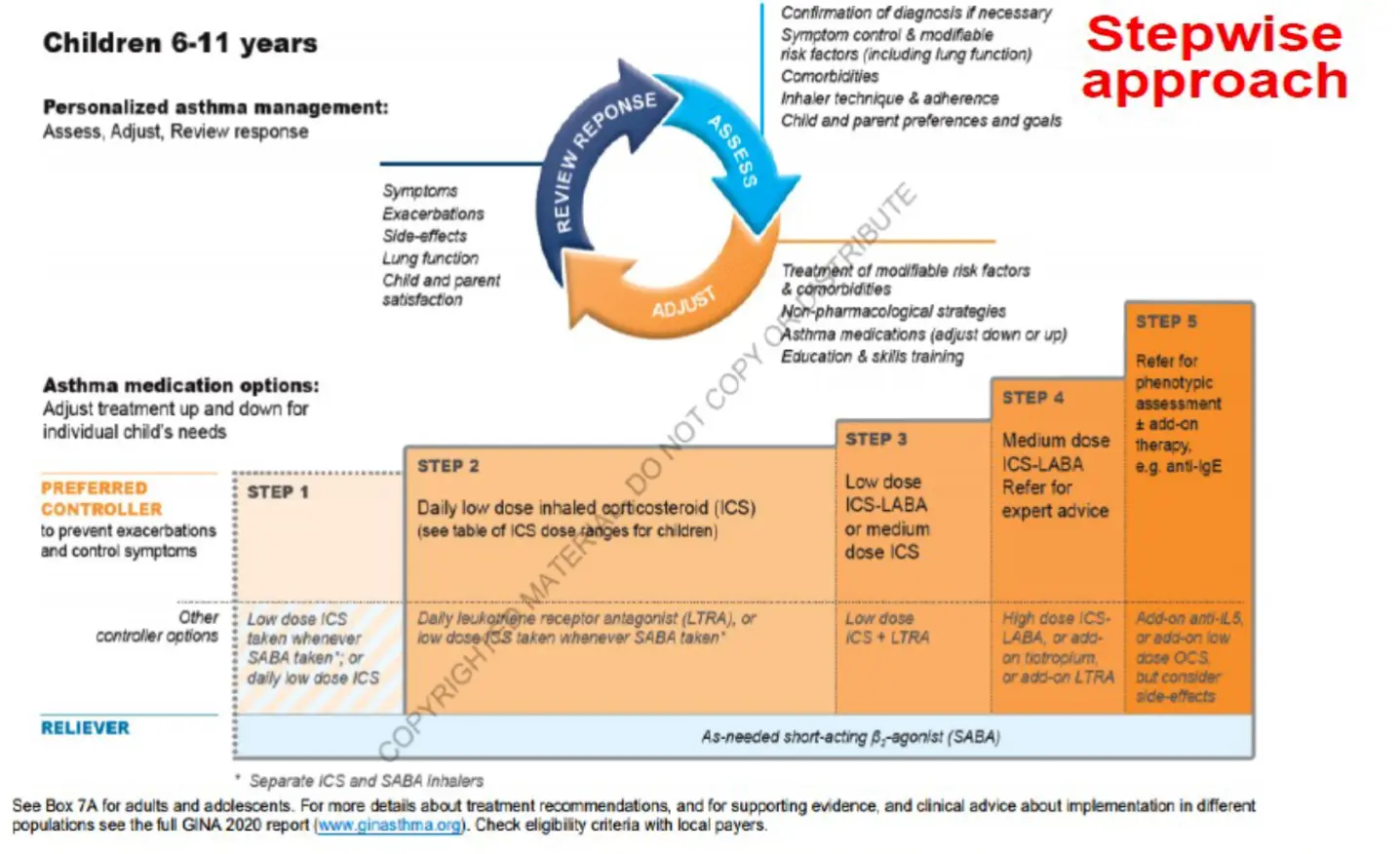
The Asthma Management Cycle for Personalized Asthma Care

1. Assessment
- Confirmation of diagnosis if necessary
- Symptom control & modifiable risk factors (see Box 2-2)
- Comorbidities
- Inhaler technique & adherence
- Patient (and parent/caregiver) preferences and goals
2. Adjustment
- Treatment of modifiable risk factors and comorbidities
- Non-pharmacological strategies
- Asthma medications (adjust down/up/between tracks)
- Education & skills training
3. Review Response
- Symptoms
- Exacerbations
- Side-effects
- Lung function
- Comorbidities
- Patient (and parent/caregiver) satisfaction
Foundational Components of Optimal Asthma Treatment
Key Treatment Components
- Environmental Control: Identify and minimize exposure to triggers
- Patient Education: Self-management skills, medication adherence, action plans
- Allergen Avoidance: Implement specific measures for identified allergens
- Influenza Immunization: Annual vaccination recommended
- Pharmacologic Therapy: Long-term control and quick-relief medications
Optimal management requires a comprehensive approach that addresses both symptom control and underlying inflammation while empowering patients through education.
Asthma Medication Classifications

Long-Term Control Medications
- Inhaled Corticosteroids (ICS)
- Leukotriene Modifiers
- Long-Acting β2 Agonists (LABA)
- Theophylline
- Biologics
Quick-Relief Medications
- Short-Acting β2 Agonists (SABA)
- Oral Corticosteroids (for acute exacerbations)
- Anticholinergics (ipratropium)
Effective asthma management typically requires both controller medications to reduce airway inflammation and rescue medications for symptom relief. The specific combination depends on severity classification and individual response.
Primary Asthma Medication Classes: Mechanisms and Applications
Short-Acting Beta-2 Agonists (SABA)
- Examples: Albuterol, Terbutaline
- Mechanism: Rapid bronchodilation through relaxation of bronchial smooth muscles
- Clinical Use:
- First-line treatment for acute exacerbations
- Rescue medication during maintenance therapy
- Pre-exercise to prevent bronchospasm
Long-Acting Beta-2 Agonists (LABA)
- Examples: Salmeterol, Formoterol
- Mechanism: Sustained bronchodilation (12+ hours)
- Clinical Use:
- Long-term maintenance treatment
- Never used as monotherapy (must be combined with ICS)
Inhaled Corticosteroids (ICS)
- Examples: Budesonide, Fluticasone, Mometasone
- Mechanism: Inhibit inflammatory transcription factors (e.g., NF-κB), reducing airway inflammation
- Clinical Use:
- Cornerstone of long-term maintenance therapy
- Most effective anti-inflammatory medication for asthma
Additional Asthma Medication Classes
Oral Corticosteroids
- Examples: Methylprednisolone, Prednisone
- Mechanism: Potent systemic anti-inflammatory effect
- Clinical Use:
- Severe persistent asthma requiring additional control
- Acute exacerbation management (short courses)
- Reserved for situations where inhaled therapy insufficient
ICS-LABA Combinations
- Examples: Budesonide-formoterol, Fluticasone-salmeterol
- Mechanism: Combined anti-inflammatory and bronchodilatory effects
- Clinical Use:
- Long-term maintenance therapy for persistent asthma
- Budesonide-formoterol may be used as both maintenance and reliever
Leukotriene Receptor Antagonists (LTRAs)
- Examples: Montelukast, Zafirlukast
- Mechanism: Block leukotriene receptors (CysLT1), reducing bronchoconstriction and inflammation
- Clinical Use:
- Exercise-induced asthma
- Aspirin-sensitive asthma
- Maintenance treatment (particularly effective in children)
Medication selection should be individualized based on severity classification, patient age, comorbidities, and response to therapy.
Inhaler Device Selection: A Patient-Centered Approach
Proper inhaler selection is critical for medication effectiveness. Device choice should consider patient age, coordination ability, inspiratory flow rate, and preference.
-
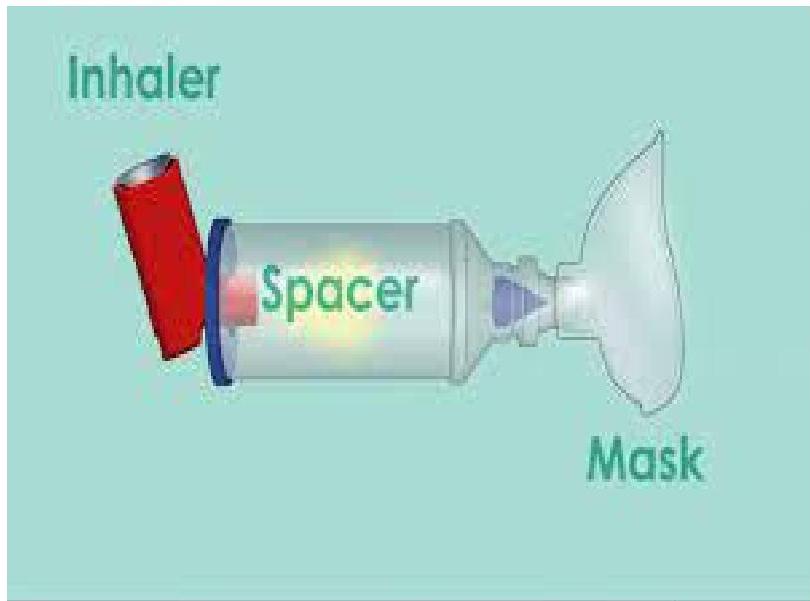
Pressurized Metered Dose Inhaler (pMDI) with Spacer: Suitable for all ages. Spacer improves drug delivery and reduces oropharyngeal deposition. Recommended for children and during acute exacerbations.
-
Breath-Actuated MDI: Eliminates coordination difficulties. Activates when patient inhales. Suitable for patients >5 years with adequate inspiratory flow.

-
Dry Powder Inhaler (DPI): Requires adequate inspiratory flow. No propellants. Generally suitable for children >5 years. Multiple dose types available.
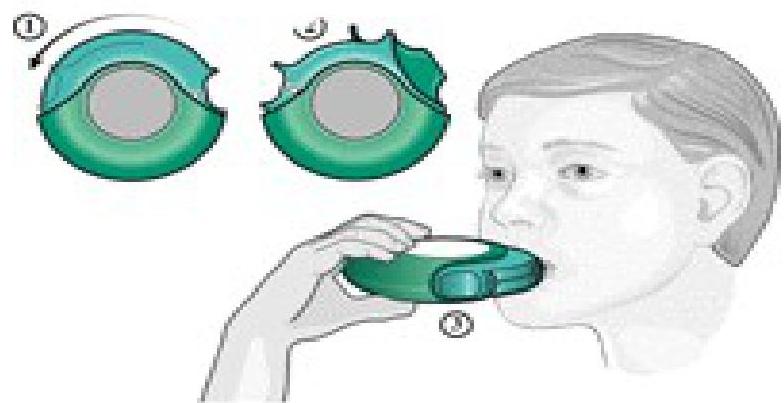 Figure 1: Diskus
Figure 1: Diskus -
Nebulizer: Ideal for very young children, elderly patients, or those unable to use other devices. Useful during severe exacerbations when inspiratory flow is limited.

Stepwise Approach to Asthma Management
Key Principles
- Treatment intensity matches severity classification
- Step up if inadequate control
- Step down after sustained control (3+ months)
- Regularly reassess control and adjust as needed
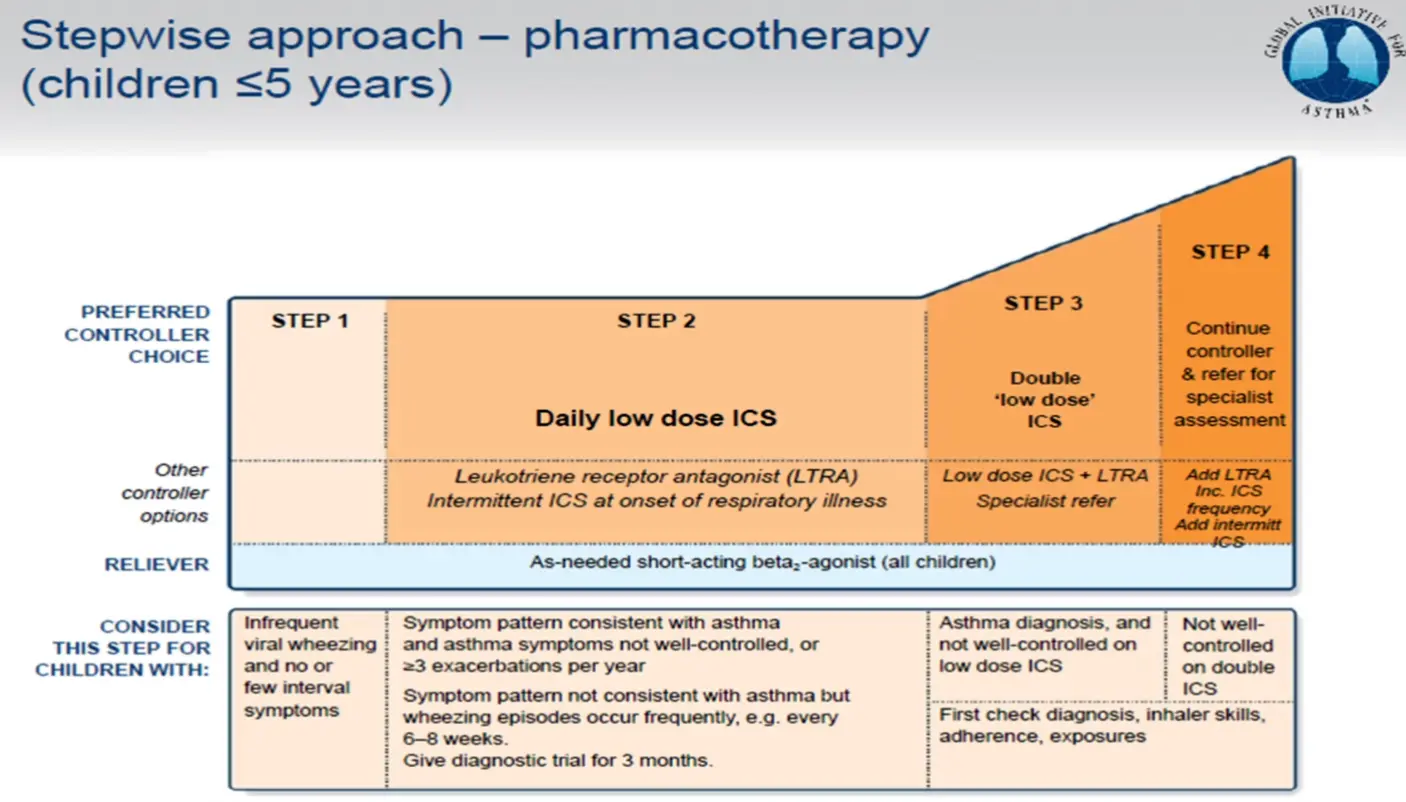
First-Line Controller Therapy
Inhaled corticosteroids (ICS) are the most effective prophylactic therapy for all age groups. They reduce airway inflammation, decreasing symptoms, exacerbation frequency, and bronchial hyperreactivity.
Add-On Therapy by Age Group
- Children >5 years: Long-acting beta-agonist (LABA) is first-choice add-on therapy.
- Children <5 years: Leukotriene receptor antagonist (LTRA) such as montelukast is recommended.
The stepwise approach allows for personalization while maintaining a structured framework for treatment decisions.
Stepwise Approach – Pharmacotherapy (Children ≤5 Years)
Step 1 - 4 Z
Children 6-11 Years
Step 1 Z
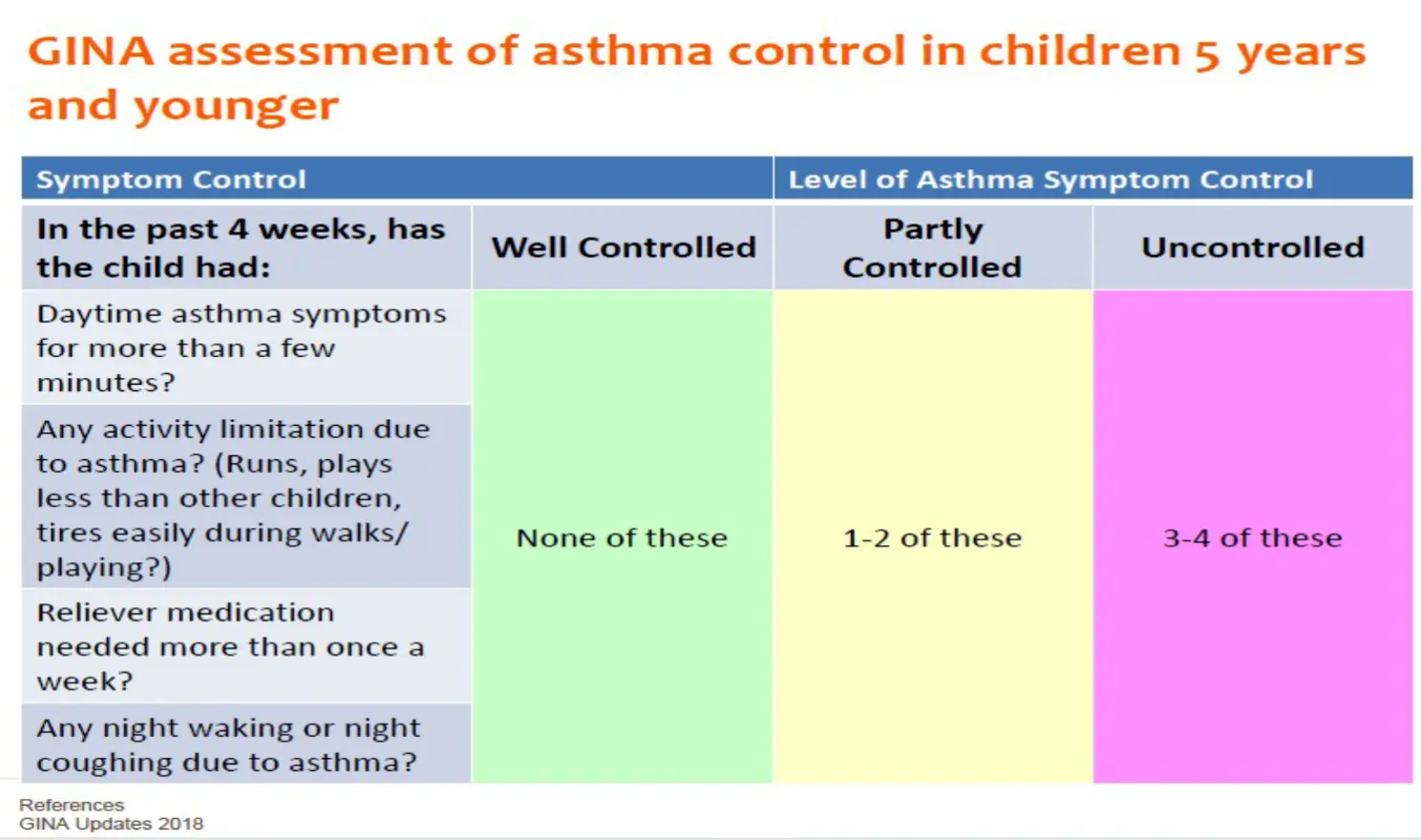
GINA Assessment of Asthma Control in Children 5 Years and Younge
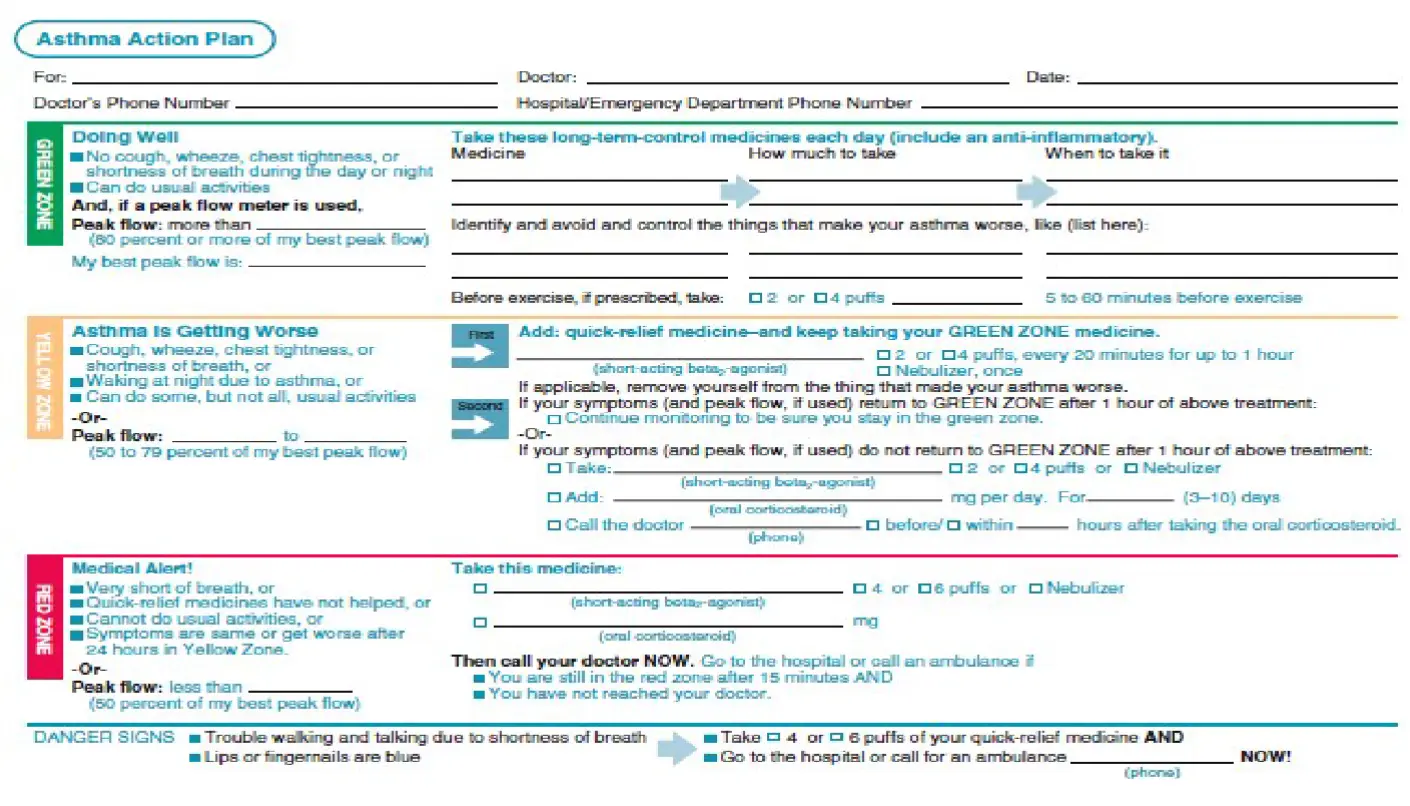
Asthma Action Plan
Personalized Asthma Care: Key Takeaways
Classification Guides Initial Therapy
Accurate severity assessment establishes the foundation for effective management. Classify based on symptom frequency, intensity, and lung function.
Stepwise Approach Enables Personalization
The stepwise framework provides structure while allowing flexibility to tailor treatment to individual needs, comorbidities, and preferences.
Reassessment Drives Adjustment
Regular monitoring of control and risk factors enables timely adjustment of treatment. Step up when needed, but also step down when appropriate.
Patient Education Empowers Self-Management
Effective asthma care requires partnership with patients through comprehensive education, action plans, and shared decision-making.